
Abstract
Introduction/Objective:
This study evaluates 4 years of data from the Seattle One Health Clinic (OHC), a novel model for clinical care which integrates human and animal health care services for youth and young adults experiencing homelessness (YPEH) and their pets.
Methods:
We analyzed deidentified data from standardized OHC visit forms, electronic medical records, and veterinary records from 2019 to 2022. We assessed the overlaps between human and animal healthcare provided and the impact of environmental stressors on both human and animal patients.
Results:
Over 50% of all human clients established healthcare for the first time in 2 years, with 85% attending one or more follow-up appointments with non-emergency healthcare services within 2 years following their initial OHC appointment. All animals received care during their visit. Needs addressed at the human-animal interface included zoonotic infections, animal allergies, and mental/behavioral health. The most common client-pet reported environmental concerns were food insecurity, heat, and cold.
Conclusion:
Our results suggest integrated human and animal healthcare is a feasible and acceptable model of care for YPEH to access acute and preventative care at the human-animal-environmental interface. This approach holds promise for increasing health-seeking behaviors, and engagement in preventative, therapeutic, and follow-up care.
Introduction/Objectives
Young Experiencing Homelessness in the United States and King County and the Benefits of the Human-Animal Bond
In 2023, there were over 34 700 unaccompanied young people experiencing homelessness (YPEH) counted in the United States (U.S.). 1 Unaccompanied YPEH are those 18 to 25 years of age without the accompaniment or care of a parent or legal guardian.1,2 In Washington State during 2023, 2026 YPEH were counted, with 58% (1177) residing in Seattle-King County. 1 Of the YPEH in King County, 66.1% were unsheltered: one of the highest rates in the nation. 1 Youth and young adult unhoused status are a result of complex issues distinct from adults, such as familial conflict, inadequate support from parent(s) or legal guardians, and abuse. 2 Experiences of trauma, structural oppression or marginalization of gender and sexual minorities, 3 and health inequities are antecedents of YPEH and result in adverse mental and physical health outcomes.2 -6
Previous research describes numerous benefits of the human-pet relationship including increased self-esteem, safety, improved mental health and well-being, and increased ability to manage stressful life events.7 -9 In addition to these benefits, YPEH who own a pet may be less likely to experience loneliness, depression, and substance misuse. 10 Emerging research suggests that cohabitating and connecting with their pet as part of the family may be protective for experiences of psychological distress among unhoused LGTBQIA+ youth.11,12
YPEH and Interactions with the Healthcare System
YPEH have disproportionality higher rates of acute and chronic illness, including living with mental illness(es) and substance use disorder, compared to their housed peers, and increased exposure to environmental factors such as heat, cold, noise, pollution, and pests.2,4,6 Compounding this higher burden of illness, YPEH also encounter increased barriers in seeking and accessing healthcare that may include financial, transportation, inconsistent access, fear or discrimination by and/or low trust in healthcare providers, and poor integration of mental health and trauma-informed approaches during the provision of care.6,13,14
Barriers of Pet Ownership Among YPEH
Despite the strengths and benefits of the human-animal bond and high rates of pet ownership (estimated 10-25%) among persons experiencing homeless (PEH), 15 many shelters and temporary and permanent housing services do not allow pets.8,16 This creates a barrier to accepting services because PEH may decline emergency shelters or housing that do not allow pets.16 -18
Access to and the financial cost of long-term veterinary care can be an additional challenge for YPEH with a pet.10,16 As these pets are typically valued as family members and sources of well-being, 11 when their pet gets sick, YPEHs are presented with a financial dilemma: whether to address their own or their animals’ needs. 19
The Seattle One Health Clinic
The World Health Organization and the Centers for Disease Control define One Health as a transdisciplinary approach that emphasizes the inextricable interconnections between humans, animals, and ecosystems.
20
This provides a framework for care delivery that highlights the importance for veterinarians and human healthcare experts to
The Seattle One Health Clinic (OHC) was established in 2018 and is a collaboration between the University of Washington Center for One Health Research (COHR), Washington State University (WSU) College of Veterinary Medicine, and Neighborcare Health, a grant-supported federally qualified health clinic (FQHC) network serving Washington’s homeless community. The veterinary care team is staffed by WSU faculty, staff, and students, human healthcare is provided by the FQHC and clinic operations are supported by COHR and the University of Washington’s University District Street Medicine student volunteers. The supplies are sourced using donations to the program, grants, and partnerships with organizations such as The Street Dog Coalition. The OHC is housed at New Horizon, a youth and young adult advanced emergency shelter serving individuals 18 to 25 years old and serves youth ages 13+ during daytime hours.
The OHC values and supports the human-animal bond and improves the health of the family unit by adding free veterinary care into the existing FQHC clinic. Veterinary and human healthcare are integrated in order to provide enhanced healthcare for pets and pet owners. The Seattle OHC occurs twice a month for 3 h per clinic. Pet owners learn about the Seattle OHC through youth and young adult shelters, case managers, and other homeless service providers, as well as through word of mouth.
In addition to volunteers, a consistent veterinarian and nurse practitioner partner to provide continuity of care on a regular cadence, collaborating to create a single healthcare plan for the human-animal unit. Clients who visit the One Health Clinic consult with both the animal and human healthcare providers. This allows the providers to address shared health needs such as extreme weather events, pest exposures, water and soil contaminants, and psychosocial risks such as domestic violence, and the intersections between the 2 species such as behavioral health and zoonotic disease spread.
We report on the data collected at the Seattle OHC clinics occurring from 2019 to 2022. The purpose of this study is to describe the medical, psychosocial, and environmental health needs among Y/YA experiencing houselessness and their companion animals.
Methods
Positionality: The Seattle OHC clinic staff, care team, and evaluation team have experience and expertise in the following areas: community support and advocacy services, public health, veterinary care, nursing, healthcare and services eligibility specialist, medicine, academics, epidemiology, and lived experiences that informed the conceptualization of this project and manuscript.
Participants and Study Design: We analyzed retrospective clinical intake data collected at 245 healthcare encounters during the 67 One Health Clinics that occurred between October 2019 and October 2022. Additional information on the OHC Seattle has been previously published. 22
Data sources: Included human health data abstracted from the (a) medical records, (b) veterinary records, and (c) intake and care documentation forms created for the OHC clinic (“Navigation Forms”). The OHC Navigation Form is designed to capture animal healthcare needs and shared environmental exposures, while also introducing the expectation that the YPEH will consult/visit with the human healthcare practitioner by asking about their own healthcare needs. In alignment with the One Health Framework, follow-up human healthcare-only visits were counted numerically, and these data were excluded from our analyses. Abstracted health information was assigned an anonymous ID to protect the confidentiality of client health data. Neighborcare Health matched veterinary records to owner subject ID.
Human variables: Abstracted demographic variables included: age at first visit, self-reported gender, race, and ethnicity. Chart abstraction determined care needs identified at human visits by the human healthcare provider, which we categorized through deductive coding into categories of human body system(s). Whether participants sought human healthcare at the time of clinic check-in was extracted from the Navigation Form. To determine if a patient established care, we reviewed linked medical charts to see if a non-emergency visit was documented in the previous 2 years. If not, we considered this person to have established care if they were seen at OHC.
Animal variables: Variables extracted from the vet record included: animal species (cat, dog, other), and veterinary care needs identified/care provided at the visit.
Human-animal dyad variables: We abstracted client responses to questions about their night housing status, benefits and barriers to pet ownership, whether the client’s animal is documented as an emotional support animal (ESA), environmental health concerns for humans, and environmental health concerns for pet.
All study protocols were reviewed and approved by the University of Washington (UW) Institutional Review Board (STUDY00005322). Neighborcare Health maintains “Release of Information” forms signed by patients that allow the veterinary team to communicate with the human health team for care coordination.]
Data Analysis
Anonymized study data were entered into and managed using REDCap, an electronic data capture tools supported by the UW Institute of Translational Health Sciences.23,24 REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies. We used R (version 4.2.2) to conduct descriptive statistics.
Results
Demographics
The majority of human participants were 23 years old or younger, precariously housed, and female-identifying (Table 1). Participants at this OHC represented diverse race and gender identities.
Demographic Characteristics N = 88 human clients, 171 animals.

Health Care Provided
During the study period, there were 245 clinic visits. Our review of the Epic EMR indicated of the 88 human clients who came to the clinic, 75 clients saw a human healthcare provider at least once and 40 (57.1%) established healthcare for the first time in the past 2 years (4 patients were excluded due to not being able to review their medical chart). Of those 40 clients, 34 (85.0%) had one or more follow-up appointments with primary or specialty care within 2 years following their initial OHC appointment.
All animal clients that completed an OHC visit were seen by a veterinarian and received necessary care. Nearly 80% of clinic visits resulted in clients receiving human healthcare, including 69% of visits where clients did not seek human healthcare at clinic check-in (Table 2).
Health Seeking and Provision of Care by Visit N = 164 a Clinic Visits With Completed Navigation Forms.

81 client visits were excluded for no Navigation Form.
The most common documented treatments were reproductive & sexual health (79) and mental health (78). Our analysis indicates that multiple care needs were addressed during 115 human health visits.
The most common documented veterinary treatments were preventative care vaccinations (317) and flea treatment (178).
Benefits and Barriers of Pet Ownership
When assessing the benefits and barriers of pet ownership reported by participants on the Navigation Forms, clients reported barriers to housing (25.0%), healthcare (13.6%), and “other” (17.0%) during at least one of their visits to the OHC. Most clients reported the primary benefits of pet ownership as psychological (59.1%), safety (14.8%), and “other” (11.4%). In the “other” response space one client described “Honestly she keeps me alive. . .I promised her that I’d be here.”
Frequency of Human Healthcare Provided a N = 375 Care Treatments Provided.
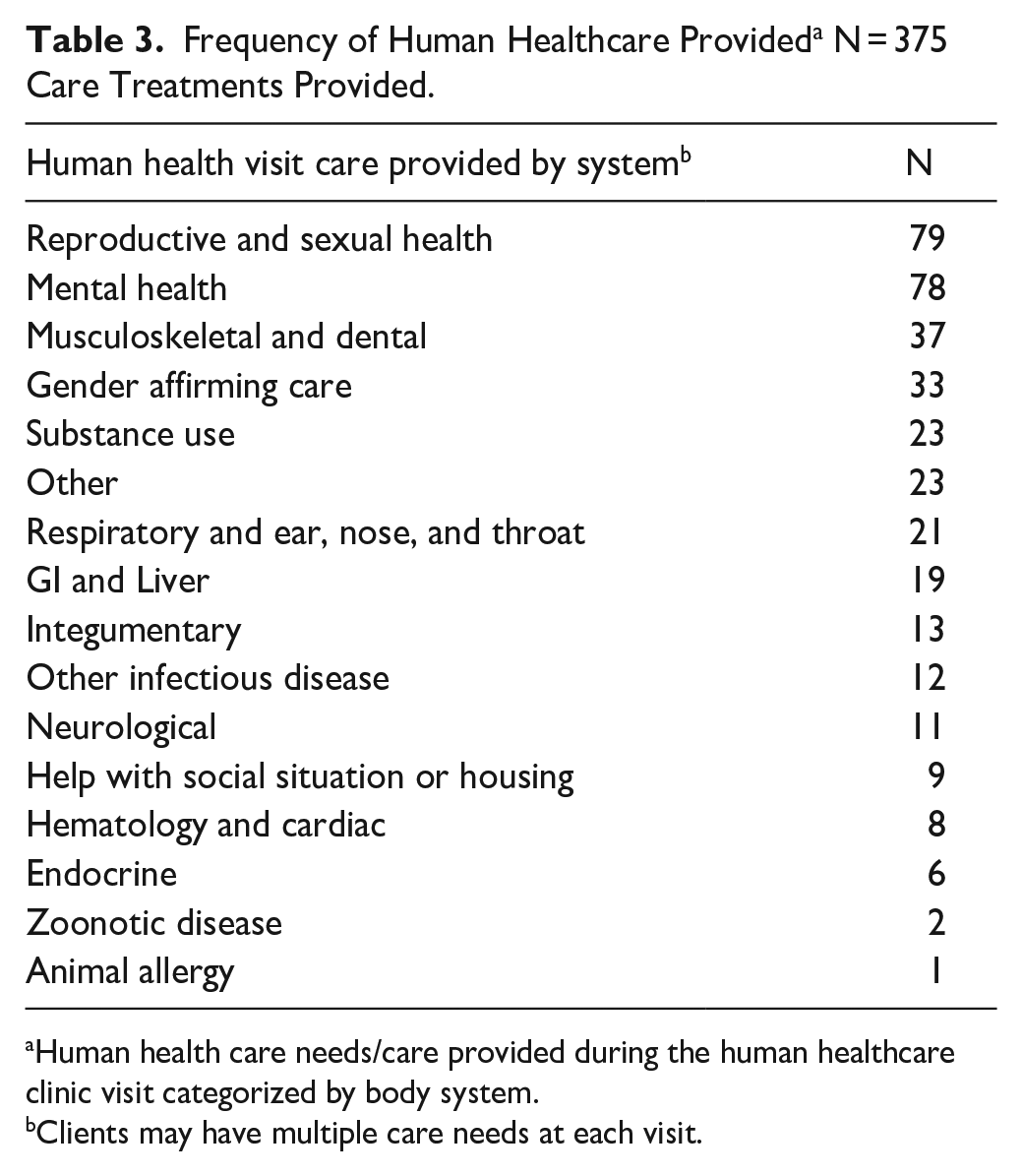
Human health care needs/care provided during the human healthcare clinic visit categorized by body system.
Clients may have multiple care needs at each visit.
Animal Veterinary Visit, N = 652 Care Needs/Treatments.

Animals may have multiple care needs identified at each visit.
Environmental Concerns
Table 5 describes clients’ reports of environmental health concerns for themselves and their animals. Clients reported food insecurity, heat, and cold as the most common environmental concerns for themselves and their animals. At less than half the visits where clients reported concerns related to heat, cold, rain, and food insecurity for themselves or their pets identified it as a shared concern for both humans and animals.
Reported Environmental Health Concerns N = 97 Visits. a

67 clients excluded for not have this portion of the Navigation Form completed.
Multiple concerns may be reported at each visit and for each animal.
Human only question.
Animal only question.
Some “other” concerns included poor ventilation, mold, mice, raccoons, and fleas.
Discussion
Our study findings indicate that an integrated model of human health and veterinary care delivery for people experiencing homelessness with animals may increase access to important preventative care and treatments for both human clients and animals. These results further suggest that incorporating the human-animal bond in healthcare delivery may optimize health-seeking behaviors and identify important environmental stressors among YPEH.
We found that most clients who visited the Seattle OHC accepted human healthcare, including those who initially sought animal care only on intake. Our results may indicate the integration of veterinary care and primary human healthcare can connect the motivation to care for one’s pet to caring for oneself, ultimately increasing engagement in healthcare.
Another important finding was that half of all clients that visited the Seattle OHC had one or more follow-up visits including those who initially sought animal care only on intake. This was greater than the rate reported in a previous study of a shelter-based YPEH human-only clinic that found a 13% rate of second follow-up. 6 Our study population was systematically different in that they were all pet owners, indicating that pet ownership may provide psychological and social connectedness which has been positively associated with health among YPEH. 25
Our results suggest that multiple preventative and acute health needs are shared across the human-animal dyad, including zoonotic disease, environmental heat and cold, and mental/behavioral health. These findings indicate that a transdisciplinary model of health care, utilizing the One Health approach, is likely to improve health outcomes for YPEH and their pet. While environmental health concerns for humans or animals were often reported, overlapping concerns were less common. This suggests that assessing the human-animal unit as a dyad rather than separate individuals can increase the identification of environmental exposures and allocation of necessary resources such as heating and cooling centers for people experiencing homelessness and their animals. This also highlights an educational opportunity to ensure pet owners are aware of the environmental risks that can have adverse health outcomes for themselves and their pets.
When examining barriers and benefits related to pet ownership, our findings were consistent with prior literature. Commonly reported obstacles included accessing housing and services that do not allow pets.5,16 -18 Notable benefits included a sense of purpose, responsibility, connectedness, and psychological health. 18 This supports the growing evidence that pet ownership among YPEH may increase well-being.10,11
Our study had some limitations. We had a moderate amount of missing data for measures collected on the Navigation Form, which was likely the result of a combination of factors including a gap in clinic volunteer training for completing the Navigation Forms and inefficacy of the Navigation Forms themselves. In addition, navigators completing the Navigation Forms with the client may result in reporting bias, social desirability bias, or observation bias. To mitigate these limitations in future Seattle OHC work, the navigator training and the navigator form (see updated Navigation form in Appendix A) have been redesigned through a quality improvement process. The small sample size, single regional study site in an urban setting, and narrow age range of the study population limited the generalizability of our findings to the larger population.
One Health Clinics decrease barriers to accessing both veterinary and human healthcare by providing a single, integrated healthcare plan that benefits the animals, guardians, and public health. Our results suggest that the human-animal bond may be an important strength among youth experiencing homelessness; a One Health approach to healthcare may increase rates of health-seeking behaviors, preventative care, treatment, and accessing follow-up care. This model of care can be modified for patient populations with historically low access to health care such as unhoused adults, the elderly, rural settings, and farming communities.
Footnotes
Acknowledgements
The authors would like to acknowledge that the work presented in this manuscript was made possible through the participation of the human and animal clients who visited the Seattle OHC and the collaboration with New Horizons, Neighborcare Health, WSU, UW, the University District Street Medicine volunteers, and clinic staff.
Authors’ Note
The authors acknowledge that some PEH identify the animals they live with as service animals or emotional support animals and not as pets or companion animals. For brevity, the authors chose to use the terms pets and animals interchangeably and should be understood to be inclusive of all forms of companionship and service noted above. Additionally, some individuals would not use the term “ownership” to describe the relationship between themselves and their animal. For the context of this paper, the authors used ownership when discussing barriers caused by having pets and companionship when discussing the benefits of the human-animal bond.
Ethical Considerations
All study protocols were reviewed and approved by the University of Washington’s Institutional Review Board (STUDY00005322). Neighborcare Health maintains “Release of Information” forms signed by patients that allow the veterinary team to communicate with the human health team for care coordination.
Consent to Participate
This evaluation includes deidentified clinical charts extracted from an electronic medical record (EMR) system. Informed consent was not collected for this evaluation.
Consent for Publication
Not applicable
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the National Institutes of Health, National Institute of Nursing Research Training Program in Global Health Nursing at the University of Washington (T32 NR019761). This work was also supported, in part, by funding from the New Tudor Foundation, as well as from a gift from the now shuttered Y/YA Shelter “Peace for the Streets by Kids from the Streets,” who supported Y/YA and the human-animal bond from 1995-2017, and whose work through the clinic carries on.
Funding for the publication of this study was provided by the American Society for the Prevention of Cruelty to Animals® (ASPCA®) Open-Access Publishing Fund.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitivity of the data, data will be available on request. Please contact the corresponding author.