
Abstract
Objectives:
Endometrial cancer incidence and mortality disproportionately affect Black patients, and delayed diagnosis is a contributor. Providers in multiple settings share the task of endometrial cancer diagnosis. The purpose of this study is to elicit physician perspectives on national guidelines for the diagnosis of endometrial cancer (EC), understanding of racial disparities in EC, and to explore physician receptivity to a risk-based, endometrial biopsy (EMB)-first approach of peri/postmenopausal bleeding.
Methods:
We performed semi-structured interviews with 12 U.S. physicians across multiple specialties. Interview structure was developed and refined using an iterative process. We used inductive reasoning to employ exploratory content analysis.
Results:
We interviewed OB/Gyn (n = 4), family medicine (n = 3), internal medicine n = 3), and emergency medicine (n = 2) physicians in all regions of the U.S. Slightly over half (58%) performed EMB. Most (58%) were uncertain about guidelines for diagnosis. Nearly half (42%) reported lack of knowledge regarding racial disparities in EC diagnosis and cancer outcomes. OB/Gyn physicians were skeptical of guideline efficacy in high-risk patients, including patients identifying as Black. Most (75%) physicians supported a risk-based, biopsy-first approach to diagnosis of EC.
Conclusions:
Physicians caring for patients at risk for EC lack knowledge of current guidelines and of racial disparities in endometrial cancer diagnosis and outcomes. A multi-pronged approach, incorporating changes to national guidelines and targeted provider education, is necessary to eliminate inequities in diagnosis of EC.
Introduction
Endometrial cancer (EC) has the fastest increasing mortality rate for any cancer that affects females. 1 It is the most common gynecologic cancer in the United States (U.S.) and has overtaken ovarian cancer as the deadliest gynecologic cancer in this country.2 -4 Black patients in the U.S. suffer a 2-fold higher mortality rate from EC when compared to their White counterparts; this gap is increasing over time.5 -9 Delays in diagnosis and advanced stage at diagnosis are modifiable factors tied to prognosis among Black patients.3,10,11
Efficient diagnosis is crucial to identify patients with endometrial cancer at early stages, yet the path to reach a diagnosis presents challenges. Providers of multiple specialties—family medicine, internal medicine, obstetrics and gynecology (OB/Gyn), and emergency medicine—share the task of diagnosing endometrial cancer in a diverse range of practice settings.12 -17 Additionally, national guidelines for the diagnosis of endometrial cancer currently emphasize ultrasound as an acceptable first step in the diagnostic evaluation of peri/post-menopausal bleeding (PPMB), despite emerging evidence of inferior efficacy of ultrasound as a diagnostic modality in diverse patient populations.15,16,18 -22 A guideline-concordant, ultrasound-first approach does not perform equitably among Black patients, those with aggressive histologic subtypes of EC, or those with fibroid uteri.19,21 -24 Providers following these guidelines are poised to contribute to disparate outcomes for these high-risk patients.
Data surrounding provider knowledge and practice patterns in the diagnosis of endometrial cancer is lacking. In a cross-sectional survey of providers across the U.S., we highlighted knowledge gaps and demonstrated that providers with improved understanding of endometrial cancer are more likely to choose guideline-concordant care; other available retrospective analyses have found that roughly half of postmenopausal patients with bleeding receive guideline-concordant care.25,26 It is unclear whether providers on the front line for evaluation of EC have been reached by emerging evidence documenting inferior diagnostic outcomes for Black patients. To build on prior quantitative work, we aimed to elicit physician understanding and opinions on current guidelines for diagnosis of EC, to ascertain physician perceptions of racial disparities in EC, and to assess acceptability of a risk-based biopsy first approach to EC.
Methods
This qualitative study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. It was reviewed by the institutional review board of our institution as part of the Guidelines for transvaginal Ultrasound In the Detection of Early Endometrial Cancer (GUIDE-EC) study and was deemed exempt. Participants provided verbal consent to participate in the study and received a $100 gift card.
We recruited a sample of OB/Gyn, family medicine, internal medicine, and emergency medicine physicians who care for adult patients with uteri from July 2023 to February 2024. Physicians were recruited from academic and community settings, with both inpatient and outpatient practice bases. Recruitment occurred using professional networks via snowball sampling. Our target population size was 12 interview participants to reach thematic saturation.27,28
An interview guide was developed addressing 5 main content areas: understanding/opinion of current guidelines, evaluation/counseling processes, opinions on racial disparities in endometrial cancer, opinions on a risk-based, endometrial biopsy (EMB)-first approach to the diagnosis of EC. Semi-structured interviews were conducted with primarily open-ended questions (e.g., “Can you describe your understanding of current guidelines?”). Demographic data included physician’s specialty, role in women’s healthcare, practice setting, practice location, and scope of clinical services.
The interview guide was refined through an iterative process with several team researchers, including clinicians and research scientists. The interview was piloted with a family medicine physician; the results of this pilot interview were further utilized to refine the guide and were included in the final analysis. Three authors conducted and recorded interviews via Zoom or telephone. Interviews lasted between 30-60 minutes and were transcribed verbatim, verified against the recordings, and de-identified.
Analysis
Analysis of all interviews was conducted by 2 authors. We conducted exploratory descriptive content analysis, first creating a codebook through an iterative process using an inductive reasoning framework. Using question content areas as a loose structure, 2 interviews (16.7%) were double-coded using open inductive consensus coding to refine the codebook.
The remaining 10 interviews were coded via split-coding using an iterative process, with new themes incorporated into the existing codebook. For each transcript, the primary coder used memos to create case summaries. Key quotes were collected from each interview. The coders utilized consensus coding for any questions or concerns regarding interview interpretation. All coding was performed using Dedoose software, version 9. 29 Data collection was performed from July 2023 to February 2024. Analysis was conducted from January 2024 to March 2024.
Results
Physician Demographics
A total of 12 interviews were conducted with 4 OB/Gyn physicians, 3 family medicine physicians, 3 internal medicine physicians, and 2 emergency medicine physicians. Physicians were purposefully sampled from locations with higher proportions of Black residents but covered all 4 regions of the United States: South (n = 6, 50%), West (n = 4, 33%), Northeast (n = 1, 8%), and Midwest (n = 1, 8%). 30 Practice settings included academic and community settings, centralized medical systems (e.g., Veterans Healthcare Administration (VA), Kaiser Permanente), federally qualified health centers, urban and rural practice settings. While most (n = 7, 58%) physicians performed EMB, no emergency medicine physicians performed EMB as part of their practice (Table 1).
Physician Demographics.

Region designation utilizes the CDC definitions of regions of the United States.
Approach to Care
In evaluating patients with PPMB, most physicians individualized the components of their approach, using history and physical exam to guide steps. Pelvic ultrasound or EMB were often the first diagnostic test performed, however one OB/Gyn physician endorsed a distinct approach, prioritizing direct visualization of the endometrium, always utilizing hysteroscopy. Physicians variably utilized endometrial thickness on ultrasound to guide next steps. While for some physicians, an endometrial thickness <4 mm was reassuring and allowed for observation, others recommended tissue sampling for all patients with PPMB.
Physicians preferred clear and concise delivery of information to enhance counseling, tailoring counseling to meet patient knowledge levels and goals of care. Discussion of cancer was variable; while some preferred to avoid naming cancer, others prioritized raising awareness of possible malignancy. Addressing pain associated with EMB was seen as a key, and under-utilized, component of preparing patients for the procedure.
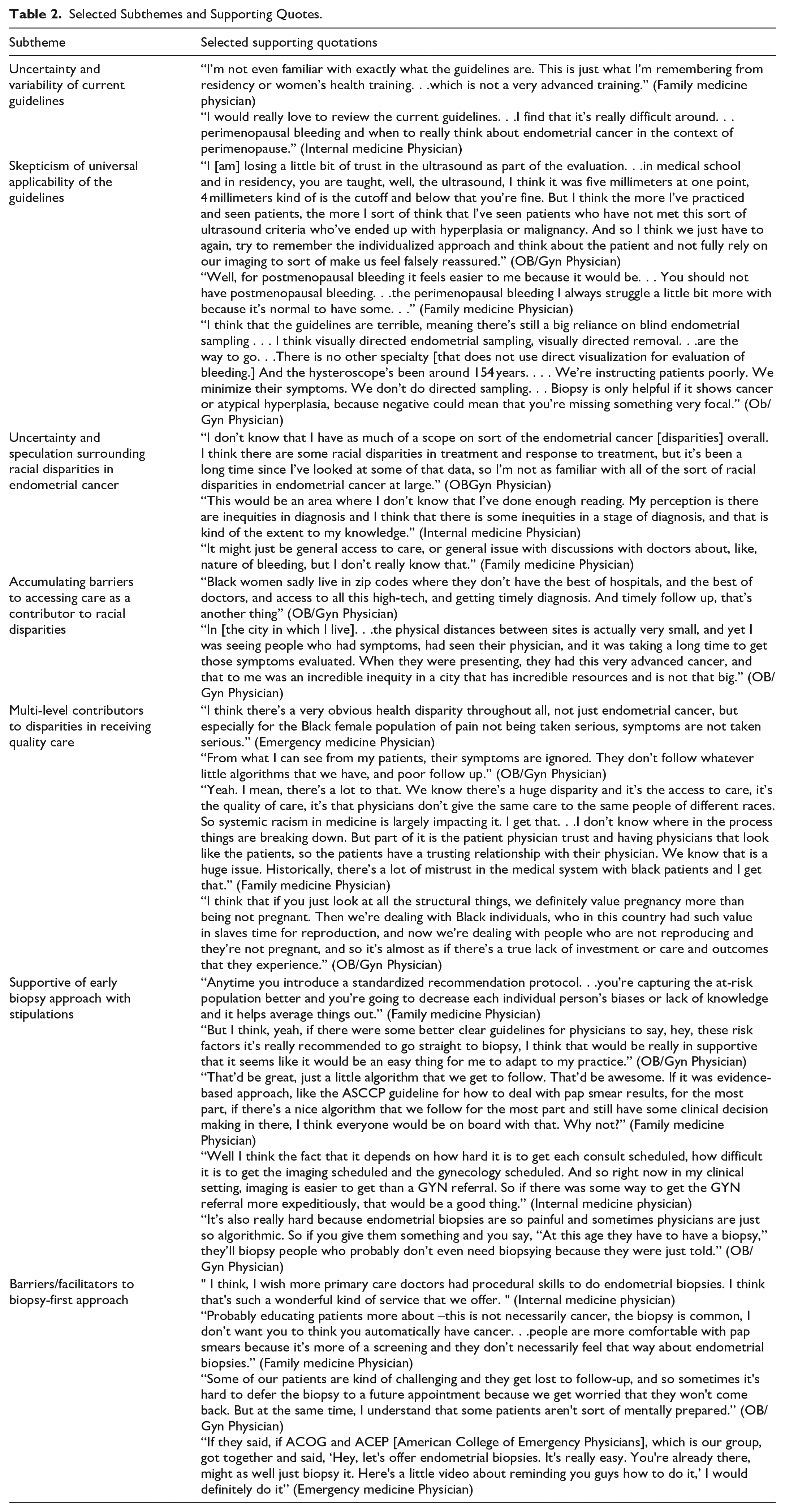
Qualitative analysis covered 3 major content areas: physician opinions on and interpretations of current guidelines, perceptions of racial disparities in endometrial cancer, and opinions on ultrasound versus tissue-sampling for the evaluation of PPMB. Patient experience was an integral theme that influenced physician answers in all content areas. Selected quotes supporting findings are summarized in Table 2.
Selected Subthemes and Supporting Quotes.
Theme 1: Current Guidelines
In discussing guidelines for diagnosis of EC, themes emerged of uncertainty, variable perceived importance of guidelines, and skepticism of universal applicability.
Uncertainty and Variability
The majority of non-OB/Gyn physicians (n = 7, 87%) reported uncertainty regarding current guidelines for the evaluation of PPMB. This included the correct order of operation of diagnostic steps, which diagnostic modalities to select, and which endometrial thickness cutoff on ultrasound should trigger endometrial tissue sampling. Despite these uncertainties, most did not routinely reference guidelines during their evaluation, but viewed their role as obtaining the most information possible prior to referring to OB/Gyn. For some physicians, this meant obtaining both an ultrasound and biopsy at the same time, while for others it meant referring immediately to OB/Gyn. One emergency medicine physician stated, “Honestly, I haven’t looked at [the] ACOG guidelines in quite some time. . .the red flag if postmenopausal bleeding and we refer on.” All OB/Gyn physicians referenced the American College of Obstetricians and Gynecologists (ACOG) guidelines as the standard of care.
The relative importance of national guidelines varied among physicians depending on their institutional setting. Physicians working at centralized health systems (e.g., VA) or in the emergency room prioritized use of institutional guidelines over guidelines from national societies.
Skepticism of Universal Applicability
Physicians knowledgeable about nationally available guidelines expressed concern that they were not effective in all groups of patients. Physicians of all specialties reported more uncertainty in evaluating perimenopausal, versus postmenopausal, patients. All OB/Gyn physicians stated that the guidelines for ultrasound in the evaluation of PPMB were not effective for Black patients or those with high-risk endometrial cancers. One OB/Gyn summarized, “There is a reasonable body of literature that suggests that the ultrasound thickness that is sort of recommended by ACOG may not perform equitably amongst different cohorts of patients, namely white individuals with uteri versus Black individuals with uteri.”
Due to the lack of clarity in perimenopausal patients and lack of efficacy in high-risk patients, the guidelines were viewed as insufficient for informed physicians.
Theme 2: Racial Disparities in Endometrial Cancer
Uncertainty and speculation regarding racial disparities in EC—both in diagnosis and outcomes—were major themes. Among physicians with knowledge, a theme of multi-level contributors to racial disparities emerged.
Uncertainty and Speculation
Nearly half of physicians (n = 5, 42%) reported a lack of firm knowledge regarding racial disparities in endometrial cancer diagnosis. Many of these physicians offered speculated potential contributors. One internal medicine physician stated:
I actually don’t know the data around racial disparities in endometrial cancer. I would imagine there are probably some barriers with. . .priorities or patient’s willingness to, number one, bring up concerns about this and comfort with discussing with their physicians their concerns about their gynecologic health and maybe some different kind of positive beliefs around cancer detection and treatment.
Speculated contributors to endometrial cancer disparities in diagnosis were heavily weighted towards patient-level factors, with a minority focusing on physician-level or systems-level issues such as access to care.
Half of all physicians (n = 6, 50%) reported sufficient knowledge to discuss racial disparities in EC outcomes. Internal medicine, family medicine, and emergency medicine physicians were less likely to endorse knowledge of racial disparities in EC compared to OB/Gyn physicians.
Accumulating Barriers to Accessing Care
Among physicians with knowledge of racial disparities in EC, decreased access to care was the most frequently mentioned contributor. Delayed symptom disclosure was frequently mentioned as a contributor to delay in accessing care. This was thought to stem from a combination of misinterpretation of symptoms as not bothersome as well as a history of normalization of bleeding by physicians throughout the reproductive life cycle. One OB/Gyn physician summarized,
I’ve heard a lot from Black women who I’ve diagnosed with uterine cancer. . .that they had irregular bleeding their whole life. . .when they got to the end of their reproductive cycle or lifespan, their bleeding was irregular again, but it felt similar to everything they had in their life and so they didn’t know that it was abnormal because probably we never as a medical profession listened enough earlier.
Two physicians mentioned that low rates of Black physicians, leading to physician-patient race discordance, added another hurdle for accessing care. Medical distrust also contributed to delayed reporting of symptoms and decreased access.
Finally, community- and systems-level factors contributed to access barriers for Black patients. Neighborhood/place of residence and distance to reach care were seen as access barriers, with one emergency medicine physician stating, “I would say generally that my concern is that access to care falls on racial and economic boundaries, and also other access problems to care, and mobility issues. . .my thought is that any barrier to care is a problem.” Barriers accumulated on multiple levels to make care access more challenging for Black patients with EC.
Multi-Level Contributors to Disparities in Receiving Quality Care
Physician and health systems factors were seen as important contributors to racial disparities in EC diagnosis after accessing care. Physicians felt that Black patients with PPMB were not listened to adequately in healthcare settings, and that physicians normalized worrisome symptoms. Multiple physicians named medical racism as a contributor to equitable diagnosis of endometrial cancer, with one family medicine physician stating, “One [factor] would be access to care and being taken seriously, and racism in the healthcare system that may make accessing the care or not being heard more challenging.” Lack of adequate follow-up after initial presentation was another contributor to timely diagnosis for Black patients. Ultrasound was again mentioned by OB/Gyn physicians as a systems-level factor contributing to disparities in diagnosis for Black patients:
Ultrasonography [is] not really very accurate in Black women. It’s been shown to perform really poorly compared to white women. . .[while] there are guidelines, there are algorithms for a lot of things we do in medicine. . .you have to think about each individual patient and their unique history, their unique scenario, and also how they feel about it and what they choose in their journey for their healthcare.
Poor prognosis amongst Black patients with EC was viewed as multifactorial. Advanced stage at diagnosis and increased prevalence of aggressive histologic subtypes of endometrial cancer were cited as important factors contributing to worse outcomes among Black patients. Increased time to access oncologic care was also thought to contribute to advanced stage at diagnosis and poor prognosis. Physicians again felt that Black patients in the United States, specifically when not pregnant, were systematically devalued, leading to poor quality of care once diagnosed.
From before symptom presentation through reaching a diagnosis, physicians with knowledge of EC disparities acknowledged contributing factors at the patient, physician, and systems levels.
Theme 3: Risk-Based Approach
In discussing a potential risk-based approach to EC diagnosis with early biopsy/tissue-sampling prioritized for patients at higher risk of cancer, themes emerged of general support for early tissue sampling, with hesitation from some physicians.
Supportive of Early Biopsy with Stipulations
Most (n = 9, 75%) physicians supported a risk-based approach to evaluation of PPMB, with some physicians (n = 2, 17%) expressing insufficient knowledge to endorse an opinion. Physicians were in favor of incorporating evidence-based practices into their approach and appreciated standardized recommendations for care. Physicians felt that scheduling ultrasound was challenging and created bottlenecks to care, in addition to having lower efficacy in high risk patients. By moving directly towards endometrial sampling, physicians expected reduced care access barriers and improved accuracy of diagnostic pathways.
Several disadvantages and potential pitfalls noted by physicians in implementing a risk-based approach to EC diagnosis emerged. One OB/Gyn physician felt that EMB was inadequate, and endorsed directed sampling with endometrial visualization for all patients (Table 2). Other physicians expressed concern about over-reliance on algorithms in medical decision making, potentially resulting in over-sampling patients with ultimately benign disease: “I think the potential harms would be, overall, the majority of diagnoses are going to be non-cancerous, so there would be a potential risk of getting. . .I guess risk of not getting the cancer diagnosis” (OB/Gyn Physician). Another physician voiced concern over implementing a race-based approach which would not allow for individualization in the diagnostic process. Physicians not able to perform EMB were concerned that they would no longer have a meaningful role in the evaluation of PPMB, leading to higher rates of early referral to OB/Gyn. Finally, some physicians mentioned inherent risks of procedures, increased pain with EMB compared to ultrasound, and unnecessary worry for patients with benign disease.
Barriers and Facilitators to Biopsy-First Approach
Facilitator to adoption of a risk-based, biopsy-first approach included robust information dissemination with educational campaigns and clear algorithms to guide decision-making: “I think that whenever there are changes in guidelines, it’s really helpful to have some kind of educational component. . .Implementation is really difficult and changing practice is really difficult” (IM Physician). Multiple physicians felt that dissemination of a new approach would be enhanced by embedding decision-making tools into the electronic medical record.
Expanding the proportion of physicians who perform EMB was seen as another needed component to successful adoption. Physician discomfort or inability to perform EMB re-emerged as a barrier, despite previous procedure-specific training. Physicians seemed willing and interested in expanding their skillset to incorporate EMB, if structural factors allowed. At the systems level, clinic structure and time constraints were viewed as a barrier, with inflexible scheduling often precluding same-day biopsy for eligible patients.
Patient-level factors which were perceived as potential barriers to implementing this approach included adequate pain control and balancing acceptability of same-day biopsy with hassle of returning to clinic for additional visits. Physicians felt that enhanced counseling, including rationale and implications of a biopsy, as well as options for pain control, would be important for patient acceptability. Offering extra visits via telehealth prior to biopsy to provide thorough counseling was one proposed solution. Loss of patients to follow-up, especially when needing to return for a separate visit to undergo biopsy, was another barrier to successful implementation of this approach.
Discussion
Black patients with EC continue to suffer from advanced stage at diagnosis and increased mortality once diagnosed.3,8,9,11,23,31,32 A growing body of evidence demonstrates that current guidelines for use of transvaginal ultrasound do not perform equitably amongst black patients and may be contributing to inferior oncologic outcomes for this vulnerable population.19 -24,33 National guidelines and professional societies have not shifted in their recommendation of either ultrasound or endometrial tissue sampling as acceptable first line tests for patients with PPMB.14 -16,34 Despite publications on endometrial cancer disparities in the mainstream media, little is known regarding whether new data is reaching physicians and being incorporated into practice. 35
In our study, the majority of physicians were supportive of incorporation of a risk-based, biopsy-first approach to the diagnosis of EC, emphasizing the need for education and dissemination of guidelines at the patient, physician, and systems level in order to be successful. Physicians also preferred an individualized, patient-centered approach with centering of pain management for procedures as key for successful adoption. Potential barriers of successful implementation included fear and distrust of the medical system, systems-level factors such as requiring multiple visits to reach a diagnosis, and lack of physicians equipped to perform in-office biopsy.
Previous literature has suggested that physicians have poor adherence to guidelines for evaluation of PPMB. In a survey-based study investigating knowledge and practice patterns, 13% of physicians chose guideline non-adherent next-steps in the evaluation of postmenopausal bleeding, and only 36% began with tissue sampling. 25 Additionally, 25% of physicians supported the unproven idea that Black patients respond to cancer treatment differently due to genetic makeup. 25 A retrospective study of women’s health care provision at the VA found that only 53% of patients in the VA system with abnormal uterine bleeding receive guideline-adherent care. 26 Less than half (46%) of surveyed postmenopausal patients had ever received anticipatory counseling from their physicians regarding postmenopausal bleeding. 36 These initial studies paint a picture of a need for widespread education and targeting at the physician level to improve diagnostic efficacy.
This study is the first qualitative study to investigate physician practice patterns, knowledge of EC racial disparities, and to explore a potential path toward alternative diagnostic pathways. We have highlighted that physicians currently on the frontline for evaluation of PPMB have not been adequately reached by existing published literature documenting decreased efficacy of ultrasound in Black patients. Physicians in all specialties reported lack of knowledge of racial disparities in EC broadly, with only OB/Gyn physicians reporting diminished trust in ultrasound as a diagnostic modality in Black and other high-risk patients. This finding is not surprising; for physicians seeing patients of all sexes and ages with the full spectrum of chief complaints, adopting the findings of primary literature which has not been incorporated into guidelines or institutional educational materials is unrealistic.
Strengths of this study include a broad physician sample, encompassing the majority of specialties which care for patients with PPMB in the front-line setting. Specifically, inclusion of physicians working in settings not traditionally seen as women’s health-specific is a strength of the study; previous quantitative and qualitative research has emphasized the importance of these clinical settings for the reporting of abnormal uterine bleeding, including postmenopausal bleeding.12,13,17,37 -39 Our qualitative study, in addition to these prior works, highlights the need for more robust education of these providers as well as systems-based changes to improve care delivery in these settings. 25 Our sample size was sufficiently large to reach thematic saturation and allowed us to explore differences between specialties. Physicians were over-sampled from the South to reach physicians more likely to care for Black patients. A limitation of this study is that it was limited to physicians and did not include advanced care providers (APPs); previous studies have demonstrated similar knowledge levels of endometrial cancer among primary care APPs and physicians. 25 There are additional known barriers involved in the evaluation of postmenopausal bleeding, such as symptoms recognition and counseling, access to ultrasound services, and cost associated with undergoing the evaluation.11,26,40 -42 Addressing all of these, in addition to the focus of this manuscript—provider knowledge and practice patterns—are important to improving timely EC diagnosis.
Conclusions
This study highlights a widespread lack of knowledge regarding current guidelines for the evaluation of PPMB and of racial disparities in EC. As EC has become the deadliest gynecologic cancer in the United States, we must arm our physicians with the skills and knowledge required to eliminate increased mortality for Black patients. We continue to advocate for a more equitable approach to diagnosis of EC among vulnerable populations and call for bringing tissue sampling to the forefront, in light of evidence demonstrating inferior efficacy of ultrasound in this population. We demonstrate that the majority of physicians are supportive of this approach and seem willing to expand their clinical skillsets to accommodate such a shift.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Kuni Discovery Grants for Cancer Research: Advancing Innovation. The sponsor had no role in study design, collection, analysis, and interpretation of data, writing of the report, nor the decision to submit the report for publication. This work is supported by the NIH Ruth L. Kirschstein National Research Service Award, T32CA0009515. Dr. Robinson was also funded from NIH R01 MD011680.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.