
Abstract
Background:
Burnout among Community Health Center (CHC) providers has worsened post-COVID-19, exacerbated by understaffing and heightened recruitment challenges due to competition from higher-paying hospitals and private practices.
Objective:
This exploratory qualitative study investigates strategies used by four leading CHCs to address perceived drivers of burnout among their providers.
Methods:
The study used qualitative interviews with CHC staff to explore approaches to mitigating burnout. Focus was placed on organizational strategies, staff engagement, and operational changes aimed at enhancing provider wellbeing.
Results:
Key challenges included low funding and rapid growth, leading to staffing shortages and strained relationships between staff and leadership. Common strategies to combat burnout involved: (1) emphasizing the CHC mission of supporting staff wellbeing, (2) creating onboarding and workforce development programs focused on support, (3) implementing operational changes to reduce workloads and maximize patient care time, (4) fostering staff involvement in decision-making, and (5) using wellness surveys with the expectation of visible changes based on feedback.
Conclusion:
The study found that employee voice is crucial in addressing burnout, contrasting with wellness approaches that focus solely on individual staff members. Involving staff in decision-making and addressing systemic issues are viewed by participants as essential strategies for mitigating burnout in CHCs.
Background
The safety net for primary care services in the United States is constituted by nearly 1,400 community health centers (CHCs) that provide care to almost 32 million patients. 1 Ninety-one percent (91%) of their patients are low-income, 9.7 million are rural, 1.4 million live without housing, 1 million are farm workers, and almost half a million areveterans. 1 This critical function is threatened by insufficient funding. A recent study showed that, in 2022, 11 million patients were served by health centers with negative margins that threaten CHC viability and access to care. 2 Another study showed that inflation-adjusted, per-patient federal funding declined between 2015 and 2023 by 30%. 3 We also know that staff shortages at CHCs have been growing. A 2024 survey found that 77% reported a shortage in mental health providers, 70% reported shortages in primary care physicians and nurses, and 69% reported a shortage in enabling service providers. 4
This issue remains a persistent challenge for CHC leaders. Surveys show staff retention is ranked as their top concern, 5 likely due to difficulty in paying staff competitive wages resulting from these funding constraints. Research highlights that understaffing is a major contributor to burnout.6,7 While limited studies examine burnout among CHC workers, one study of over 120 organizations—including community-based and Federally Qualified Health Centers—used the Mini Z measure of physician burnout and found that clinician burnout reached 60% in 2021, a sharp rise from 45% in 2019. 8 A 2022 Health Resources Services Administration (HRSA), using the Oldenburg Burnout Inventory and extending it to six points (rather than the original four), found burnout in CHCs was 3.1 out of 6 among respondents. 9
It may be that the CHCs’ safety net mission provides some protective influence since employees may be choosing to work in a CHC over a non-safety net setting despite lower wages. It may also be that CHCs unique governance structure, with the requirement that 51% of board members be health center patients, strengthens the staff’s trust in this institutional mission. Perhaps some CHCs are implementing strategies that are helping, and other settings may be able to learn from their experiences. While these are not the central questions we address in this study, they do motivate our research aim.
This study examines how four CHCs, recognized by their peers as leaders in addressing burnout and moral injury, are working to tackle these challenges.
Existing Evidence
Burnout is a manifestation of chronic workplace stress resulting in the experience of emotional exhaustion, depersonalization, and a sense of ineffectiveness. 10 An overlapping but distinct phenomenon is moral injury, which refers to the “psychological, biological, spiritual, behavioral, and social impact of perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations.” 11 While moral injury in the past has been viewed as one driver of burnout, numerous scholars now suggest that it is related but distinct. Conceptually, moral injury in healthcare is often a result of health workers feeling they are not able to do what they believe is right for their patients, including delivering high-quality care and/or helping them access the needed resources.12 -14
There is still very little outcomes research on moral injury, but one study showed that burnout and moral injury contribute to each other and that they also both directly affect the intent to leave. 15 Outcome studies on burnout reveal that it is not only associated with poor health outcomes for health workers but contributes to high turnover rates and threatens access to and quality of care.10 -12
Existing studies of burnout specific to CHCs point to workload, lack of support from leadership, poor communication, and moral distress as drivers.9,16 -20 Evidence on how best to address burnout in CHC settings, however, is extremely limited. Our review of the literature on interventions to increase wellbeing among staff at CHCs found five studies that met the inclusion criteria (see Appendix A). Two studies found no effect of the interventions. The first was a qualitative, descriptive study of a 1-year Provider Wellness Initiative that included individual and peer-focused, systems-focused, and team/community-focused programming. 17 Clinicians reported no improvements, particularly in their priority area, which was greater control of their clinical practice. The second study, a repeated cross-sectional design, assessed whether an intervention designed to support health centers’ transition from volume- to value-based models of care improved staff satisfaction. They found it did not change. 19
Three studies found small positive effects on burnout or staff satisfaction, but the interventions were disparate and mainly focused on quality of care improvements. Using a cross-sectional descriptive design, the one examined the effects of a quality improvement initiative called the Health Disparities Collaboratives (HDC) on burnout. They found a positive effect, but only when the HDC workload was shared fairly, new staff were trained effectively, and sufficient staff and skills development opportunities accompanied the program. 18 The second study was a pre-post intervention design without a control group. They found that a hypertension teaching protocol positively affected staff satisfaction. 21 The last was a cross-sectional study that assessed the effects of an intervention described as “interior enhancements” on staff wellbeing, which included evidence-based design, sustainable initiatives, and an introduction to Lean concepts. 20 They found that the site with the most comprehensive design features had the highest measured Quality of Well-being score, while those with less comprehensive interventions had only minor improvements.
As these studies reveal, there are still large gaps in our understanding of the most effective approaches for reducing burnout and moral injury in CHCs. The literature is sparse, and the interventions tested were highly disparate, making it difficult to compare them. Three different quality improvement initiatives showed some promise, but it was unclear what the mechanisms were for their moderate success. Together, these studies suggest that research on how to address burnout in CHCs is still in its infancy.
This study identifies aims to begin to address this gap by identifying common themes across the approaches used in four CHCs. In Part 1, we examine the primary drivers of the problem that leaders and staff at these CHCs identify as causing burnout and moral injury. In Part 2, we examine the responses designed by leaders to these problems, as well as the similarities and differences across the strategies being used.
Methods
This study was approved by IRB # NCR245546 as exempt. Participants were provided with a consent form prior to the interview via email. We utilized an exploratory, descriptive design to examine strategies employed by four CHCs to address burnout and moral injury among their staff. We identified these four organizations in the context of a national conference of CHCs in early 2024 organized by the National Association of Community Health Centers (NACHC) that was focused on how to be “an employer of choice.” We queried participants on which CHCs had the most experience addressing staff burnout and/or moral injury. Participants identified 12 CHCs that were heavily engaged in this work. We selected four of these CHCs using a purposeful approach that sought diversity across several variables as follows: (a) geographic location (east/west/mid-west/south), (b) size (over 100,000 patients were identified large, and under 30,000 patients were identified small), as well as (c) typical patient populations for CHC, that is, not outliers. The characteristics of the four selected CHCs are presented in Table 1. To ensure confidentiality, we identified the CHCs only as A, B, C, and D.
Characteristics for Community Health Centers in Sample (2023).
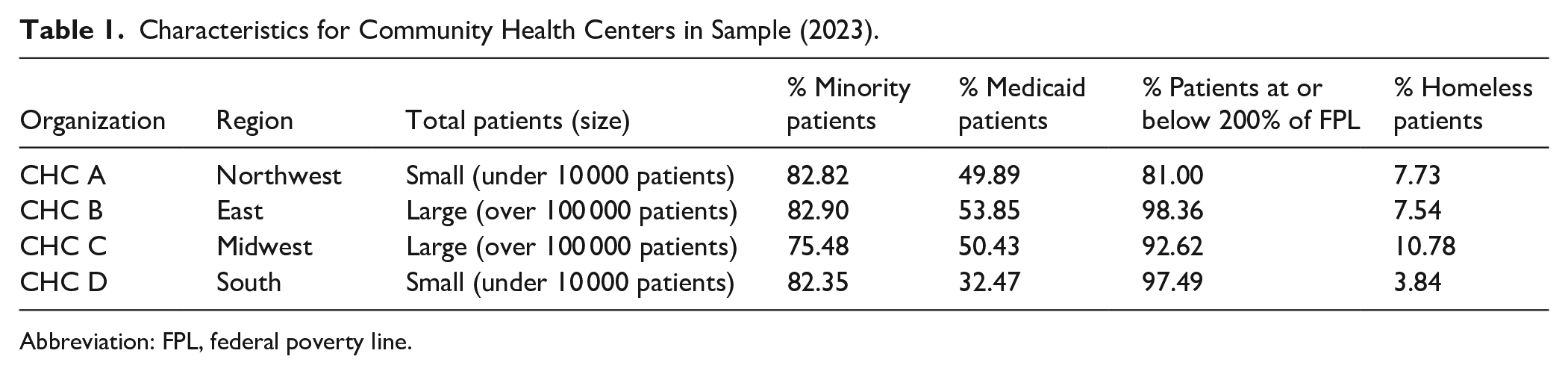
Abbreviation: FPL, federal poverty line.
This sample is not intended to represent the full CHC universe. Indeed, each center’s attributes are specific to their size or demographic served, making them somewhat unique. Because the study aims to identify leading practices rather than representative practices, we do not view the inclusion of CHCs that may not be “average” in size or patient demographics as necessarily a study limitation.
We conducted 15 semi-structured interviews of leaders and employees, with between four and five informants from each CHC. The sample also included executives, as well as frontline health workers from each organization. Interviews were conducted via Zoom from April 2024 to July 2024 and transcribed. Consistent with the principles of theoretical saturation, at 15 interviews, we concluded no new themes or insights were emerging from the data, suggesting that the sample was sufficient. The interview schedule included questions about (1) the extent of the burnout problem, (2) what they viewed as the major drivers, (3) the development of their intervention(s), (4) its perceived effectiveness on wellbeing and staff retention, and (5) any continuing challenges they have encountered. See Appendix B for the interview guide. Analysis of the transcripts was conducted by the two authors and consisted of an iterative process of content analysis. We conducted a structured content analysis where the data were initially categorized into two broad themes: drivers and mitigation. Using a two-step coding process, we first applied these overarching themes and then inductively developed more detailed subcategories based on the data. Meaningful sentences served as the primary coding units, ensuring that excerpts were contextually relevant to the assigned themes. Our coding framework was anchored in the predefined categories of drivers and mitigation, with iterative refinement based on emerging patterns within the data. No analytic software was used for coding and analysis, as the dataset consisted of 15 interviews, making manual analysis a more practical and effective approach.
Results
Part 1: Drivers
The explanatory models of why burnout and moral injury exist in CHCs, as provided by both the leadership and frontline staff at CHCs, focused on CHC-specific issues that relate to three levels: societal, health system, and the CHC organization. These drivers were important to identify in order to understand why the leadership prioritized the strategies that they later described.
Societal Drivers
Several informants discussed the moral injury incurred as a result of bearing witness to the poverty, racism, and other forms of social discrimination experienced by their patients in their daily lives. Leaders noted that the lack of adequate access to health care was at the heart of the creation of the CHC movement in the 1960s. 22 They argued that while this strong commitment to caring for underserved and minoritized communities is a source of pride and identity, it is also a source of moral distress.
One clinician affirmed that the underfunding of CHCs is a legacy of racism and society’s continued devaluation of the population groups they serve. “When people think of poor people in this country, they generally think of Black people. . .of Black women, welfare queens, and images of people who are portrayed as not deserving of much. So, I think what we’re trying to do (at CHCs) is not widely valued in this country. . . I didn’t use to understand why we’re underfunded, which I (now) think is primarily about American racism.”
There was also awareness that many of the support staff also experience the trauma of marginalization, as expressed by a CHC leader. “In this community, our staff have those exact same challenges. They’re dealing with the exact same traumas that the patients are dealing with.”
Many study participants pointed out that underfunding CHCs means that they cannot compete with other healthcare and other industries’ salaries, leading to chronic understaffing. “Healthcare recruitment and retention is an issue in every corner, and while in rural areas it’s the availability of clinicians, in areas closer to (cities), the competitive packages from well-funded hospital systems, are very, very challenging to compete with.”
Again, this was directly associated with being underfunded. “When you’re underfunded that translates to how many visits you’re going to see - because we’re paid by the visit. . . There’s this drive to keep our doors open: how many visits (does) one has to have - without enough support. . .to be helpful to people in all the ways we want to be?”
Faced with this, staff grappled with whether their role in combatting these systemic issues was effective. One clinician talked about how feeling that you have impacted patients’ lives is critical to mitigating moral injury. “I think we’re all prepared to do some suffering for a purpose, if we think that suffering is meaningful and helpful, and accomplishing something. But most of us are not prepared to voluntarily do that without purpose.”
Thus, informants focused on a set of drivers related to the tension between CHCs’ safety net mission and larger societal trends that they perceived to chronically undervalue the importance of their work in helping serve the most disadvantaged populations in the United States. A key variable identified by one participant was the idea that being able to effectively help people, despite these conditions, was protective against burnout and moral injury while feeling that they are not able to provide the care people need and deserve as a driver.
U.S. Health System Drivers
A second set of drivers was related to the increased administrative burden imposed by the health system’s demands for pre-authorization, billing complexity, quality reporting, and clunky electronic health records. These pressures are certainly not unique to CHCs, but informants felt they were particularly offensive in the context of trying to deliver safety net services. As one clinician reported: “As these burdens of documentation have gotten bigger and bigger, more and more has been asked of support staff. We’re drowning and the effect of the drowning is that we can’t do the thing that you want us to do, because we’re spending all our time trying to document that we did the thing.”
CHC leaders were empathetic. One executive noted: “The task is not a doable task. And so, people give up. Constantly. The definition of moral injury is knowing the right thing and not being able to do it. I think you’re at the crux of the beginning of moral distress and moral injury.”
Nurses and medical assistants also report that documentation demands are impeding care. “This is not numbers to us. And that is something that I’m very passionate about. . . I understand we’re looking for good outcomes, but at the end of the day, I’m a nurse first -I want to impact the patients’ lives. I want to hear their stories. I want to be a part of their journey. I want to be a part of their life.”
Organizational Level Drivers
The third set of drivers that emerged from the interviews were specific to organizations. Leaders were cognizant that not all drivers are external and that they bear responsibility for workplace wellbeing. Organizational challenges were particularly salient in CHCs that had experienced rapid growth. Some frontline staff went as far as to link rapid growth to perceptions of (a) an increased emphasis on money, (b) the loss of personal relationships with leadership, and (c) a reduced role for them in decision-making.
One leader from a large CHC acknowledged this: “We were growing from a very personal place to an organization that was too large for people to have a personal connection with all the leaders.” A staff person in the same CHC agreed: “I feel like the organization is just too big. Like they keep expanding and expanding and expanding. We can’t even staff the sites that we have open. We’re struggling in certain places all across the network, across all, you know, different disciplines, different positions.” Staff from another CHC also lamented the growth. She worried about an increased focus on “dollars and cents and audits and productivity, rather than patient care.” This understaffing was one cause of the burnout, according to participants. Some staff worried that the rapid growth had led to reduce participation in decision-making: “We (frontline staff) need to be invested in it too. We need to have some part in it.” They acknowledge that the pandemic was partly to blame: “(In the past) all the managers. . . would discuss (applicants’) applications. Then COVID hit and that was all taken away.” Staff participants expressed the view that they wanted to be more involved in decisions. “Management should take their stronger people and be able to go, hey, what do you guys think? Similarly, a clinical leader noted that “Budget discussions tend to be led by finance. . . And it’s my opinion that that discussion would be best done by people with a clinical perspective, or people closest to patients, and/or patients themselves, starting from a place of what would be the best for us to do?”
A final area of concern was that wellness surveys must result in visible changes. One frontline worker advised her leaders to do more in that regard: “I think if I were in leadership and I was using those surveys, I would make it known that those surveys were being taken under consideration.”
In summary, we heard voices of both leadership and frontline staff acknowledging the challenge of rapid growth meant that more and better communication, greater emphasis on mission, and enhanced opportunities for staff participation were needed.
Part 2: Strategies to Mitigate Burnout and Moral Injury
The strategies identified by leaders and frontline staff largely aligned with the drivers described above, spanning: (1) strategies to address societal-level factors, (2) operational strategies to alleviate the workload caused by system-level factors, and (3) relational strategies to build trust and accountability at the organizational level. Most CHCs were engaged at all three levels. All four of the CHCs in our sample used external consultants and/or membership organizations to help them devise and/or implement their efforts.
The focus on workforce wellbeing was generally framed as helping to retain staff. Indeed, given the underfunding of CHCs and the corresponding difficulty of competing for new staff using just salaries, leaders and frontline workers alike talked about how critical retention is. One leader summed up the view of all the CHC leaders: “We have to prioritize the people that we have. We have to prioritize retention. We spend more resources, more money, more time, more energy, and more effort hiring and rehiring and retraining and everything. Why don’t we just invest in retaining the good staff members that we already have?”
Table 2 presents a summary of the specific approaches described by informants in relation to the drivers they identified.
Drivers and Approaches to Mitigating Burnout and Moral Injury.

Strategies to Reinforce Mission
All of the CHCs recognized the importance of emphasizing the organization-wide mission of addressing not just the healthcare needs of patients that presented at their clinics but also the broader imperative of social justice for their communities. Staff reported that this emphasis gave meaning to their work and provided a sense of belonging that helped mitigate moral injury. In one small CHC, this was accomplished by working to create a culture that closed the gap between the CHC and the community. In this case, they focused specifically on Indigenous values, although their approach could be applicable to other population groups. They describe their approach as: “A commitment to being unapologetically Indigenous. Our workforce development programs are really designed to train our native and next native-serving workforce. In other words, their workforce IS the community.
They describe this commitment as having gained momentum during COVID, when, with input from staff, they developed five core competencies “First and foremost is the commitment to Indigenous and organizational values, (then) collaboration, customer service, accountability, and communication.” These competencies are the centerpiece of a new orientation program for all employees called “7Gen”, that aims to foster an environment of trust, honesty, and transparency. “During the pandemic, we started a new onboarding program with our whole entire team and it’s a five-day deep intensive program into our organization. We talked about our core competencies, we talked about the history of the organization, we talked about native history, and urban native history specifically, and talked about all the things that are important to our organization, which are the foundation, of our Indigenous knowledge, an informed system of care, which we call Indigeknow.”
This is operationalized as the collective “why” they do what they are doing. “What we do as an executive leadership team is we share our whys, and so do our division directors, because we want people to know who we are, why we do this work, and what it takes when the work is challenging to care for yourself.” A participant echoed this perspective, as well: “As a participant, because I was a part of the last 7Gen, the shared ‘why’ really allows staff to realize they’re not alone.”
At a large CHC, wellness programs are guided and implemented by an external organization that tries to help them become more patient-focused. In doing this, they emphasize shared values across the c-suite and frontline personnel. “We can’t fully compete on the compensation side. So, we really, really do try to focus and attend to the mission orientation of the staff.” Another informant in the same CHC put it this way: “What we’re doing (here) is different than just showing up to do health care in a private practice or showing up to do health care in the hospital-based clinic. There is a mission here and a purpose that is deep and different, and that we are part of. As hard as it is at the end of a really bad day, we have been a part of something that is meaningful in people’s lives.” Consistent with the idea of a shared mission, this CHC provides training on structural racism. They have also organized visits for frontline staff to migrant camps. “We have folks tour migrant camps to really understand what our patients are experiencing and to see that firsthand, because sometimes they may just be experiencing things from the perspective of being in the Health Center.”
Another CHC (small) also emphasized training that strengthens the mission. “We have partnered with a group called X (name deleted), which was started around how to equip clinicians to practice in trauma-informed ways and have practical things that they can share with patients who really have an issue because of chronic stress.” They also offered training on LGBTQ+ issues and women’s health issues in response to requests that emanated from a monthly multidisciplinary advocacy meeting open to anyone. “Across the gambit, (we focus on) things that come up in our monthly multidisciplinary advocacy group. That, I think, helps a lot.”
Beyond looking outwards, the CHCs are addressing social determinants of health among staff too. Several CHC leaders spoke of the importance of creating a trauma-informed work environment for staff. A leader from this small CHC reflected: “Part of implementing a trauma-informed environment is recognizing that we all come from our own experiences of trauma, and we commit to not retraumatizing one another.” Similarly, the leader from a large CHC described developing training to help staff understand the trauma patients have experienced so that they are more empathetic. “Our strategy has really been educating our staff on,. . . what our patients go through, the discrimination that they face, so that when a patient shows up and the interaction is stressful, the staff member is not triggered.”
On-the-job training and staff development for career advancement were also mentioned by several centers as key to their success in minimizing burnout and improving retention. All of the CHCs informants viewed staff career advancement as part of serving the community. CHC leaders acknowledged that many of the people they invest in would subsequently seek jobs elsewhere. They viewed this acceptable because of their community-based mission. At the same time, they point out, career advancement helps reduce burnout and improve retention. One CHC leader reports “turnover at the clinician level has been very low, very low. . . and I think that is partially because of all of those workforce development programs. We’ve basically grown our own.” At another CHC, they partnered with one of the local community colleges that provides technical training for the medical assistants on site. “We pay them while they’re still in school. . . And once they get their certification, then can they agree to stay on for at least a year.”
As in most health care organization, these four CHCs have also used recognition programs, such as bonuses. However, across the four organizations a notable theme was that these programs were focused on collective, rather than individual, performance. The underlying argument they seemed to make is that recognition programs should be about mission, not simply transactional or aimed at operational fixes. If they are rewarding good economic performance, the recognition program is designed to share benefits. Thus, in the small Indigenous-focused CHC, they linked bonuses to collective goals that included proxies for well-being, such as turnover. “We have one overarching incentive program that is built on these key results (turnover, staff satisfaction, and financials) and each result translates to x percentage. So, the staff see that, and their driven to help ask questions around ‘what can we do to help’.” A leader explained: “We’ve been really clear with the staff when we have a profitable environment, we are always going to take care of them (through bonuses). We’re going to share with them.”
Strategies to improve operations. The efforts to address what was frequently described as “the overwhelming” workload constituted a second set of CHCs’ strategies to mitigate burnout. As reported in Part 1, leaders indicated they understood the double-bind of mission-driven work: the overwhelming workload reduces time with patients who need it most. This creates an imperative to find ways to alleviate the workload. Many of the specific measures implemented by CHCs focused on reducing the workload and giving people more time to do non-clinical work and more time off.
In this context, they talked about efficiency. “What it really is about is workflow efficiencies and time,” a leader in a small CHC reflected. She described their efforts to standardize workflows to reduce after-hours documentation burdens for clinicians: “We build out teams that not only provide ‘at the elbow’ support in workflows, but we standardize workflows. Using the Epic Language, we monitor very closely ‘pajama time’, which is a metric of how often people are on their quote-unquote ‘own time’ in the electronic health record.” A large CHC executive reported that they reduced clinician clinical hours and allowed more time off. “To address some of the burnout issues, we’ve reduced clinicians to four days a week, or even three days a week.” A third CHC executive described carving out and setting aside charting time and reducing the number of patients per provider per day. “We also offer charting times, we have two hours of charting time per day, . . . . and we only require our providers to have 16 encounters per day.” They moved them to four ten-hour work days a week during COVID, which worked so well that they decided to maintain the schedule. At the fourth CHC, they moved from 15-minute to 30-minute appointment times. They believe that this shift in scheduling paradoxically allowed them to see more patients. The executive reasoned as follows: “The system that we had before, there would always be one provider who was designated to take walk in, sometimes two. When I went back and analyzed how many walk-ins we were actually taking. . . it would be on average 5-6 per day. . . So, looking at that, I said, we weren’t really tracking productivity versus capacity. And so, when I looked at the hours that providers are in clinic, versus how many patients they’re actually seeing, I said, you know, even if they just saw 2 patients per hour, we will still see more patients.”
Three of the four CHCs described changing job roles to improve efficiency. At the first CHC, a leader described the process: “We had broken down every task that goes into a person coming for health care . . . and everybody with a different job description has a different colored sticky note. We said, ‘Please go put your color on the tasks that you do.’ Some tasks had four or five different job descriptions saying I think this is my job. And other tasks had nobody’s thing up there. And we’re ALL looking at it and thinking oh, obviously we need to do something about this.”
At the second CHC, a major bottleneck was the front desk, where patients had to wait in line to check-in. They trained their medical assistants to check patients in when they saw a line forming. They also implemented direct rooming for established patients. Lastly, they simplified forms and sent them via text or email to patients minutes after their appointment was made and in advance of their arrival for a visit.
In the third CHC, they focused on creating new opportunities for clinicians to provide care outside the center locations. “We created a work environment that is very varied and allows clinicians who are committed to the community health center movement to have many ways that they can serve in that capacity.” This, they believe, has helped reduce burnout.
Strategies to Improve Relationships
Leadership that we interviewed understood, each in their own way, that building trust with staff and moving beyond what one described as an “us vs them” mentality was essential to achieving workforce wellbeing. They also recognized that as CHCs grow larger, there are unique challenges of communication that they must address.
At one of the large CHCs, leaders report that they have intentionally focused on communication, which they describe as: “making people feel valued. . . A lot of what we found is . . . we think we’re talking up here and the message filters down, it dies somewhere in the middle.” At a CHC that is still small but has grown, they indicated that, as they expanded they have had to change the organizational structure to have more decentralized leadership, such that it is “directly connected with people in that region.” They tried an “open-door policy to encourage frontline staff to come to leadership with problems and suggestions.” However, they reported that they found this approach was disempowering direct supervisors. Instead, they now promote better team resolution of problems. “They needed to build some relationship with their supervisor in their team. And so, now, if they’re coming to me to tell me there’s an issue, I’ll say ‘Oh and did you talk to you know your supervisor about it?’ ‘Well, no, I haven’t told her.’ And I say, ‘Well I think this is important for her to know and I’m going to encourage you to go back and talk to her, sit down with her and tell her how this is affecting you, or the team, and see if you can come up with a solution.’ So, there’s a lot more of the direct working as a team, but also letting them know why.”
CHC leaders also emphasized the limits of their ability to solve problems and the importance of being honest with staff about it. One CHC leader explained, “If it’s something I can’t fix, I absolutely have to be able to be real, you know, (and explain the) legitimate reason why.”
All of the CHCs, both large and small, understood the importance of flattening the hierarchy and empowering staff to lead change. One CHC leader put it succinctly: “ Our staff says, ‘I’m overwhelmed, and they (the leadership) don’t understand me.’ So, creating the mantra that those who do the work (should) transform the work, and empowering them is critical.” At the indigenous-focused CHC, where both patients and employees are referred to as “relatives,” one of the leaders explained the importance of staff participation. “Every single person is incredibly important to the operation of services for our relatives. And it doesn’t matter if you’re the president and CEO, or if you’re a provider, or if you are on our environmental services team, or if you work in finance. It doesn’t matter. Every single person has an important spot in the circle. And we’re all, we’re all related. We’re all together.”
An important part of this trust-building is financial transparency. During this same CHC’s 5-day staff orientation, they describe this: “We also go over the financial health of our organization, like how we use money. . . all of those things that oftentimes people in clinical settings are just left out. This is a really powerful thing.”
The interviews suggested that staff empowerment is manifested in varied ways across the four CHCs. Still, in each case, they recognized that the operational changes were only meaningful if these relational changes accompanied them. The linking of the two domains was explicit. A CHC leader summarized it: “I think it’s working (workflow changes) because the staff felt heard.” They also described institutional mechanisms (system of meetings) that were implemented to make sure that staff felt heard, to position leadership as the support for department heads who, in turn, support frontline teams. The CMO describes an evolution in her role: “We went to a monthly meeting where I do 1-on-1s with each of the department heads, where we go over their action plan and we talk about how I can support them,. . . and then, we as a full team can see where everyone is on their action plan.” This same CHC combined institutional mechanisms with an explicit leadership style that empowers others. The approach uses data from staff engagement surveys to reflect on how leadership can improve. “Last year was a really in-depth employee engagement survey that was different from what they had done previously. And the survey looked at things like trust, if they feel that they’re treated fairly, if they trust their teammates, if they feel they have what they need to do their role.” With the help of a consulting group, these data were then used to inform leadership development training.
At a large CHC, they use Schwartz Rounds, 23 which they characterized as an effort “to really provide a space for connection and conversation and support.” They have also used a “What Matters to You” 24 methodology to better understand staff perspectives. Frontline staff described the experience as follows: “Basically, admin comes on site and they ask you, like, hey, what matters to you, what can we do? Which is great, except it’s kind of scary as a staff member. But it was good that they did that; I definitely appreciate it, and it makes me feel like, OK, well, ‘we’re trying to get some data to see what is it that we can fix, what can we work on,’ or even ‘you know what, that’s just not possible’. . . I feel like we have the space to share ideas.” The same CHC offered team-building exercises, which staff also appreciated. “I think it is so important - and this also contributes to the prevention of burnout in my opinion – that the organization is investing in team building exercises.”
The importance of strengthening relationships as a strategy specifically for reducing moral injury was mentioned by staff at another large CHC: “I think isolation, in the midst of being overwhelmed, is one of the things that leads to moral distress and burnout. And anything that helps build community in the midst of that experience, is an important piece to help change that.”
Another institutional approach used by one large CHC and is common across all kinds of healthcare organizations was the creation of a Wellness Council and a Chief Wellness Officer. The executive reported as follows: “We put a stake in the ground that we were going to make this a priority and created a chief wellness officer. . . It’s really a setting up an organizational structure where we hear what people are concerned with, and we work with them in an ‘empower with’ mentality rather than a ‘power over’ or ‘under’ to create a safer environment, but also one that is always listening and wanting to improve.”
They also offered mindfulness training. “We’ve partnered with a number of groups, but most recently out of Stanford with Compassion Institute and they give offerings that are virtual, small setting, meaning that they divide into small groups and have a facilitated kind of mindfulness approach.”
Leaders at all four CHCs felt that measurement of and accountability for employee wellness and engagement was important to track over time and that accountability to staff and the board regarding data use was also important. They all indicated that they reported data (administrative and survey) results to staff. The view from frontline staff in one large CHC that they did see how data were used to make improvements was acknowledged and understood by leadership there, and they indicated that they were working hard to show staff that survey results were informing decisions. Two CHCs also indicated that they reported data on turnover at the department level to their boards monthly and that these data were part of the CEO’s performance evaluation.
Discussion
Our interviewees identified drivers at the societal, health system, and organizational levels. Social drivers centered on the fact that the populations served by CHCs are severely disadvantaged. Several respondents said they saw the underfunding of CHCs as a reflection of society’s devaluation of the people they serve, and one linked this directly to structural racism. The moral injury they identified at this level occurred when staff felt they could not meet their patients’ needs. According to a scoping review of healthcare workers during COVID-19, this was a common finding in organizations where staff faced resource shortages and staffing constraints 25 similar to those observed in the CHCs in our study. Research from the UK’s National Health Service similarly found that systemic lack of funding left healthcare workers exposed to more situations of moral conflict such as being understaffed or lacking the medical equipment to care for patients. 26
The system-level drivers were related to the overwhelming workload staff experience due to factors such as pre-authorization, billing complexity, quality reporting, and the corresponding time spent on electronic health records. These tasks take time away from patient care, exacerbating the stress and potentially causing the moral injury associated with being unable to spend time with their patients. 27
Organizational-level drivers were also cited, including concerns about the rapid growth in some CHCs, which can cause a perceived distancing of leadership and staff, concerns about revenues becoming too much of a priority, and concerns that surveys did not necessarily lead to change. This aligns with a study that identified eroding trust and communication from leadership to be a significant concern for healthcare workers facing ethical challenges during the pandemic. Inconsistent policies and communication were determined to be key stressors, contributing to feelings of moral distress. 28
These drivers are similar to those identified in the HRSA 2022 survey, although the qualitative nature of our study provides greater detail. We note that these drivers are by no means unique to CHCs and have been documented in other healthcare settings well. 20
The burnout related strategies used by the four participating CHCs matched the drivers identified. We highlight five areas in which these four leading CHCs offered lessons to their peers, as summarized in Table 3. The first was that the mission of serving marginalized populations needs to be (a) explicitly inclusive of staff and (b) reinforced through workforce programs. Collective recognition programs (as opposed to, or in addition to, individual bonuses), as well as career development programs can form part of this principle. Informants reflected on the fact that many employees chose to come to and stay with their CHC because of its commitment to the community. As such, they believe it is important to continuously demonstrate the importance of mission to the leadership and to do so in a way that locates staff as part of, or in some cases allied with, the community they serve. This aligns with other research that found the “overwhelming importance of the CHC mission” 29 was the most important factor in the decision of participating physicians to work at a CHC and that “work for an organization whose mission I believe in” 29 was ranked as the most important factor for physicians’ workplace.
Lessons From CHCs.
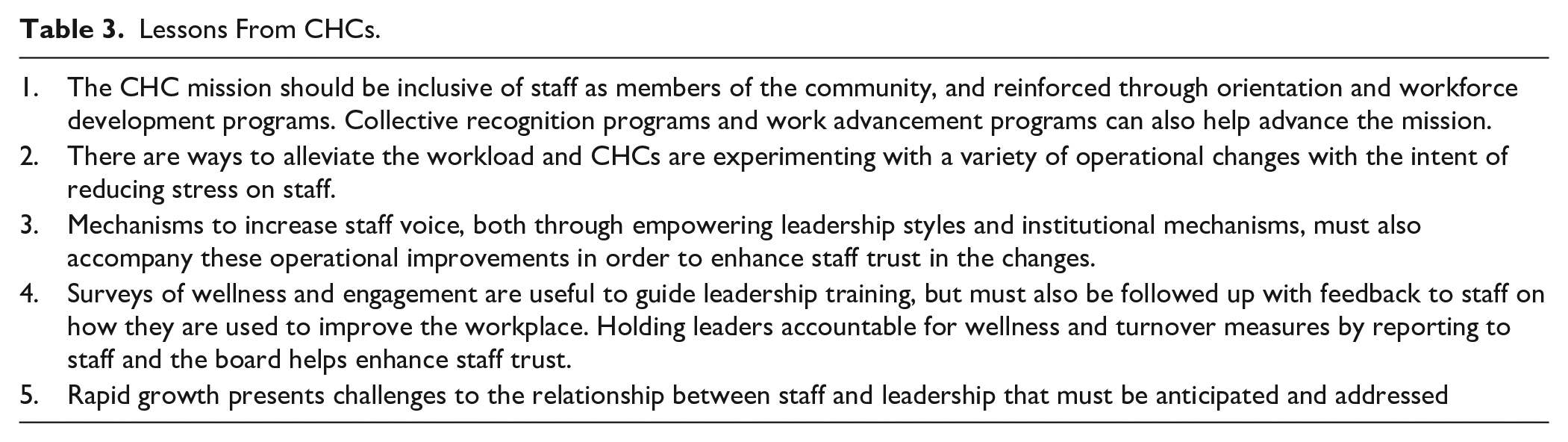
Second, informants described various efforts to improve efficiency as a means to alleviate the “overwhelming” workload. These included moving to a 4-day work week, extending visits from 15 to 30 minutes, making support staff roles more flexible so they could fill in for each other, and changing how check-ins and walk-in patients were managed. These measures suggest that the culture of “15-minute appointment” and “pajama time (after-hours administrative work)” for clinicians are not inevitable and that with staff participation, they were able to make changes. The perceived importance of improving efficiency tracks with other research that found that maintaining work/life balance was the highest-ranking factor among physicians at a Massachusetts CHC. 29 An additional study found that fairly shared workload and having sufficient funds and personnel were all associated with lower levels of burnout among CHC staff. 18
The third lesson that emerged from these interviews is that operational changes were insufficient; they had to be accompanied by efforts to improve relationships and create trust in the administration. This was accomplished by advancing a leadership style that empowers others to voice their views and participate in decisions. It also involves creating structures and normative processes that reduce hierarchies and enhance staff voice. Approaches included building all-staff training that advances an egalitarian organizational culture in which everyone is viewed as a relative, major investments in wellness structures that measure staff engagement, and continuously seeking ways to increase staff participation in organizational decisions. In each case, they understood that employee voice was a foundational building block for improving wellness and engagement and that operational fixes offered by the administration without staff input were insufficient. This idea is consistent with the most recent efforts to conceptualize moral injury in healthcare as relating to the perceived meaning of operational decisions.30,31
Fourth, all CHC informants agreed that measurement of, and accountability for, burnout and moral injury is critical. However, they also understood that staff must be able to see evidence that the data collected is used to create change. Frontline staff had mixed perceptions of the degree to which this is the case, suggesting that using data for decision-making and communicating that this was done is more complicated than it first appears. The two larger CHCs have taken the communication challenge seriously and made feedback on actions taken based on survey data a major area of work. Consistent and open communication from leadership within health care organizations has been found to be associated with reduced stress and lower burnout among healthcare workers. 32
The fifth lesson was that rapid growth creates staffing challenges and a perceived disconnect between leadership and staff. This is, again, consistent with prior research. A study of nurse practitioners in community health centers found that a better relationship with CHC administration was associated with decreased turnover intent and improved job satisfaction. 33 Grieving the loss of more intimate relationships appeared to be an inevitable part of organizational growth for the two larger CHCs, but, importantly, CHCs were aware of this and trying to address it. In one case, they were decentralizing authority regionally, and in the other, they had created a central wellbeing institute to service all sites.
This study has several potential limitations. First, based on our sample selection criteria, we focused on just four CHCs. While we reached theoretical saturation within this sample, a larger sample could produce different results, even if the size of the corpus of data would become less manageable. These are trade-offs typical in qualitative research. The sample was constructed from a national CHC conference hosted by the NACHC in early 2024, with four CHCs selected because they were considered leaders in this area by their peers, but also provided diversity in terms of geographic location and size. Second, consistent with a qualitative approach, we were interested in the perceptions of participants and did not directly measure burnout among participants or CHC staff. As such, we cannot assert a relationship between the strategies described and outcomes beyond the subjective claims of informants. Finally, the perceptions reported by informants may not be representative of the broader group of staff. In short, the value of this qualitative research is to elicit participants’ own accounts of their lived experiences, not to provide evidence that a particular strategy leads to improved outcomes.
Conclusions
The qualitative analysis of interviews with leaders and staff from four CHCs suggests that considerable thought and resources have been invested in reducing burnout and moral injury, especially since the COVID-19 pandemic. While each CHC developed its own set of programs to advance this work, there is a collective understanding that a staff-inclusive mission that is reinforced through programs is essential, that while operational improvements to workflow are necessary, they are insufficient, and that staff must feel heard. The approaches use different entry points, but they all aspire to elevate the voice of frontline health workers.
These are not entirely new ideas, for sure, but they stand in contrast to the dominant approach to addressing burnout that has been studied in other healthcare settings. The focus of most of the intervention research on addressing burnout in settings beyond CHCs has been on individual-level interventions—often training programs, apps, or peer support—that aim to increase resilience and manage burnout. Examples include Resilience in Stressful Events, 34 psychological first aid, 35 Stress First Aid, 36 mindfulness,37 -39 and others built upon evidence-based principles to improve resilience in managing stressful working conditions.40,41 Studies show mixed results, at best, for these types of interventions.37,38,42 As a result, many researchers and experts argue that organizational change is a more important approach to addressing burnout and moral injury and should be supported with funding and more research.43 -48 We note, in particular, a randomized trial conducted by Linzer et al 49 that showed that organizational strategies aimed at improving work conditions that were devised by primary care physicians, nurse practitioners, and physician assistants themselves resulted in less burnout and more job satisfaction compared to the control group.
The CHCs’ emphasis on creating leadership styles, institutional mechanisms, and a shared culture that includes staff as part of the mission and elevates employee voice in decision-making is, therefore, unusual in the literature on burnout. Notably, even in the one CHC that had implemented an individual-level wellness program (the Stanford mindfulness program), it was not viewed as central to mitigating burnout and moral injury. Rather, it was framed as an additional benefit, like tuition assistance or a flexible work week, which helped communicate the idea that employee well-being matters and is an integral part of the CHC’s broader social mission.
We find that the work these CHCs are doing is consistent with the conclusions of Linzer et al, 49 as well as the recommendations made by the National Academies of Medicine, 50 and the Surgeon General’s 48 recent reports on burnout among healthcare workers, that more emphasis on organizational change is needed. This study lays out a set of participatory organizational approaches that should be supported and studied more systematically.
Footnotes
Appendix A: Methodology for Literature Review
A comprehensive literature search was conducted using PubMed, PsycINFO, PAIS Index, Scopus, and Cochrane. The search strategy included keywords and Medical Subject Headings (MeSH) terms related to burnout, moral injury, retention, turnover, and interventions, specifically focusing on community health centers in the United States. Exclusion criteria included all papers published before 2003 that were not available in English and were not peer-reviewed. They were also required to study an intervention at a community health center in the United States. A total of 5712 papers were found with 2020 duplicates. Fifty-four were determined eligible for full-text screening, and five were found to fit the review criteria.
Appendix B: Interview Guide
Author’s Note
Samantha Meeker is also affiliated to Loyola University, Chicago, IL, USA.
Abbreviations
CHC: Community Health Center
HDC: Health Disparities Collaboratives
HRSA: Health Resources Services Administration
NACHC: National Association of Community Health Centers
Ethical Considerations
The George Washington University’s Office of Human Research determined IRB# NCR245546 to be exempt from IRB review under DHHS regulatory category 2.
Consent to Participate
An informed consent document was provided to participants. Consent was assumed through participation.
Consent for Publication
Verbal consent was provided for the included quotes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Bureau of Health Workforce (BHW), National Center for Health Workforce Analysis (NCHWA), Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $450,000, with zero percent financed with non-governmental sources. The contents are those of the author[s] and do not necessarily represent the official views of, nor an endorsement by HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
In order to maintain participant confidentiality, we are unable to share data.