
Abstract
Introduction:
Depression is a prevalent, debilitating, and potentially life-threatening disorder that affects millions of people worldwide and is influenced by multiple factors.
Objective:
To examine the influence of sociodemographic, socioeconomic, and health-related factors on depression in the Peruvian adult population using data from a nationally representative survey conducted between 2020 and 2022.
Methods:
A descriptive analysis of the variables was conducted, followed by a bivariate analysis using the Chi-square test with the Rao-Scott correction. Subsequently, a multivariate analysis was performed using a Poisson multiple regression model with robust variance to estimate adjusted prevalence ratios (aPR) and their corresponding 95% confidence intervals.
Results:
The study included 72 334 participants aged 18 to 97 and identified an increased likelihood of depression among older adults (≥60 years; aPR = 1.18 [1.08, 1.29]); single individuals (aPR = 1.33 [1.22, 1.45]); separated individuals (aPR = 1.32 [1.18, 1.47]); divorced or widowed individuals (aPR = 1.44 [1.34, 1.56]); residents of the Sierra region (aPR = 1.41 [1.30, 1.53]); economically inactive individuals (aPR = 1.08 [1.01, 1.16]); individuals with disabilities (aPR = 1.50 [1.28, 1.77]); those diagnosed with hypertension (aPR = 1.45 [1.33, 1.58]) or diabetes (aPR = 1.42 [1.27, 1.59]); and those who smoke monthly (aPR = 1.32 [1.19, 1.48]). Conversely, being male (aPR = 0.50 [0.46, 0.54]), having a higher level of education (secondary or above; aPR = 0.69 [0.62, 0.76]), residing on the coast (aPR = 0.83 [0.76, 0.91]) or in the jungle region (aPR = 0.87 [0.79, 0.96]), living in a rural area (aPR = 0.85 [0.78, 0.93]), and having a higher wealth index (aPR = 0.81 [0.71, 0.94]) were associated with a lower likelihood of depression.
Conclusions:
In conclusion, depression is significantly associated with various sociodemographic, socioeconomic, and health factors.
Introduction
Depression is a common mental disorder that negatively affects the way individuals feel, think, and act. 1 It is generally characterized by persistent sadness, loss of interest in usual activities, fatigue, and cognitive impairment, which together can severely interfere with daily functioning and quality of life. 2 According to the World Health Organization (WHO), 3 an estimated 3.8% of the global population suffers from depression, including 5% of adults (4% of men and 6% of women) and 5.7% of adults aged 60 and over. In the Americas, the Pan American Health Organization estimates that approximately 5% of the population experiences depressive symptoms, with a greater burden observed among women. 3 Within South America, countries have reported some of the highest rates in the region, with increasing trends over the last decade. 4 In Peru, the Ministry of Health (MINSA) reported 247 171 diagnosed cases of depression in 2022. Among these, 75.24% were women and 17.27% were minors, showing an unequal burden by sex and age. 5 The National Institute of Mental Health (INSM) also recognizes depression as a public health priority, estimating a prevalence ranging from 6% to 10% in the population. 6
The prevalence of depression is influenced by various sociodemographic factors, with notable differences by sex: women tend to experience higher rates of depressive symptoms, often attributed to hormonal and psychosocial factors, whereas in men, depression is more commonly linked to socioeconomic conditions.7 -10 Age is also a predisposing factor, as older adults are more likely to develop depression due to social isolation, chronic illnesses, and the loss of loved ones.11,12 Similarly, a low level of education is associated with a higher risk of developing depressive symptoms.8,12,13 The natural region of origin and ethnicity may increase the risk of discrimination, cultural barriers, and limited access to mental health services, all of which can contribute to the onset of depressive symptoms. 14 In rural areas, restricted access to healthcare and education, along with low income and social isolation, can also contribute to the development of these symptoms. 12
Other studies have shown that individuals from disadvantaged socioeconomic backgrounds are more likely to experience chronic stress, financial instability, debt, and limited access to mental health resources, all of which contribute to the development of depression.8,13,15 This finding has also been reported in studies involving older adults, such as the one conducted in China by Zhou et al, 16 which found that low socioeconomic status is significantly associated with a higher prevalence of depressive symptoms. Similarly, individuals with chronic physical conditions—such as diabetes, cardiovascular disease, and multimorbidity—are also at increased risk.17 -19
Multiple studies indicate that low income, low educational attainment, and unemployment are associated with higher rates of depressive symptoms, making individuals with a disadvantaged socioeconomic status particularly vulnerable to this condition.20 -22 These findings highlight the need to reduce socioeconomic inequalities through policy reforms, enhance mental health services, and combat stigma surrounding mental health. These actions are essential to strengthening mental well-being and mitigating the impact of depression on individuals and communities.
On the other hand, studies analyzing factors associated with depression in national surveys, such as the study by Daray et al 23 in an adult population from three Latin American countries (Argentina, Chile, and Uruguay), 23 found that higher depression levels were associated with sociodemographic factors (being a woman and aged between 35 and 44 years) and health factors (current smoking and a history of chronic diseases). Conversely, lower depression levels were associated with higher education and being cohabiting or married. In Peru, Hernández-Vásquez et al 24 analyzed the 2018 Demographic and Family Health Survey (ENDES) and found that sociodemographic factors associated with a higher prevalence of depressive symptoms included being a woman and older age. Health-related factors included having diabetes mellitus, high blood pressure, and a history of disability. Conversely, sociodemographic factors associated with lower depression levels included being married or cohabiting and having at least a secondary education. The only socioeconomic factor linked to lower depression was economic well-being (quintiles 3-5).
Although a decrease in depressive symptoms might have been expected following the acute phase of the COVID-19 pandemic, the prevalence of depression has remained high—or even increased—in many populations, including in Peru. This persistence can be attributed to multiple ongoing and cumulative factors, such as prolonged economic instability, rising unemployment, weakened social support networks, and chronic stress resulting from food insecurity, domestic violence, and limited access to mental health services. 25 Furthermore, the psychological after-effects of confinement, unresolved grief, and information overload may have had long-term consequences on the mental health of the population. 26 Therefore, it is essential to consider these structural and social factors when analyzing the sustained increase in depression following the pandemic.
Although some studies have explored the factors associated with depression in Peru, there is still limited research that comprehensively examines the interplay between sociodemographic, socioeconomic, and health-related variables. For instance, Rautio et al 27 evaluated this association in a sample of older adults but focused solely on wealth level as a socioeconomic factor. Other studies have investigated these relationships using national survey data; however, they often analyzed the variables separately or within isolated years.23,24 These limitations restrict the generalizability and integrative understanding of depression’s social determinants. Therefore, the present study is relevant because it simultaneously assesses multiple sociodemographic (sex, age, education, marital status, region, and area of residence), socioeconomic (wealth index and economic assets), and health-related factors (insurance status, disability, hypertension, diabetes, smoking, and alcohol use) in a nationally representative sample of Peruvian adults, using data collected across 3 consecutive years (2020-2022). This approach allows for a more robust and comprehensive analysis of the determinants of depression in the Peruvian context.
Methods
Design
This study employed a cross-sectional and analytical design based on secondary data. The analysis was conducted using data previously collected by the Demographic and Family Health Survey (ENDES), a national survey carried out annually by the National Institute of Statistics and Informatics (INEI). As this is a secondary data analysis, no direct data collection or surveying was performed by the authors. The study is also retrospective in nature, as the events analyzed occurred before the initiation of the present investigation.28,29
Participants
The study population consisted of Peruvian adults aged 18 years and older, selected from ENDES data collected between 2020 and 2022. ENDES is a nationally representative survey that covers all 25 regions of Peru and includes private households and their members. Its sampling design includes women aged 15 to 49, children under 5, and at least 1 household member aged 15 or older.
For this study, a total of 72 334 adults who completed the health questionnaire in the 2020, 2021, or 2022 survey waves were included in the final analysis (see Figure 1).
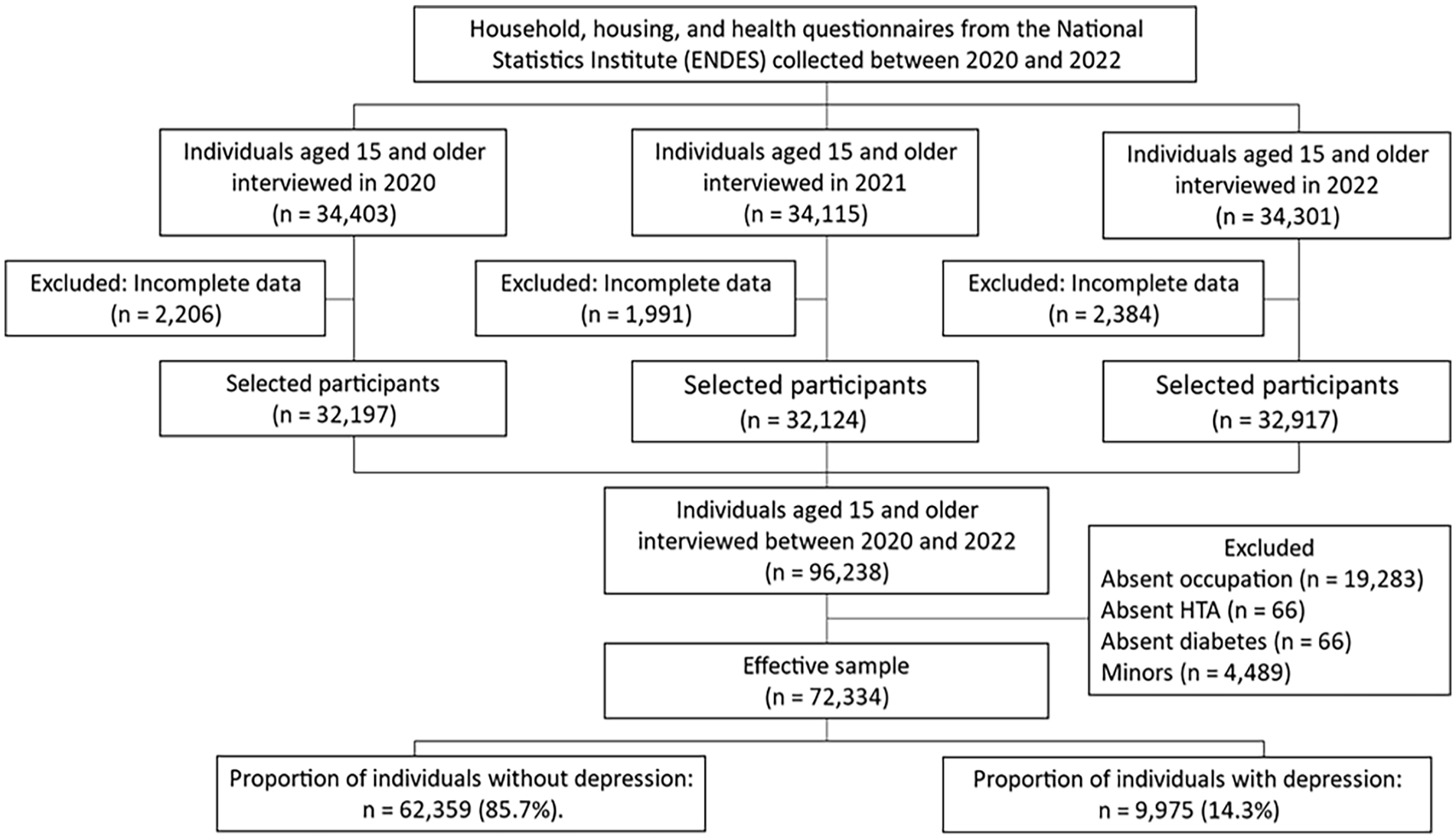
Flowchart of the sample selection process.
Variables of the study
The dependent variable, depression, was measured using the Patient Health Questionnaire (PHQ-9), located between questions QS700A and QS700I of the health questionnaire (CSSALUD01) in the Spanish National Health Survey (ENDESA). 30 It consists of 9 items with a Likert-type response scale ranging from 0 (not at all) to 3 (almost every day), with total scores ranging from 0 to 27. Higher scores indicate greater depressive symptomatology. The scale demonstrates adequate psychometric properties for the Peruvian population. 31 A cutoff score of ≥7 was used to define clinically significant depressive symptomatology. 32 For the present study, internal consistency reliability was calculated using the full sample across all years included, yielding a satisfactory McDonald’s omega coefficient (ω = .882).
The independent (exposure) variables were categorized into 3 groups:
(a) Sociodemographic factors: Sex (female, male), age group (young, adult, elderly), educational level (primary or lower, secondary, higher), marital status (single, married or cohabiting, separated or divorced, widowed), natural region (Metropolitan Lima, rest of the coast, highlands, jungle), and area of residence (urban, rural).
(b) Socioeconomic factors: Economic activity (yes, no) and wealth status (very poor, poor, average, rich, richest). These categories are based on the classification developed by the National Institute of Statistics and Informatics (INEI), the central and governing body of the National Statistical System in Peru. INEI is responsible for regulating, planning, directing, coordinating, and supervising official statistical activities in the country, including the classification of socioeconomic levels through methodologies based on national surveys.
(c) Health factors: Health insurance (no, yes), disability (no, yes), diagnosis of high blood pressure (no, yes), diagnosis of diabetes (no, yes), monthly smoking (no, yes), and monthly alcohol consumption (no, yes).
Additionally, the year of the survey was recorded (2020, 2021, 2022).
Data analysis
This study conducted a secondary analysis of ENDES data from 2020 to 2022. For this analysis, the databases for the required years were first downloaded from the ENDES web portal (https://proyectos.inei.gob.pe/microdatos/) and imported into the open-source statistical software RStudio (v. 4.0.3). They were then merged with the databases for the health survey (CSALUD01), household (RECH23), and housing (RECH0, RECH1, and RECH4). This was performed using the survey package (v. 4.0) and the svydesign function, which enabled data linkage at both the household and individual levels using the variables HHID and QNUMBER, respectively. To ensure greater representativeness of the results, the Primary Sampling Unit (HV001), stratum (HV022), and sample weight (PESO15_AMAS) were included as design variables.
The descriptive analysis of the categorical variables was calculated with the values of absolute frequency and the weighted proportions, while for the numerical variables the mean (M) and standard deviation (SD) were used. For the bivariate analysis of factors associated with depression, the Chi-square test (χ²) with a Rao-Scott correction was used. This correction accounts for standard error and confidence interval adjustments when analyzing complex survey data. Finally, a multivariate analysis of the factors influencing depression was conducted using a Poisson multiple regression model with robust variance, yielding adjusted prevalence ratios (aPR) with 95% confidence intervals. To ensure acceptable multicollinearity, the Variance Inflation Factor (VIF) must be less than 2.
Ethical Considerations
This research did not require ethics committee approval, as the data is publicly available on the INEI website. This institution obtains the consent of each participant during the evaluation process, ensuring that all information is collected confidentially and that the anonymity of the individuals involved is respected.
Results
Characteristics of the Population
The study included 72 334 Peruvian participants of legal age, ranging from 18 to 97 years (M = 42.3, SD = 16.9). There were more women (52.6%), adults aged 30 to 59 (54.5%), and individuals with secondary education (42.9%). Additionally, 14.4% (13.9-14.8) experienced depressive symptoms. For a more detailed analysis, see Table 1.
Characteristics of the Participants.
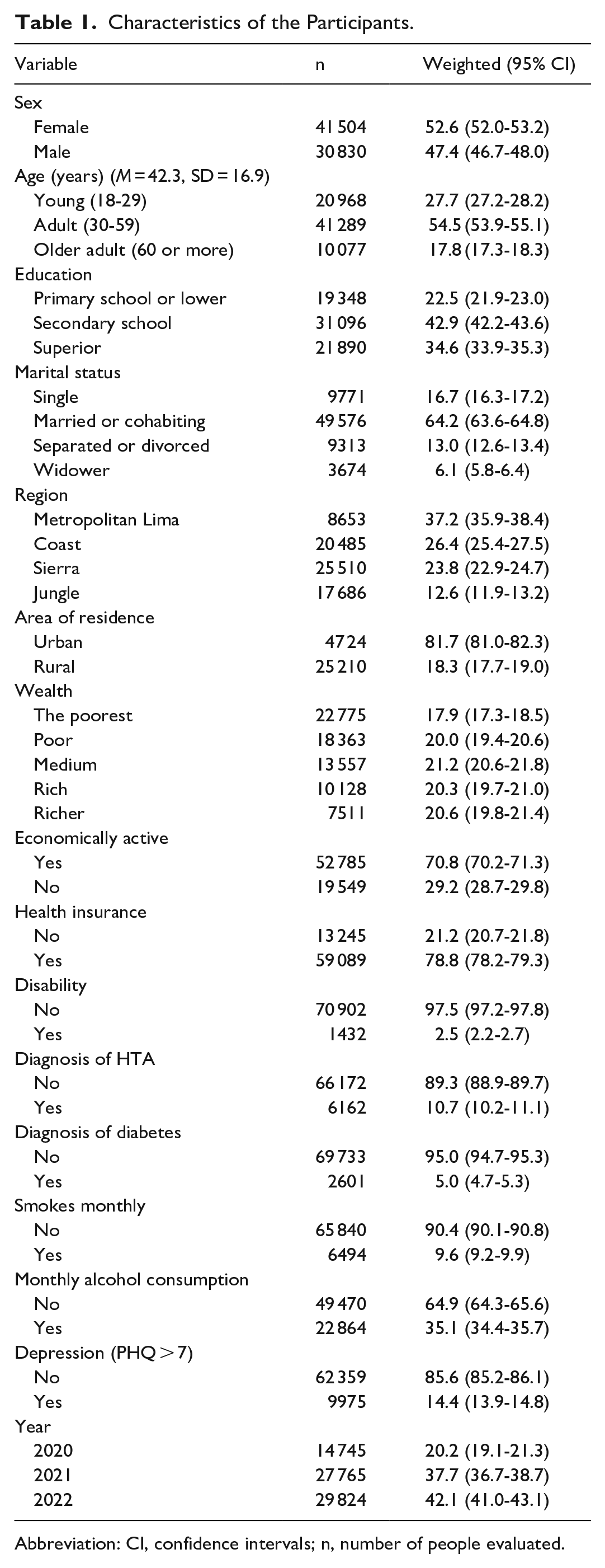
Abbreviation: CI, confidence intervals; n, number of people evaluated.
Bivariate associations
The bivariate analysis revealed significant associations between depression and sociodemographic factors such as sex, age, educational level, marital status, region, and area of residence (P < .05). Similarly, significant associations were found for socioeconomic factors such as wealth and economic activity, as well as health factors including health insurance, disability, HTA diagnosis, diabetes diagnosis, and monthly smoking (see Table 2).
Bivariate Associations Between the Exposure Variables and Depression.

Abbreviation: P, level of significance.
Multivariate analysis
The Poisson regression model with robust variance revealed that the following characteristics were associated with a higher prevalence of depressive symptoms: being an older adult (60 years or older), being single, separated/divorced, or widowed, residing in the sierra region, not being economically active, having a disability, being diagnosed with hypertension, having diabetes, and smoking monthly. Conversely, being male, having a higher level of education (secondary or above), residing in the coastal or jungle regions of Peru, living in rural areas, and having a higher wealth status were all associated with a lower prevalence of depression. It is important to note that no multicollinearity issues were identified, as the VIF was below 2 in all cases (Table 3).
Adjusted Prevalence Ratios of Factors Associated With Depression.
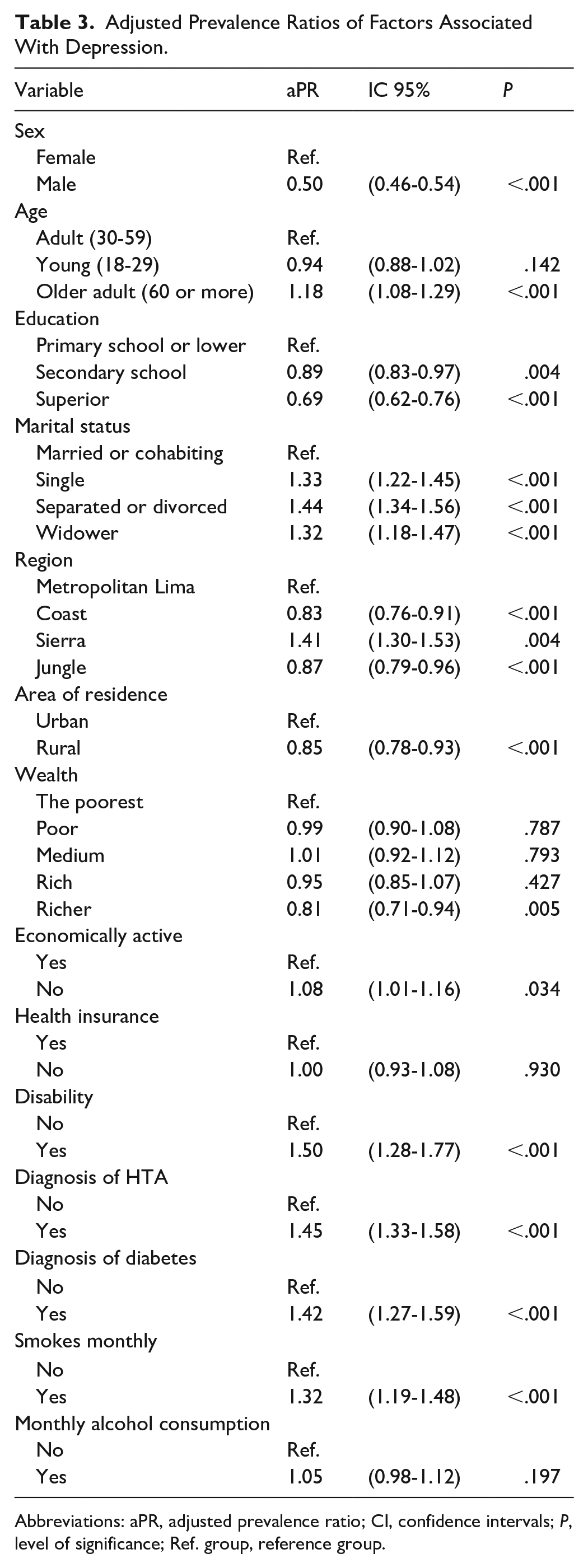
Abbreviations: aPR, adjusted prevalence ratio; CI, confidence intervals; P, level of significance; Ref. group, reference group.
Discussion
Depression has become a significant global public health issue, driven by a range of complex and multifaceted factors. 33 Despite advances in understanding this issue, there remains a critical need to identify and examine the factors that contribute to depression, as these may vary depending on sociodemographic, socioeconomic, and health-related contexts. This study aimed to explore the influence of such factors on depression using data from a nationally representative survey conducted between 2020 and 2022.
One of the most significant findings of this study is that depressive symptoms are influenced by a range of sociodemographic, socioeconomic, and health-related factors. Specifically, among sociodemographic factors, being an older adult (60 years or older), being single, separated/divorced, or widowed, and being from the sierra region were identified as factors that increase the likelihood of depression. These results align with other studies that have reported that aging, social isolation due to marital status, and the unique geographical and cultural conditions of the sierra region contribute to a higher risk of developing depressive disorders.34, 35 Living conditions in the sierra region, often marked by geographical isolation, limited economic opportunities, and restricted access to healthcare services, tend to exacerbate vulnerability and increase the risk of depression. 36 According to the WHO, 37 older adults may be more vulnerable to depression due to a reduced social support network and the presence of chronic illnesses. Additionally, factors such as marital status, particularly being widowed, were found to be associated with feelings of loneliness and loss, which increase the likelihood of depressive symptoms. 38
Regarding socioeconomic factors, individuals who were not economically active exhibited a higher prevalence of depressive symptoms. This finding aligns with other research, which confirms that depressive symptoms are more common in individuals who have lost their jobs or have been unemployed for extended periods, compared to those with any form of employment, including informal or temporary jobs. 39 However, the relationship between economic problems and depression is bidirectional, as depression can exacerbate financial difficulties, creating a harmful cycle in which economic issues and mental disorders reinforce one another. 40
In the third analytical group, health-related factors such as a diagnosis of hypertension, the presence of diabetes, and monthly smoking were associated with a higher prevalence of depressive symptoms. These chronic conditions not only impose a significant physical burden but may also contribute to or exacerbate mental health issues. Hypertension and diabetes, both complex diseases with potentially serious complications, can increase levels of stress and anxiety, contributing to the development of depressive symptoms. 41 Similarly, smoking, particularly when persistent, has been associated with a higher incidence of depression, possibly due to the neurochemical effects of nicotine and the lifestyle factors linked to smoking. 42
On the other hand, certain variables were identified as being associated with a lower prevalence of depressive symptoms. In particular, being male was linked to a reduced risk, which is consistent with previous research indicating that women are at significantly higher risk due to biological, hormonal, and psychosocial factors.23,24,27 Another protective factor identified was a higher level of education (secondary or higher), as education not only provides cognitive and social resources but also grants access to better job opportunities and support networks, which are considered protective against depression.43,44 Furthermore, residing in regions of the Peruvian Coast and Rainforest was associated with a lower prevalence of depression compared to other areas. Although these regions are often less economically developed, they may offer a lifestyle more connected to nature and less stressful. 45 Similarly, living in rural areas was associated with a lower prevalence of depression, likely due to reduced exposure to stress and stronger community support networks. 46 Finally, a higher level of wealth was associated with a lower prevalence of depression, as it provides economic stability and facilitates access to better health services, housing, and an overall higher quality of life. 22
Depression clearly increased from 2020 to 2022 among participants, with prevalence rates of 20.2% in 2020, 37.7% in 2021, and 42.1% in 2022. This indicates that the prevalence of depressive symptoms has doubled in just 2 years. One primary reason may be the prolonged impact of the COVID-19 pandemic, which brought adverse factors such as mandatory confinement, social isolation, and increasing economic and health uncertainty—each of which has had lasting effects on mental health and contributed to sustained levels of depression.36,47
Limitations
It is important to acknowledge the limitations of this study. First, it focuses on the general population and does not include a significant number of economically active individuals or those with specific characteristics. Secondly, our research does not account for changes in participants’ depression over time, as an observational approach was used and the participants varied each year. Consequently, it was not possible to assess longitudinal changes in the analyzed sample. Finally, in our study, the PHQ-9 was the sole measure used to assess depressive symptoms. It is possible that using other depression scales, such as the Reynolds Depression Scale or the Beck Depression Inventory, which cover a broader range of depressive symptoms, could have yielded different results. However, we believe that the PHQ-9 captures the core indicators of depressive symptoms as outlined in the DSM-5. Therefore, using other scales would have provided additional information on symptoms not specific to depression.30,32
Additionally, it is important to recognize the limitations associated with the use of secondary data from national surveys. First, we had no control over how the data were collected, and some variables may be affected by measurement errors or reporting bias, especially self-reported data on depressive symptoms and health status. Second, certain relevant variables—such as history of mental illness, social support, or access to mental health services—were not available in the dataset, which may have influenced the results and limited the scope of our analysis. Lastly, secondary databases are susceptible to recall bias and social desirability bias, particularly in mental health assessments, which may underestimate or distort the true prevalence and associations observed.
Conclusion
In conclusion, this study highlights the sociodemographic, socioeconomic, and health-related factors that influence depression among Peruvian adults. The findings indicate that being an older adult, being single, residing in the highlands, having hypertension or diabetes, and smoking are associated with a higher likelihood of experiencing depressive symptoms. In contrast, higher educational attainment, rural residence, and greater wealth are linked to a lower prevalence of depression. The significant increase in depression levels from 2020 to 2022, partly due to the prolonged impact of the COVID-19 pandemic, underscores the need for comprehensive interventions.
Footnotes
Ethical Considerations
This research did not require ethics committee approval, as the data is publicly available on the INEI website.
Consent to Participate
The INEI obtains consent from each participant during the evaluation process, ensuring that all information is collected confidentially and the anonymity of individuals is respected.
Consent for Publication
Not applicable.
Author Contributions
MB-D conducted the statistical analysis, designed the methodology, and drafted the initial manuscript. MB-D and J-AM-G collaborated on data analysis, interpreted the results, and revised the manuscript. JS contributed to the statistical analysis and played a key role in drafting and refining multiple manuscript versions. All authors reviewed and approved the final version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Señor de Sipán has provided institutional support for the article processing charge (APC) related to the publication of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated to support the findings of this study are not publicly available, but can be requested from the corresponding author.