
Abstract
Objective:
To identify predictors of clinically meaningful declines in health-related quality of life (HRQoL) among COVID-19 patients over a 12-month period in a prospective, natural history investigation.
Methods:
We conducted a longitudinal study involving individuals who had tested positive for SARS-CoV-2, assessing various factors and their impact on HRQoL after 12 months. Key potential predictors examined included demographic information, medical history, and symptom reporting. HRQoL was measured using the validated EuroQoL Dimension 5 level scale at baseline and at the 12-month follow-up.
Results:
The analysis revealed that shortness of breath, a diagnosis of COPD, lower BMI, and a history of anxiety at the initial visit were all significantly associated with clinically meaningful worsening of HRQoL at 12 months. Specifically, individuals with these factors experienced more pronounced declines in HRQoL compared to those without. Notably, the small number of COPD cases within our sample (4 total) limited the reliability of this predictor.
Conclusions:
Shortness of breath, lower BMI, and a history of anxiety are important predictors of deteriorated HRQoL in COVID-19 patients over the long term. Although the association with COPD is less reliable due to sample size limitations, these findings highlight the need for targeted interventions and continued support for patients exhibiting these risk factors to improve long-term HRQoL outcomes. Future research with larger samples is needed to confirm these results and further investigate the role of these factors in post-COVID HRQoL declines.
Background
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by novel coronavirus (SARS-CoV-2). 1 Even when individuals recover from the acute SARS-CoV-2 infection, there are often lasting symptoms that severely affect an individual’s function and quality of life.2 -4 It has been well-established that COVID-19 is associated with a wide variety of symptoms, possibly affecting any organ system, and that these symptoms may be persistent in many regardless of age, gender, race, or ethnicity.5,6 Current estimates suggest that approximately 60% of the entire US population has been infected with SARS-CoV-2 7 and the CDC reported 277 deaths during the last week of June, 2024. 8 Hence, primary care physicians have been and will continue to see patients at various points after initial SARS-CoV-2 infection and it is imperative to identify individuals who will have the greatest impact of COVID-19 on their lives and health.
Health-related quality of life (HRQoL) is a widely used indicator of one’s health and well-being. HRQoL encompasses physical and mental health perceptions, with the CDC defining HRQoL as “an individual’s or group’s perceived physical and mental health over time.” 9 HRQoL is an important component of public health surveillance and can be considered a marker of unmet needs. 10 In addition, self-assessed health status has been shown to be a better predictor of mortality and morbidity than more traditional risk factors such as functional status and depression.11,12
Therefore, if risk factors can be identified that distinguish individuals that have diminished HRQoL post-COVID-19, healthcare and public health providers can better prospectively identify this population to address potential unmet needs. While there have been numerous studies examining the HRQoL of individuals after SARS-CoV-2 infection, with a recent systematic review including over 20 studies, 13 the majority of studies investigated HRQoL cross-sectionally and did not assess long COVID. The few studies that have examined HRQoL prospectively stopped evaluation at 3 months 14 or 6 months. 15 The literature on COVID-19 does continue to grow every day, specifically in the context of examining long COVID.16 -22 However, the vast majority of literature on long COVID is also cross-sectional, with HRQoL only being assessed at 1 time point and utilizing a comparison of HRQoL in individuals who had COVID-19 to individuals without COVID-19. While these analyses provide important information about the prevalence and burden of symptoms at different snapshots in time, it doesn’t provide continuous monitoring of data that would possibly identify individuals at particular risk for HRQoL that worsens over time.
Therefore, the aim of this prospective, natural history study was to identify predictors of changes in HRQoL over time among individuals with a history of SARS-CoV-2 infection. Participants entered the study at varying timepoints after infection (ranging from 44 to 420 days) and were followed for at least 12 months.
Methods
Patient Population
Based on the search of our electronic medical record system, individuals who had tested positive for SARS-CoV-2 (diagnosed with a positive qPCR test or an antigen test) at an outpatient or inpatient facility of Inova Health System between March 2020 and July 2022 were contacted to participate in this prospective study. Eligible enrollees were required to have been at least 28 days post COVID-19 diagnosis, willing and able to provide an informed consent, and be at least 18 years of age. The study protocol received approval from both the Institutional Review Board (IRB) of Inova Health System and from the Western IRB prior to study initiation. Written consent was obtained for in-person patients and verbal consent was obtained for virtual patients.
Data Collection
The full description of all study procedures and assessments (physical, cognitive, and questionnaire) conducted for the protocol is detailed in our previous publication. 23 All participants were asked to verbally answer specifically curated questions about their COVID-19 illness experience (eg, duration and severity of illness). For this investigation, demographic information, medical history, and HRQOL data were utilized. These data were from the baseline (initial) and 12-month time points. Consented participants were given the option to participate in-person at our clinic or remotely (by phone or through online video conferencing) for both time points.
Post-COVID Symptoms
To assess post-COVID symptoms at the Baseline visit, participants were verbally asked if they had any current symptoms that were not present prior to their COVID-19 infection. Due to the variability in responses, symptoms were reviewed by investigators and categories were created based on the most commonly reported symptoms.
HRQOL/PRO
To evaluate the impact of COVID-19 on function and HRQOL, we included data from the EuroQol 5 Dimension 5 Level (EQ-5D) assessment. The EQ-5D is a generic instrument that is widely used for the calculation of health utility scores. Health status is measured in terms of 5 dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression; the resulting 5-digit number is then converted into a single weighted index score (range 0-1) using a previously described crosswalk algorithm. 24
To assess Mobility, the participant is asked if they have “no,” “slight,” “moderate,” or “severe” problems walking or are “unable to” walk. For Self-Care, they are asked if they have “no,” “slight,” “moderate,” or “severe” problems with washing or dressing themselves or are “unable to.” For Usual Activities (ie, work, study, housework, family, or leisure activities), they are asked if they have “no,” “slight,” “moderate,” or “severe” problems with usual activities or are “unable to.” For Pain/Discomfort, they are asked if they have “no,” “slight,” “moderate,” “severe,” or “extreme” pain or discomfort. For Anxiety/Depression, they are asked if they are “not,” “slightly,” “moderately,” “severely,” or “extremely” anxious or depressed.
To detect meaningful clinical change in EQ-5D scores over time, we adopted the concept of minimal clinically important difference (MCID), which is defined as the smallest difference score possible to be perceived by patients as beneficial in order to mandate change in patient management. 25 The purpose of MCID is to add clinical relevance from the patient’s perspective when observing changes to HRQOL scores. This approach has been previously utilized by others when investigating EQ-5D.25 -27
Statistical Analyses
Parameters were summarized as mean ± standard deviation or frequency (percentage), and were compared between groups (those with clinically important worsening of EQ-5D compared to those without) using Wilcoxon rank sum non-parametric test (continuous parameters) or Pearson’s chi-square test (categorical parameters). Independent predictors of the study outcome (the presence vs absence of minimal clinically important worsening of EQ-5D at 12 months following baseline) were assessed using a logistic regression model. MCID groups were defined as a change of EQ-5D index of 0.05 (5% of range size) in either direction. Two-sided P-values of <.05 were considered statistically significant.
Results
There were 82 participants (out of 189 participants that were contacted for follow-up) who had HRQoL assessed at the baseline timepoint and 12 months after baseline (Table 1). The majority were females (58.5%), white (54.9%), college-educated (67.1%), married (57.3%) with a mean age of 55.7 ± 14.8, and average body-mass index of 30.5 ± 8.1. The most common co-morbidity was hyperlipidemia (42.7%) followed by hypertension (37.8%).
Characteristics of Participants With and Without Minimal Clinically Important Worsening of HRQoL at 12 Months Post Baseline.

Abbrviations: BMI, body-mass index; COPD, chronic obstructive pulmonary disease.
Statistically significant (P < .05) difference between those with and without worsening of HrQoL.
Trend (P < .10) for a difference between those with and without worsening of HrQoL.
On average, participants entered the study 172.4 (89.5) days after their diagnosis. A total of 33 people were hospitalized (40.7%) and 8.6% had been placed on a ventilator. At baseline, 92.7% of the sample reported at least 1 symptom and on average experienced 2.82 (2.28) symptoms. At 12 months, 76.3% of the sample reported at least 1 symptom and on average experienced 2.11 (2.22) symptoms.
Health-Related Quality of Life
As presented in Table 2, individuals with a minimal clinically important worsening of HRQoL have statistically significant differences in all 5 domains that are assessed: mobility, self-care, usual activity, pain/discomfort, and anxiety/depression. Participants with HRQoL worsening were more likely to report shortness of breath at baseline, have a diagnosis of chronic obstructive pulmonary disease (COPD), have a lower BMI, and a history of anxiety (Tables 1 and 2).
Health-related Quality of Life (HRQoL) Experienced by Participants With and Without Minimal Clinically Important Worsening of HRQoL at 12 Months Post Baseline.
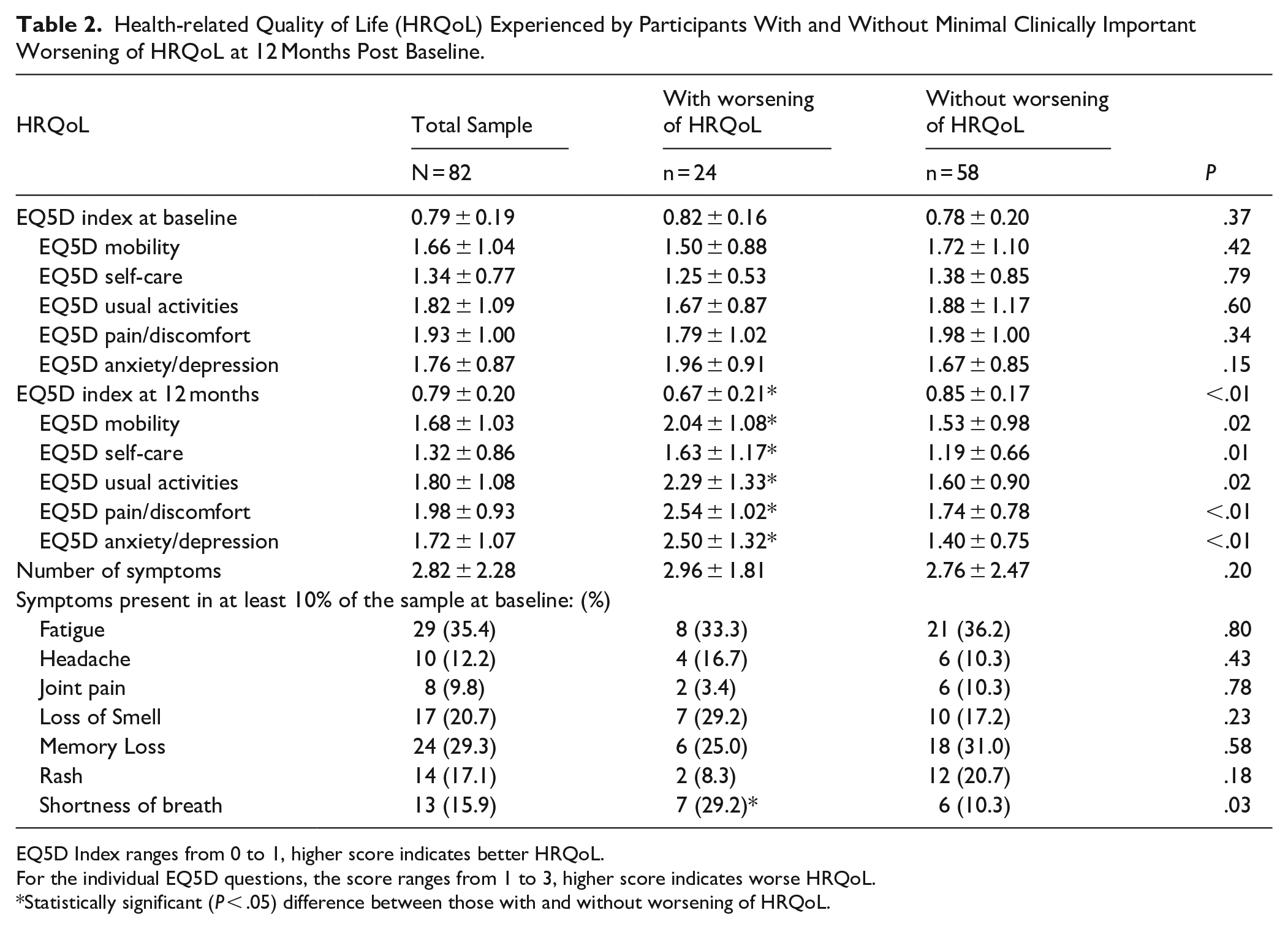
EQ5D Index ranges from 0 to 1, higher score indicates better HRQoL.
For the individual EQ5D questions, the score ranges from 1 to 3, higher score indicates worse HRQoL.
Statistically significant (P < .05) difference between those with and without worsening of HRQoL.
Prediction of Worsening Health-Related Quality of Life
Table 3 shows the factors associated with a clinically important worsening of health status based on a multivariable logistic regression. Factors that were statistically significant univariately were entered into the model. All factors of the model were assessed at baseline. Shortness of breath symptom report, history of anxiety, and BMI remained as statistically significant predictors in the model.
Statistically Significant Factors Predicting Minimal Clinically Important Worsening of Health-related Quality of Life at 12 Months Following Baseline.

Abbreviations: BMI, body-mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease.
COPD was only present in 4 individuals (4.9% of the sample) and while the odds ratio was very high, it did not reach statistical significance.
Discussion
Summary
Our study found that shortness of breath, diagnosis of COPD, lower BMI, and a history of anxiety at the initial visit were all associated with worsened HRQoL 12 months later (Table 3). The number of cases of COPD within the sample (4 total) limits the reliability for that predictor.
Findings Within the Context of Previous Research
The most surprising finding was that those with higher BMI at the initial visit were not more likely to have minimal clinically important worsening of HRQoL. The majority of the literature associates increased BMI with increased rate of hospitalization, ICU utilization, increased post-COVID syndrome risk, and longer recovery—especially for women or when there was pulmonary disease prior to COVID infection.28-32 The presence of post-COVID sequelae is not confined to those who have had severe SARS-CoV2 infection (eg, hospitalization). 23 Our data are consistent with portions of that previous literature; the group that had higher BMI (no worsening of HRQoL) did have higher numbers of cases of hospitalization and ventilator use, albeit not to a statistically significant degree. Higher BMI has also not been universally reported as worsening mortality in those with acute COVID, even in the early days of the pandemic.33,34 Others have noted that there may be a U-shaped curve between BMI and outcomes, with both low and high BMI patients at increased risk. 35
However, this is not the first time that higher BMI has been associated with better recovery post illness, also known as the obesity paradox. 36 This is especially seen in older adults, for whom low BMI is associated with worse all-cause mortality outcomes in the presence of comorbidities and acute conditions when short and long-term mortality are assessed. 37 Future investigations will need to study this phenomenon further, with longitudinal studies being required to thoroughly understand the prospective relationships between BMI and diminished HRQoL.
Shortness of breath is a common symptom in both acute and post-COVID syndrome 38 and in our investigation, it was a predictor of worsening HRQoL. Shortness of breath can manifest in various ways, and its relationship to HRQoL and COVID-19 can be complex. There are various potential explanatory factors including: (1) lung damage; (2) inflammation; (3) deconditioning; (4) cardiovascular effects; (5) reactivation of previous symptoms; and (6) psychological factors.
COVID-19 primarily affects the respiratory system, and severe cases can lead to lung damage or scarring. Even after recovery, individuals may experience ongoing respiratory issues, including shortness of breath. Persistent inflammation following a COVID-19 infection can contribute to ongoing respiratory symptoms. The inflammation might affect the lungs or the lining of the airways, leading to breathing difficulties. Prolonged illness or hospitalization can result in physical deconditioning. Individuals who have been bedridden or less active during their illness may experience decreased lung capacity and endurance, leading to shortness of breath during physical activity. COVID-19 can also impact the cardiovascular system. Inflammation and damage to the heart or blood vessels can contribute to symptoms like shortness of breath, as the heart works harder to supply oxygen to the body. In some cases, individuals may experience a reactivation of symptoms related to pre-existing conditions, such as asthma or COPD, which can be worsened by COVID-19. 39 Anxiety and stress related to the illness or the recovery process can exacerbate the perception of shortness of breath. Some individuals may feel more breathless due to heightened awareness or anxiety, even if there is no significant underlying physiological cause.
Our findings support that both a history of COPD and anxiety are related to worsening HRQoL, along with shortness of breath. To further investigate potential factors that were related to shortness of breath, we conducted an additional analysis comparing those individuals that reported shortness of breath at the initial visit to those that did not report that symptom. There was not strong evidence that the shortness of breath was related to an underlying mechanical disruption, as the arterial oxygen saturation was similar across groups, as was the history of COPD and being hospitalized and/or being on a ventilator during COVID. However, there were various factors that distinguished individuals with shortness of breath at the initial visit including a history of asthma, higher BMI, higher resting heart rate (but not systolic or diastolic blood pressure), a higher number of symptoms reported, and higher scores on assessments of anxiety (ie, GAD-7). It is clear that the relationship between shortness of breath and worsening HRQoL is multifaceted, likely involving both physical and psychological aspects. It will be important to continue to study this symptom in order to try to understand the prospective relationship with HRQoL and the underlying factors that cause the manifestation of the symptom, perhaps including repeated measures of pulmonary mechanics, which we did not measure in this study.
Limitations
There are limitations that should be noted for this study. One limitation is there was no time limit criteria for when subjects needed to enroll after they met inclusion criteria of >28 days post-acute infection. Thus, the window between infection and study enrollment was relatively wide, as some subjects were enrolled shortly after infection and others were enrolled months later. It is likely that because of this, there were post-COVID symptoms that were not captured at the baseline visit due to these symptoms having subsided during the period between infection and enrollment. The second limitation is missing data. Not all subjects at the baseline and/or 12 months visit completed the EQ5D assessment and therefore could not be included in this analysis. Although the study originally recruited several hundred people, with a smaller portion included in this investigation (due to missing data), the sample size may not have been powerful enough. For example, COPD diagnosis was statistically significant, but with only 4 cases within the cohort, the confidence interval of the finding was too wide to be useful in determining the size of the effect. Additionally, the sample consisted of individuals that volunteered for a longitudinal research study, and individuals that volunteer for these types of studies may have inherently different experiences than individuals that would not volunteer.
Another important limitation to consider is the conceptual validity of HRQoL measures, particularly when using multi-domain tools such as the EQ-5D. Some scholars have raised foundational concerns about the extent to which the anxiety/depression domain may influence or confound responses across the other domains (mobility, self-care, usual activities, and pain/discomfort), particularly in contexts marked by widespread psychological stress such as the COVID-19 pandemic. 40 In our study, it is possible that elevated anxiety and depression during the pandemic influenced participant responses across all dimensions, thus complicating the interpretation of HRQoL as a distinct and multidimensional construct. While HRQoL remains a widely used and accepted metric, this potential overlap—especially under conditions of heightened psychological distress—should be considered when interpreting our findings.
Conclusions
Our study highlights key predictors of minimal clinically meaningful declines in HRQoL in COVID-19 patients over a 12-month period. Notably, shortness of breath, a diagnosis of COPD, lower BMI, and a history of anxiety at the initial visit were all significantly associated with clinically important worsening of HRQoL. These findings underscore the importance of evaluating patients for these symptoms and addressing them early in the recovery process to potentially mitigate long-term declines in quality of life. The limited number of cases with COPD (n = 4) affects the reliability and generalizability of this predictor. Overall, our results emphasize the need for ongoing monitoring and support for COVID-19 patients, especially those presenting with shortness of breath, lower BMI, and a history of anxiety, in order to improve long-term outcomes and enhance quality of life.
Footnotes
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board (IRB) of Inova Health System and from the Western IRB. Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Leyla de Avila, Maria Stepanova, Jillian K. Price, and Carey Escheik. Resources for the study were provided by Zobair M. Younossi and Lynn H. Gerber supervised the investigation. The first draft of the manuscript was written by Ali A. Weinstein and Leyla de Avila and all authors commented on previous versions of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internal support from Inova URAP grant #U20-09-4275.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.