
Abstract
Background
Failure to show up to a primary care appointment leads to disruption of the core purpose of primary care—continuous quality care over time. Missed appointments are a major source of inefficiency in the medical system and lead to poor control of chronic disease, later presentation to care, wasted health care dollars, and ineffective use of provider time. 1 -7 No-shows are a particular problem in primary care settings providing care to underserved populations and could be a contributing factor to poorer health outcomes in these groups. 8 -12 In 2012, Massachusetts General Hospital Chelsea HealthCare Center (MGH Chelsea) adult medicine practice had the highest no-show rate (16%) in the hospital’s primary care network. The objective of this study was to explore who were the patients not showing to the appointments at MGH Chelsea and their reasons for no-show.
Methods
The study was performed at MGH Chelsea, a community health center serving a predominantly Latino, non-English speaking and low-income population in Chelsea, Massachusetts. 13,14 The mortality rates in Chelsea for common chronic conditions such as coronary disease, diabetes, and cerebrovascular disease are higher than the state average. 13,14
All appointments for patients 18 years or older that were scheduled with primary care providers at MGH Chelsea adult medicine practice from March 23, 2012 to September 4, 2012 were included in the study. Using a daily generated list of eligible patients who had missed that day’s appointment, a bilingual (English/Spanish) patient service coordinator (PSC) attempted to call these patients the same or following day. The PSC documented the patient’s reported reason for missing the appointment, and these reasons were reviewed and categorized by the authors. Calls were made on weekdays from 6
Demographic data were collected on all adult patients’ who had scheduled appointments during the study period and analyzed using 2-sided t test of proportions to determine if race, ethnicity, language, gender, age, and insurance differed in patients who no-showed, compared with those who came to their appointments. Among patients who had no-showed, we also compared demographic characteristics of patients who were interviewed by phone to those who were not reached.
The unit of analysis was the no-show visit and patients that no-showed multiple times during the study period may have been called more than once.
Results
During the study period, there were 7508 scheduled appointments in the adult medicine practice. 1904 (25.4%) cancelled and rescheduled appointments were excluded from the analysis. Of the remaining 5604 appointments that were included, 844 patients did not show to 927 appointments (16.5%). There were 735 (79%) calls made to the patients who missed their appointments, and 273 (37%) were interviewed.
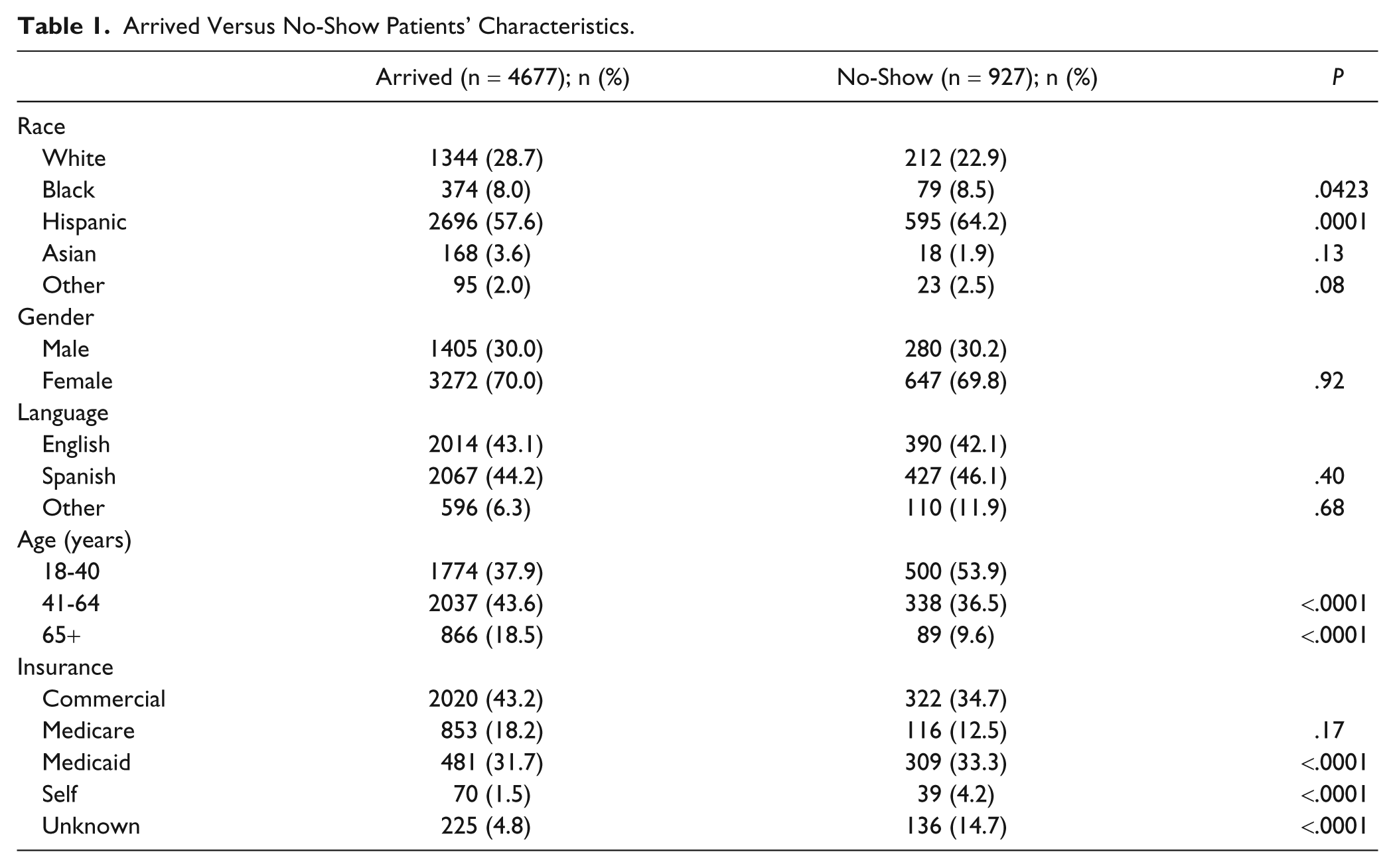
The patients who no-showed to their primary care appointments were younger (P < .0001), black (P = .0423) or Hispanic (P = .0001), and had Medicaid, self-insurance, or unknown insurance (P < .0001; Table 1).
Arrived Versus No-Show Patients’ Characteristics.
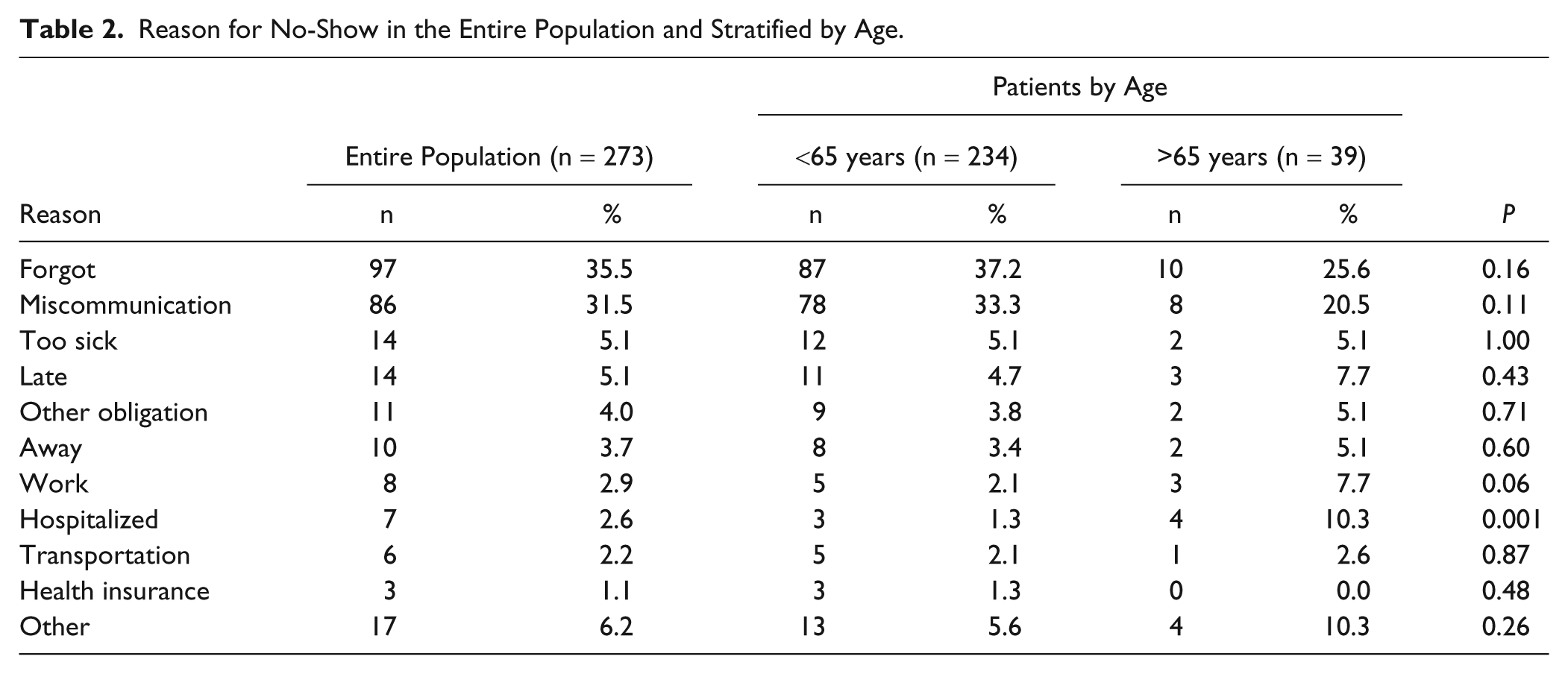
The 2 most common reasons patients cited for missing an appointment were forgetting (n = 97, 35.5%) and miscommunication (n = 86, 31.5%; Table 2). Comparing patients who the PSC was able to reach post no-show to those that were unreachable, we did not find statistically significant differences by gender, race, ethnicity, or language. However, the patients who responded to phone calls post no-show were more likely to be older than 65 years (14.3% vs 7.1%, P = .0004) and/or insured through Medicare (17.6% vs 10.6%, P = .0145). We further examined differences in reasons for no-show by age. Hospitalization was the only reason more likely to be reported among patients 65 years and older (P = .001; Table 2).
Reason for No-Show in the Entire Population and Stratified by Age.
Discussion
Our study revealed that in an adult medicine clinic caring for an underserved population, patients more likely to no-show to their primary care appointments were younger, black, Hispanic, and have Medicaid, or no known insurance. Patients missing appointments most commonly reported forgetting and miscommunication as their reasons to no-show. Similar reasons were reported in a general practice in the United Kingdom 6 and a military clinic in the United States. 15 The miscommunication category included patients who said they thought they had canceled the appointment, patients who thought the appointment was a different date or time, patients who tried to call the clinic but did not get through, and patients who did not realize they needed to call and cancel.
Several studies reported that non-English speakers were less likely to show to their appointment 2,9,11,12,16 -18 ; however, in our study, language spoken did not differ among patients who no-showed and those who came to their appointments. MGH Chelsea has 16 interpreters/outreach workers on site covering 13 languages, 19 and all PSCs and medical assistants at the clinic are bilingual as are many providers. Weather, a significant barrier in the literature, 20 was not noted in our study, probably because it was conducted during spring and summer.
Only 3 patients reported insurance as the reason for no-show. This may be because of the health insurance mandate in Massachusetts. 21 Patients with either unknown health insurance or self-insured were more likely to no-show. Because of the insurance mandate, it is possible that these represent patients who have only been receiving care at the clinic for a short time period, are nondocumented immigrants, and/or represent an even more vulnerable subset of the patient population that is particularly disconnected from the health care system.
Notable in the breakdown of reasons for no-show are the patients who reported hospitalization as their explanation. MGH and MGH Chelsea have an electronic system notifying both appointment schedulers and PCPs when a patient is hospitalized, thus allowing for coordination of perihospitalization care. Because of this system, hospitalization should never lead to no-shows. A potential explanation is hospitalization at a nonaffiliated medical facility, which would not activate the notification system and would require the patient to contact the clinic and cancel their appointment. A possible solution would be coordination among Boston area hospitals to notify PCPs when a patient is admitted. Although this occasionally happens on an individual basis, the system is not formalized.
Several important limitations warrant consideration. The data were analyzed retrospectively. Our results, from an urban community health center affiliated with an academic hospital, may not be generalizable to other clinical settings. However, this study demonstrates that providers can study their practices and use the results to improve patient care. No-shows were defined by appointment and not patient, so if a patient no-showed multiple times during the study period, these would be captured as individual no-show events. The reason for no-show was patient reported with no way of verifying accuracy of report. The calls were made by a PSC working in the same practice, so patients could have felt uncomfortable sharing their reason for no-show with someone associated with their provider. However, we chose an experienced PSC, Latina, from the same community, and whom patients trust and often share personal information with.
Although patients were not called on all days during the study period, in 79% contact was attempted; however, only 37% of patients who no-showed were actually reached. It is possible that the results would differ if a larger sample of the population were captured. Comparing the demographic characteristics of no-shows who were reached by phone to those who were not, the only difference we found was that patients reached were more likely to be older and/or insured by Medicare. In the 65 years and older group, the only reason for no-show more often mentioned was hospitalization. Because of limited resources, calls were made for only 2 hours in the evening hoping to reach patients who might not have showed because they missed the routine reminder call, which is made in the morning. Patient with irregular work hours or nighttime obligations could have been missed with this approach and they might have provided different reasons for no-show.
With the results demonstrated in this analysis, interventions directed toward the listed reasons for no-show can be designed and implemented, 9,22 -25 To target forgetfulness and miscommunication mentioned by 66% of patients in our study, we will evaluate 2 new interventions to improve attendance to primary care appointments at MGH Chelsea. Patients will receive 2 text messages or, if they are deemed to be at high risk to no-show, an additional reminder call will be made 7 days prior to their appointment. We will conduct a randomized control trial to evaluate which intervention is the most effective in our population.
Understanding the demographic characteristics associated with no-show such as age, ethnicity, and insurance type can also inform the creation of interventions to decrease no-shows. 2,4,9,11,12 For providers, it is helpful to know who is more likely to no-show and why, so that obstacles to coming to appointments can be addressed on an individual level. Examining reasons for no-show on an individual practice level is an important first step. Exploring different methods to reduce the no-show rate is needed to increase access to quality primary care and reduce health disparities. 4,9,22,26,27 While the results of this study can help guide the design of interventions aimed at decreasing no-shows, future studies are needed to determine the most effective method to improve attendance to primary care appointments.
Footnotes
Acknowledgements
The authors would like to thank Janet Santiago, patient service coordinator, who made phone calls and recorded patient reason for no-show, Patrick Ryan Cronin for assisting with biostatistical analysis, and Steven J. Atlas, MD, MPH, for reviewing the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Harvard Medical School Center for Primary Care Academic Innovations Collaborative Grant.
Author Biographies