
Abstract
Improving the health system for the future will include developing and successfully implementing programs to improve the health of populations and communities. Programs that successfully engage individuals in their health and health care have intrigued policy makers, communities, health plans, and providers for many years. The Patient Protection and Affordable Care Act of 2010 included funding for demonstration projects to encourage behavior modification for healthy lifestyles among Medicaid beneficiaries and determine scalable solutions. 1 This article contributes to the knowledge base about incentive programs by examining early experience from one of the first incentive programs targeting Medicaid beneficiaries—Florida Medicaid’s Enhanced Benefits Rewards (EBR) program.
Florida’s Enhanced Benefits Rewards Program
Florida’s EBR program was designed to incentivize beneficiaries to take an active role in their health and health care through engaging in certain health-related behaviors. Beneficiaries can earn up to $125 in credits annually for participating in health-related activities, including checkups, childhood immunizations, mammograms, pap smears, colorectal screenings, and wellness activities outside of the clinical setting.2,3 Beneficiaries must actively seek out, enroll, and successfully complete the activity, as well as submit documentation to their health plan to show that they have participated. All credits earned can be used to purchase items at Medicaid-approved pharmacies, including vitamins, diapers, over-the-counter medicines, and other items. 2
Between the program launch in September 2006 and May 2010, more than 170 000 Florida Medicaid beneficiaries earned credits totaling approximately $28.3 million (Table 1). 3 Of credits earned, beneficiaries spent $14.2 million to purchase over-the-counter items from approved Medicaid pharmacies.
Top 10 “Healthy Behaviors” in Florida Medicaid’s Enhanced Benefits Rewards Program, 2006-2010. a

Source. Agency for Health Care Administration (2010). 3
Through May 5, 2010.
Despite initial large numbers of EBR credit earners, awareness and participation in the program may vary among Florida Medicaid beneficiaries. Qualitative interviews conducted with Medicaid beneficiaries reveal that some would find a monetary incentive sufficient motivation to engage in healthy behavior, but other beneficiaries would not.4,5 Furthermore, differences in program participation could be attributed to levels of knowledge about the program’s existence and levels of inclination to participate.
Florida’s EBR program is part of a national trend toward greater consumerism within health care and increased efforts to encourage consumers to take personal responsibility of their health. 6
Incentive programs such as Florida’s can only be successful to the extent that patients or consumers (a) are aware that such programs exist, (b) take action and perform the designated health behaviors, and (c) use earned credits in some way. To inform development and implementation of other programs aimed at incentivizing healthy behaviors, this study focuses on potential factors associated with knowledge of and participation in Florida Medicaid’s EBR program.
Methods
This study is a cross-sectional analysis of surveys of Florida Medicaid beneficiaries who were eligible to participate in the EBR program. Eligible participants lived in 5 counties (2 urban and 3 rural) that were part of larger 1115 waiver demonstration program occurring at that time. Questions were added to the Medicaid Health Plan Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys in order to track awareness and use of the EBR program. This analysis uses the responses from 2009 since by then the EBR program had been operational for approximately 3 years and had reached a period of stability in enrollment growth.
The sampling frame for the survey was based on Florida Medicaid administrative eligibility files. To be eligible for the survey, an enrollee had to be enrolled in Medicaid for at least 6 consecutive months. Individuals who were dually eligible for Medicare and Medicaid, live with a developmental disability, or were residents of nursing homes or hospice were excluded from the sampling frame. Study participants were randomly selected based on county and plan characteristics and surveyed via telephone by interviewers at the University of Florida Survey Research Center. Parents completed the survey on behalf of their children. The University of Florida Institutional Review Board approved this research.
A total of 6904 interviews were completed with a response rate of 46%. We compared respondents with nonrespondents using data from the member-month and eligibility files. Distributions of the 2 groups did not differ in a statistically significant way with respect to race/ethnicity, gender, Medicaid eligibility category, type of managed care plan, and county of residence. The cooperation rate (ie, the proportion of respondents contacted who actually completed the survey) is 76%. In our analyses and in making population estimates, we weighted the sample to reflect plan share in each county and survey nonresponse.
Three outcome variables were derived from the survey. All respondents were asked (a) if they had heard of or were aware of the EBR program. If the respondent answered yes, they were then asked (b) if they participated in an approved activity. Respondents who indicated they participated in an activity were then asked (c) if they redeemed a credit. Study investigators created these items and, prior to survey implementation, asked a pilot group of Medicaid beneficiaries if they understood the questions. As a result of the pilot, modifications were made in the wording of the items, specifically, adding phrase describing the EBR.
Our analytic samples excluded individuals who did not respond to the EBR questions. Sixty-seven people did not respond to the initial question on whether they were aware of the program reducing the initial analytic sample to 6837. Individuals who were not aware of the program were not asked if they participated in an activity. Similarly, individuals who had no participation were not asked if they redeemed a credit.
Factors associated with knowledge of and participation in EBR included sociodemographic characteristics, health status of beneficiary, and health system characteristics. Sociodemographic characteristics include language spoken at home (English, Spanish), Hispanic ethnicity (yes, no), race (white, black/African American, other), educational attainment (no high school diploma, high school graduate or general education diploma [GED], some college) and age (younger than 18 years or 18-65 years). Health status was assessed by respondent self-report (excellent, very good/good, fair/poor). Health system characteristics included whether the beneficiary had a personal doctor (yes, no), number of visits made to the doctor in the past year, plan type (in a Provider Service Network (PSN) or Health Maintenance Organization for 6 months continuously, switched health plans within past 6 months), and county of residence (Broward, Duval, rural counties). Sociodemo-graphic characteristics, health status, presence of a personal doctor, and number of visits to a doctor were standard CAHPS items. 7 The CAHPS are a family of standardized instruments used widely in the health care industry to assess enrollees’ experiences and satisfaction with various aspects of their health care (see http://www.cahps.ahrq.gov). Other health system characteristics (plan type and county of residence) were obtained from the Florida Medicaid administrative files.
Using Stata (version 10), we used logistic regression to model the determinants of being aware of the EBR program, engaging in an approved behavioral activity, and redeeming a credit for an approved activity. 8 All variables were entered into the model regardless of their association with the dependent variable which was not assessed a priori. We calculated the Hosmer–Lemeshow goodness-of-fit test for all models. 9 P values for model fit, respectively, were .36, .17, and .58 suggesting no evidence of lack of fit.
Results
The majority of beneficiaries spoke English at home, were not Hispanic, were high school graduates, were parents reporting on behalf of their children, and had a personal doctor (Table 2). More than half were Black/African American. Between 12% and 15% reported being in fair or poor health and between 13% and 19% had no physician visits during the past year. Less than 60% were in a Health Maintenance Organization plan for at least 6 months, whereas roughly 14% switched plans. Finally, approximately half of the beneficiaries lived in Broward County.
Characteristics of the Analytic Samples, 2009.
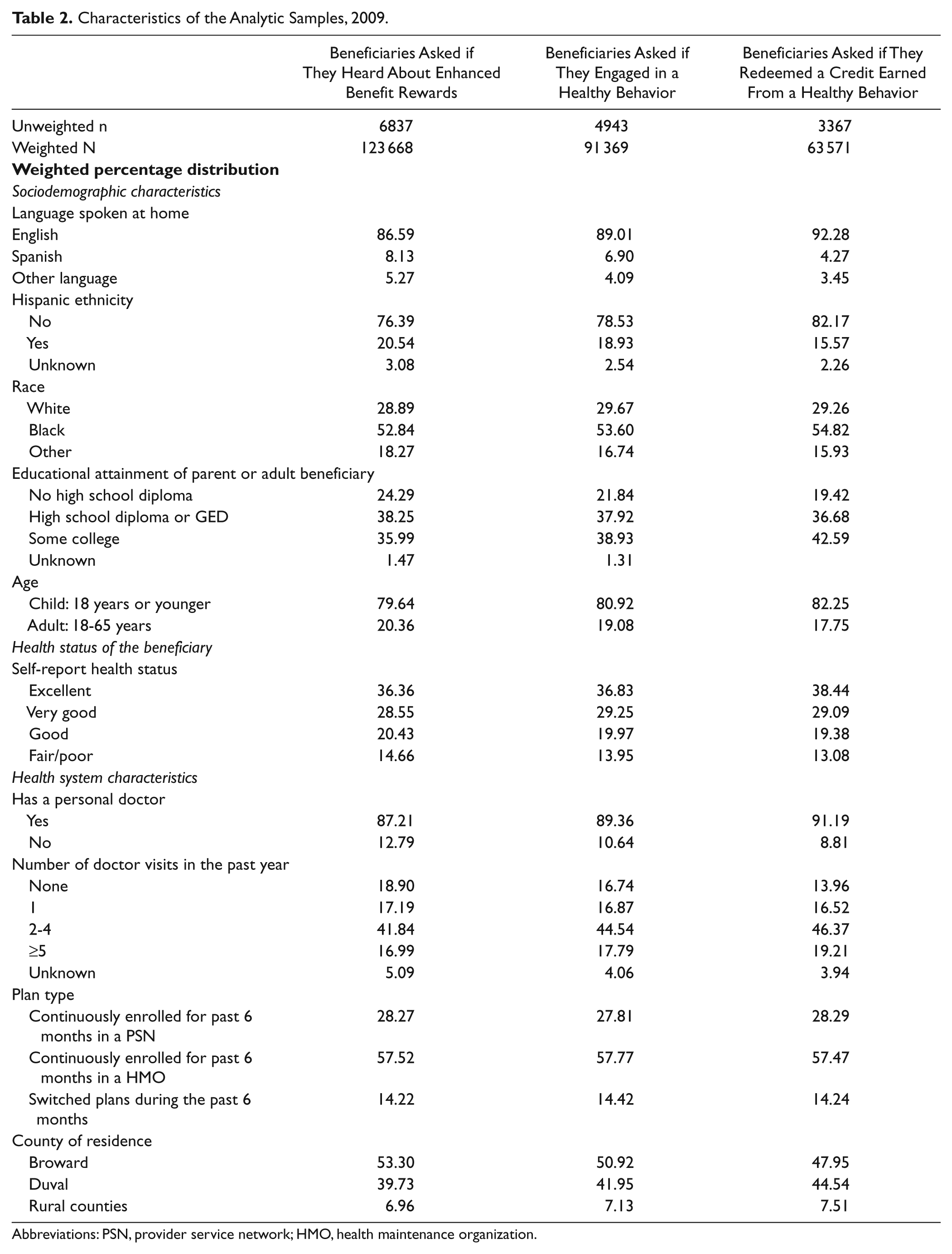
Abbreviations: PSN, provider service network; HMO, health maintenance organization.
Approximately 77% of beneficiaries reported being aware of the EBR program. Of those who were aware, 71% reported that they had engaged in an approved activity and 72% of those who engaged reported redeeming their credits.
After controlling for other variables, language, race, educational attainment, age of beneficiary, having a personal doctor, number of physician visits, switching health plans, and county of residence, were found to be statistically significant predictors of program awareness (Table 3). Being a non-English speaker, non-white, and having less educational attainment was associated with reduced likelihood of program awareness. Adult beneficiaries were less likely to report awareness compared with parents of child beneficiaries. Beneficiaries without a personal doctor and those reporting one or no physician visits during the past year were less likely to report being aware of the EBR program. Finally, individuals who switched health plans during the past 6 months and those residing in Duval County had increased likelihood of program awareness.
Logistic Regression: Determinants of Enhanced Benefit Rewards (EBR) Program Awareness, Participation in Approved Behavior, and Spending Earned Credits. a
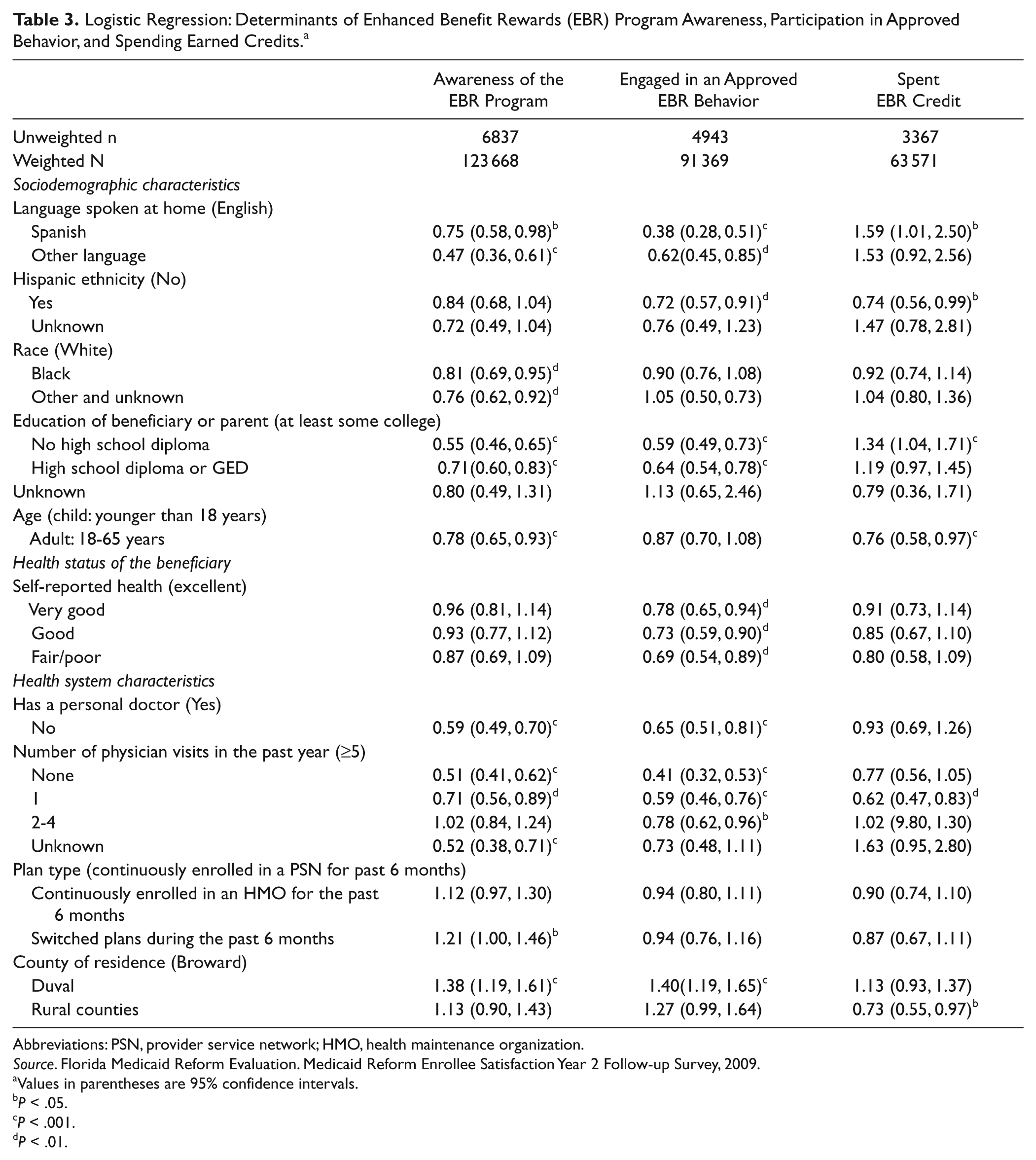
Abbreviations: PSN, provider service network; HMO, health maintenance organization.
Source. Florida Medicaid Reform Evaluation. Medicaid Reform Enrollee Satisfaction Year 2 Follow-up Survey, 2009.
Values in parentheses are 95% confidence intervals.
P < .05.
P < .001.
P < .01.
Language, Hispanic ethnicity, educational attainment, having a personal doctor, the number of physician visits, and county of residence were associated with engaging in an approved EBR behavior. Non-English speakers had reduced odds of engaging in a behavior, as did those of Hispanic ethnicity. Less educational attainment was also associated with lower odds of engaging in an approved behavior. Self-reported health status was a predictor of engaging in a behavior, and those in poorer health were less likely than those with excellent health to engage in an approved behavior. Individuals without a personal physician and those with few or no physician visits in the past year were less likely to engage in approved behaviors. Duval County beneficiaries were more likely to report engaging in approved behaviors.
Unlike EBR program awareness and engaging in an approved behavior, individuals who spoke a language other than English had higher odds of spending an EBR credit. However, individuals who were Hispanic were less likely to spend their credit compared with non-Hispanic beneficiaries. Adult Medicaid beneficiaries were less likely to report spending earned credits than parents of child beneficiaries. Individuals with one doctor visit were less likely to report credit spending compared with those with 5 or more visits.
Discussion
Since health behavior incentive programs are relatively new to Medicaid, the empirical evidence of their success or failure is relatively limited and results so far are mixed. Idaho’s wellness incentive program, for example, resulted in an increase in well-child visits for children enrolled in the Children’s Health Insurance Program. However, the rate of increase was greater for children who needed only one well-child visit compared with those needing multiple visits, and for Latino children compared with those of other ethnicities and races. 10 Furthermore, early examinations of Florida’s and Idaho’s experience highlighted difficulties in educating beneficiaries about incentive programs as well as the barriers recipients face in engaging in health behaviors. 5
The study described here provides examples of the ways in which sociodemographic characteristics, health status, and health system characteristics influence Medicaid beneficiary participation and engagement in an incentive program. Although data suggest that Florida Medicaid’s incentive program is maturing and program participation has increased, beneficiaries are not equally likely to participate and consequently benefit from EBR.
Perhaps most critical is the fact that knowledge or awareness of the program varies across groups of beneficiaries. As we suspected, non-English speakers, those with less education, and those without a personal physician and few physician encounters were less likely to be aware of the EBR program. County of residence was also a significant predictor of awareness of the EBR program. Similar trends were reported when respondents were asked if they participated in approved behaviors. Those who reported being in fair/poor health were less likely to engage in an approved activity, despite the fact that their health could most likely benefit from such engagement.
Although there were specific targeted efforts in Florida to reach out to Spanish and Haitian-Creole speaking communities, lower rates of awareness and participation among non-English speakers relative to English-speaking beneficiaries was still observed. The outreach used in Florida was extensive. For example, a public relations firm that specializes in outreach to immigrant communities was engaged to place advertisements in Spanish and Creole language newspapers and radio stations and to work with community leaders in publicizing the program. Furthermore, when an enrollee selected a health plan, telephone counselors who spoke in Spanish or Haitian-Creole were available to explain the EBR program to beneficiaries who spoke those languages. In addition, on enrollment in a plan, beneficiaries received welcome packets introducing the EBR program; and if a beneficiary earned a credit, periodic statements were mailed with an up-to-date account balance. Finally, Florida Medicaid included inserts promoting specific products available for purchase using the credits.11,12
When implementing an incentive program to encourage healthy behavior, organizers must consider these and other strategies such as community and health plan engagement to ensure participation by non-English-speaking persons. In addition, paying attention to the nuances of different geographical areas will ensure that all residents have an equal chance of program participation. For example, community groups, local pharmacies, and social service agencies could be used to provide additional dissemination conduits and also be involved in the overall design of the program, perhaps tailoring the intervention to specific populations and locations within a state.
Having a physician with whom one regularly interacts was key to knowledge and engagement in the EBR program. This finding underscores the need for provider education and participation in any health-related incentive program. Often, physicians and other providers are the main conduits of health information for their patients, and therefore play a vital role in the marketing of such incentive programs. Prior qualitative research on Medicaid beneficiaries indicated that they look to their physicians for information about their health. 4 Informing physicians, obtaining their support, and providing them with information to educate their patients are important steps to ensure beneficiary participation. Ideally, engaging physicians in the design of such programs can facilitate communication about such programs and enhance beneficiary participation.
It is important to note that a majority of EBR credits have been awarded for physician visits, childhood preventive care, and prescription drug compliance, all of which require encounters with a doctor. Very few credits have been earned for wellness activities such as smoking cessation or weight loss programs.3,11,12 The strong linkages between provider connections and EBR awareness and participation might be partially explained by the degree to which credits have been earned for physician office visits. Additionally, as shown in a recent literature review in contexts other than Medicaid showed that incentives appeared to work well when there were clearly defined behavioral goals that were simple to achieve (eg immunizations). By contrast, when behavioral goals were more complex (eg, weight loss) the incentives were less effective and long-term results not sustainable. 13
Turning to the question of whether a beneficiary who engaged in an approved EBR behavior actually spent the credit, our analysis revealed 2 positive predictors: being a Spanish speaker and not having a high school diploma. Although this finding is contrary to our expectations, it could be that these beneficiaries are those who are in most need of additional resources and therefore have a stronger motivation to redeem the credit. Adults were less likely than parents of children to redeem a credit. This is not surprising given that the administrative data show that most of the credits are used to purchase diapers.11,12 Perhaps the prospect of obtaining credits was more of an incentive for parents because of the need to purchase diapers and other costly, but necessary, items for their children. Individuals in rural areas were less likely to have spent a credit. This could perhaps be because of greater access barriers to a redeeming pharmacy.
This study is limited by the fact that the data were self-reported and no clinical measures were used to assess the benefit of this program on beneficiary health. Administrative and clinical data can be used in the future to address issues of engagement, the types of behaviors reported by beneficiaries, and overall long-term impact on health. However, the focus of the study reported here is on beneficiary perceptions, which can only be obtained from survey data. Both kinds of data are useful in determining the overall impact of the incentive program on health behaviors and health care utilization.
Policy makers, health plans, health care providers, and communities continue to search for ways to motivate citizens to engage in healthy behaviors. However, obtaining the initial engagement in such a program can prove challenging as different groups are not equally likely to be aware of, participate in an approved activity, or redeem a credit. Working with physicians and community organizations to design specialized outreach programs for targeted groups would likely lead to increased participation across all beneficiaries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Florida Agency for Health Care Administration.