
Abstract
Health-related social needs (HRSNs), such as food insecurity and housing instability, drive health and well-being. The socioeconomic impacts of the COVID-19 pandemic increased the prevalence of HRSNs and highlighted the critical need for strategies to address those needs, particularly in communities experiencing health disparities. Implementing HRSN screening requires adopting effective strategies to overcome common challenges. This report synthesizes promising implementation approaches and lessons learned from the Accountable Health Communities Model, a national effort funded by the Centers for Medicare & Medicaid Services Innovation Center to systematically screen for and address HRSNs in clinical settings. Key strategies include increasing patient engagement and building trust through culturally tailored language and outreach; using and sharing data for monitoring and improvement; using technology to expand access to screening and referrals; dedicating staff to screening roles; integrating screening into existing workflows; and building buy-in among staff by communicating the impact of screening and encouraging peer connections.
Keywords
Health-related social needs (HRSNs) are key drivers of health, well-being, health care use, and disparities (California Accountable Communities for Health Initiative, 2021; Kelley et al., 2020; Rojas Smith et al., 2020). The socioeconomic impacts of the COVID-19 pandemic increased the prevalence of HRSNs and highlighted the need to address HRSNs to improve health outcomes, particularly in communities experiencing health disparities (Center for on Budget and Policy Priorities, 2021).
The Accountable Health Communities (AHC) Model, funded by the Centers for Medicare & Medicaid Services (CMS) Innovation Center, identified promising practices for implementing HRSN screening and referrals in clinical settings before and during the COVID-19 pandemic. The model supported 28 awardees, including health systems, community-based organizations, academic institutions, health information exchanges, and public health departments, across 21 states in rural, urban, and suburban communities. (Initially, 32 organizations received AHC Model funding, but 4 organizations withdrew during implementation.) Awardees worked with clinical sites at their organization or partner organizations to screen all Medicare and Medicaid patients for five HRSNs: (a) food, (b) housing, (c) interpersonal safety, (d) utilities, and (e) transportation (Billioux et al., 2017; CMS, 2021). All patients with identified needs received referrals. Those who also had two or more emergency department visits in the past 12 months were offered navigation services to connect them with resources. Collectively, awardees screened 1.1 million patients and provided navigation services to more than 137,000 people from May 2017 to June 2022 (Johnson et al., 2022).
This article describes strategies awardees used to overcome implementation challenges and improve screening. It is particularly relevant for hospitals implementing screening in response to CMS’s (2022) rules to promote inpatient screening for HRSNs and given the National Committee for Quality Assurance’s (NCQA, 2022) recent adoption of HRSN screening quality measures.
MethodS
We analyzed quantitative and qualitative data collected from 2018 to 2021 to identify common implementation challenges, capacity-building opportunities, and promising strategies related to HRSN screening.
We reviewed a summary of findings from awardees’ learning needs assessments (LNA). Twenty-nine awardees completed LNAs in April 2019 and May 2020 (96% and 89% response rates, respectively) and 28 awardees completed the LNA in February 2021 (100% response rate. One awardee withdrew from the AHC Model in 2020). The anonymized summary used descriptive statistics to identify elements of screening implementation that awardees ranked as high or moderate learning needs and challenges ranked as top priorities. We identified elements and challenges consistently ranked as learning needs and top priorities across years.
To identify promising strategies to address priority needs and challenges, we reviewed and coded qualitative data, including (a) reports based on semi-structured site visit interviews with 12 awardees, (b) summaries of 16 peer-learning discussions with representatives from all 28 awardees, and (c) a 2020 tracking report of the COVID-19 pandemic’s effect on screening processes and applications of technology for screening for 28 awardees.
LNA responses guided our qualitative coding process; we coded all strategies awardees used to address top learning needs and challenges recorded in the LNA. Specifically, we looked for strategies to address challenges with (a) engaging patients in screening, (b) monitoring and improvement, (c) engaging and retaining staff, and (d) the COVID-19 pandemic. We used thematic analysis to identify common strategies awardees used to address each of these challenges and other promising practices (Braun & Clarke, 2012).
This study was a document review that did not involve human participants; therefore, we did not submit it to an institutional review board. All named organizations approved the inclusion of their practices in this article.
Results
Capacity Building Opportunities for Implementing HRSN Screening
In the LNA summary, awardees consistently identified “engaging patients” as one of the top two learning needs (across the first 3 years of implementation) and “improving screening processes” (during the first 2 years). However, as screening processes matured and the COVID-19 pandemic changed clinic use, additional needs emerged. In 2021, to reflect COVID-19 pandemic circumstances, the LNA included a new option to select “using technology to expand screening and navigation.” This became a top learning need. Table 1 summarizes learning needs across years.
Responses to a Survey Question Asking Awardees to Rank Screening-Related Learning Needs (2019–2021)
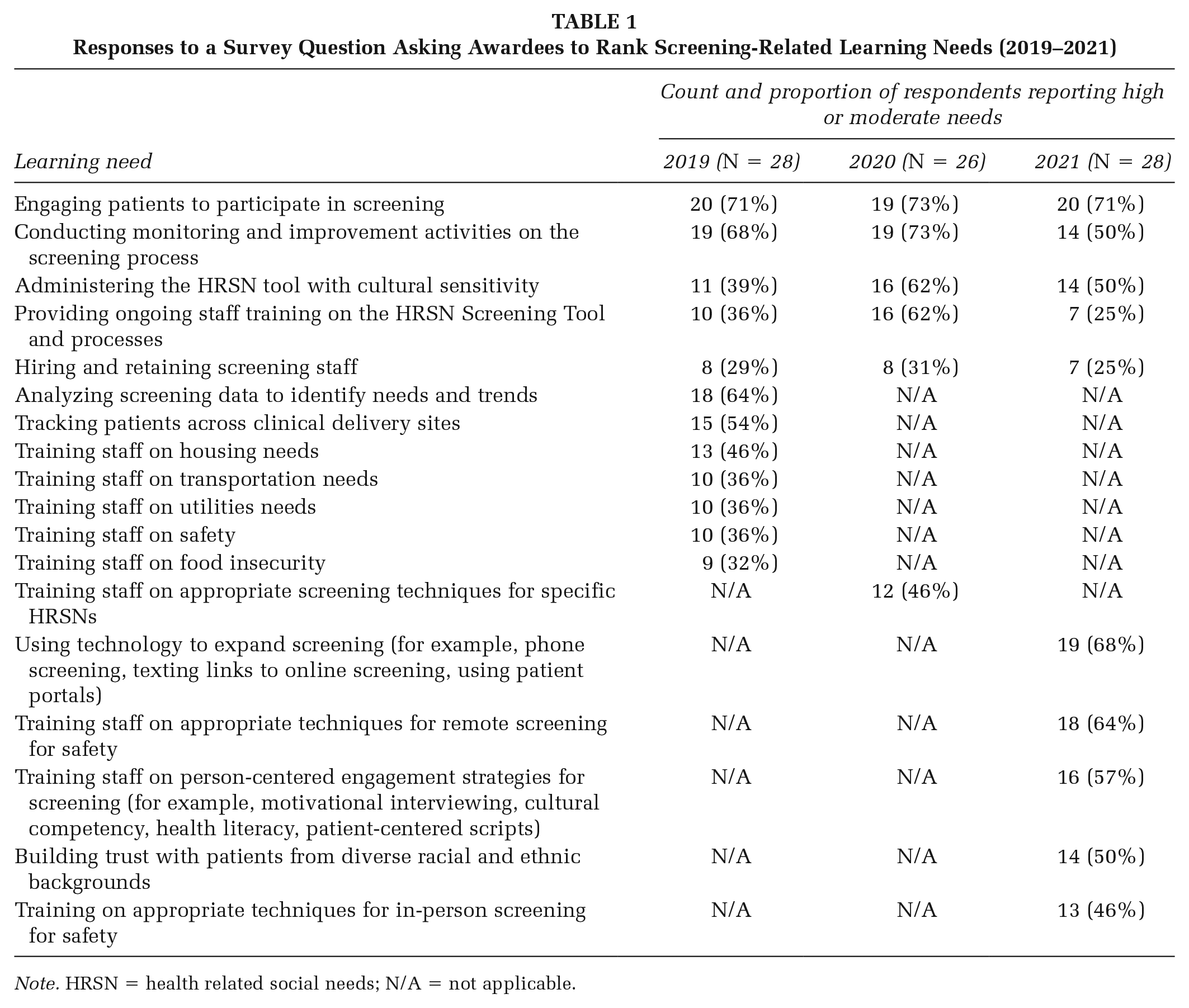
Note. HRSN = health related social needs; N/A = not applicable.
Awardees also identified and ranked challenges in the 2020 and 2021 LNAs. Top challenges included generating buy-in among clinical delivery site staff (2020), insufficient staff time for screening (2020 and 2021), and low patient volume at clinical sites because of the COVID-19 pandemic (2021). Table 2 summarizes key challenges.
Responses to a Survey Question About Awardees’ Challenges With Health-Related Social Needs Screening (2020–2021)
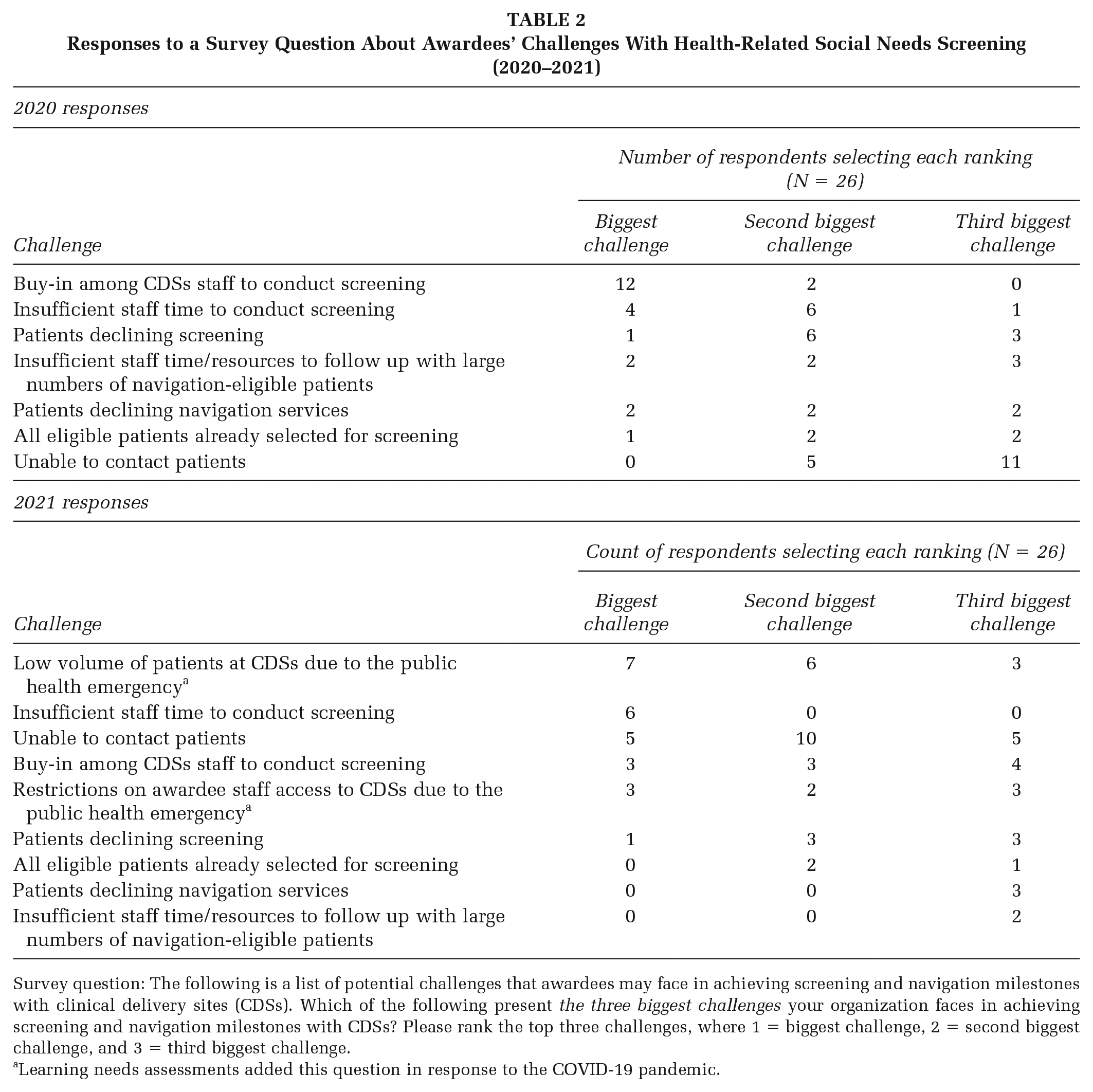
Survey question: The following is a list of potential challenges that awardees may face in achieving screening and navigation milestones with clinical delivery sites (CDSs). Which of the following present the three biggest challenges your organization faces in achieving screening and navigation milestones with CDSs? Please rank the top three challenges, where 1 = biggest challenge, 2 = second biggest challenge, and 3 = third biggest challenge.
Learning needs assessments added this question in response to the COVID-19 pandemic.
Promising Strategies to Improve HRSN Screening Implementation
Building trust through culturally tailored language and screening approaches increases patient engagement in screening
Awardees stressed the importance of building trust with patients—for example, by using personalized scripts to introduce HRSN screening and building rapport with patients. Several awardees noted the importance of helping staff adapt screening scripts to reflect their personalities, which made staff feel comfortable delivering the information and patients more receptive. Awardees also found that patients perceived staff who reflected the community’s cultural composition and who wore casual attire as more approachable, which increased patients’ comfort with screening.
Other awardees discussed adapting scripts based on patients’ needs. For example, New York-Presbyterian Hospital used interpretation tools to deliver its script in multiple languages and created an audible version of the script for patients with limited literacy. Reading Hospital-led journey-mapping exercises and focus groups with community-based organizations serving older adults to learn how to best reach patients over age 64. It found the words “help” and “need” provoked concerns about losing independence, while patients reacted positively to “entitlement” and “support.” Reading Hospital used this information to adapt its scripts and found a slight increase in screening and navigation rates for patients ages 65 and older.
Using and sharing performance data for HRSN screening supports monitoring and improvement
Awardees shared data on HRSN screening rates with clinical sites in dashboards or visual report formats. These data helped identify sites that were performing well, or that needed improvement, and sparked conversations about challenges, strategies, and successes. Awardees also used data to inform specific quality improvement efforts. For example, Oregon Health and Sciences University (OHSU) tracked text-message screening responses to identify the times of the day when patients were most likely to engage, and what language was associated with the most opened texts and completed screenings. Texts that referenced “social needs” and sent either before 9 a.m. or after 3 p.m. were most likely to be opened.
Novel technologic approaches expanded screening during the COVID-19 pandemic
All 28 awardees reported switching to telephonic screening when the COVID-19 pandemic necessitated changes to screening workflows. Because engaging patients by telephone was often challenging, some awardees explored additional modalities for reaching patients. Six awardees used technology—such as texts, patient portals, and emails—to link patients to a secure online version of the AHC HRSN Screening Tool, thereby expanding screening opportunities.
Texting
Two awardees set up systems to deliver text messages to patients that linked to the AHC HRSN Screening Tool. OHSU sent automated text messages to patients during or after clinical visits, reviewed results, shared relevant community resources by text, and followed up with patients eligible for navigation services by phone or text. MyHealth Access Network, a health information exchange (HIE) that used texting as its only screening modality throughout AHC implementation, delivered real-time text messages to patients during clinical visits and captured results in the HIE. MyHealth Access Network noted the value of working within Federal Communications Commission guidelines to ensure cellular companies do not block texts and obtaining a short code for the project to reduce the number of blocked messages.
Patient Portals
Three awardees added fields to online patient portals (such as MyChart) with an introduction and secure link to the HRSN Screening Tool. These awardees combined the screening link with pre- or post-visit materials in patient portals for in-person and telemedicine visits. Some organizations also generated electronic messages to alert patients to complete HRSN screening.
Email Campaigns
Although only one awardee, Denver Regional Council of Governments (DRCOG), delivered HRSN screening via email, its email campaign increased screening rates dramatically, with 431 patients completing screening in the first 2 months of the campaign. DRCOG noted the importance of crafting an email that integrates familiar logos and includes the provider’s name to build trust. DRCOG pilot-tested the campaign and sent emails in small batches to match staff capacity and ensure patients received timely follow up to their screening.
Having dedicated screener roles and integrating screening into existing workflows can increase efficiency and staff time for screening
Although staffing models varied widely, many clinical sites assigned screening to existing reception or registration staff who had other responsibilities and little time to dedicate to screening. To address these competing priorities, several awardees added staff dedicated solely to screening, sometimes in combination with navigation responsibilities. Three awardees developed credit-earning internships for local college or graduate students to administer HRSN screening. However, one challenge of this approach was difficulty finding coverage during school breaks.
Ensuring that HRSN screening fits within existing clinical workflows was another important strategy for maximizing efficiency. Several awardees collaborated with staff at clinical sites to develop or tailor screening approaches that staff could incorporate into processes like registration, triage, or discharge.
Communicating the impact of HRSN screening and creating mechanisms for team connections supported staff buy-in
Many awardees built staff buy-in for HRSN screening by demonstrating how their work improves patients’ health outcomes and well-being. Awardees used two primary strategies to achieve this goal: (1) training staff on social determinants of health, and (2) collecting and sharing patient testimonials and success stories, including through mediums such as videos and newsletters.
Another common strategy for encouraging staff buy-in was to provide opportunities for peer connections and collaboration. Approaches to fostering connection included conducting regular site visits to support staff, discuss performance, and answer questions; hosting regular meetings with staff from multiple clinical delivery sites to share challenges and promising practices; and distributing monthly newsletters or emails showcasing screening tips and successes. Awardees reported that these strategies motivated staff to conduct screenings; one awardee noted consistent upticks in screening rates following quarterly cross-site meetings.
Discussion
Implications for Practice
New CMS (2022) rules in 2022 increased the need for HRSN screening best practices (NCQA, 2022). Our national cross-site findings highlight strategies for addressing common HRSN screening challenges, such as generating staff buy-in, gaining patient trust, and improving screening processes. This work expands the evidence for promising practices and can inform wider implementation of HRSN screening in clinical settings (Buitron de la Vega et al., 2019; Davidson & McGinn, 2019; Kaiser Permanente Center for Health Research & OCHIN, 2022). It demonstrates that regular communication, connection, and support are critical for gaining staff buy-in. Our results highlight the importance of centering patients throughout the implementation of a screening program and show how personalizing and refining scripts based on patient feedback helps build trust and rapport. Our work also identifies strategies for using technology, such as texting and email, to expand and streamline HRSN screening processes. Although the AHC Model focused on Medicare and Medicaid patients, these findings can apply to screenings with other populations.
Limitations
We were not able to directly measure the impact of implementation strategies on screening rates. Our document review relied on summary documents that represent the efforts of several awardees. However, because we did not systematically ask all awardees about their efforts to address key challenges, this review might miss some implementation strategies.
Conclusion
Screening for HRSNs and making referrals can help address the root causes of poor health (Castrucci & Auerbach, 2019), but these activities are only part of the solution. Many health care and public health organizations are working with their communities to assess and ensure the availability and quality of resources to meet residents’ social needs. These organizations can also consider upstream interventions to improve community conditions and address the systemic and structural determinants of health. Developing and maintaining the infrastructure and workforce capacity to do so will also require sustainable value-based payments and collaboration between payers, providers, and communities (National Academies of Sciences, Engineering, and Medicine, 2019).
Footnotes
Authors’ Note:
We would like to thank the AHC Model staff and awardees, whose work we have described in this publication, including Tanieka Mason (Reading Hospital), Anne King (Oregon Health and Science University), Jennifer Faries and Dr. David Kendrick (MyHealth Access), Dr. Dodi Meyer (New York-Presbyterian Hospital), and A.J. Diamontopoulos (Denver Regional Council of Governments). We would also like to thank Katherine Verlander for her review and feedback on this manuscript. Funding provided by Centers for Medicare & Medicaid Services, Contract [HHSM-500-2014-00034I].