
Abstract
Background:
Hispanics/Latinos (H/L) are the largest minority group in rural areas in the United States. Although childhood obesity represents a growing burden for this population, there is a lack of culturally relevant interventions designed for Latino children and their families.
Objective:
This study evaluates the relevance and acceptability of Hispanic Family Connections, a technology-delivered and family-based childhood obesity prevention program for Hispanic/Latino families in rural Nebraska. The program’s materials include a workbook with activities for home completion and interactive voice response (IVR) calls.
Methods:
A qualitative exploratory study was developed through Focus Groups. Participants were adults who self-identified as H/L, caregivers to children aged 6 to 12, and Spanish literate. A bilingual mediator used a script with 12 questions, based on the project’s conceptual and methodological frameworks: i-PARIHS, Cultural Relevance Questionnaire, and FRAME. We used PowerPoint presentations to share samples of the materials that comprise the Hispanic Family Connection intervention. Sessions were recorded, and we applied thematic content analysis with the support of a codebook based on the constructs of Innovation, Facilitation, Beneficiaries, and Adaptations.
Results:
Twenty-six H/L who lived in rural Nebraska participated in 8 Focus Groups (FG). We conducted 7 FG in Spanish and 1 in English. Participants highlighted the program’s delivery mode using automated personalized technology, which could give them more freedom to engage. They considered the images and wording culturally relevant and easy to understand. Also, the involvement of all family members was a positive note, with parents working as role models. Factors such as workload and weather conditions could act as barriers to participation.
Conclusion:
Overall, the intervention was considered relevant among rural Hispanic/Latinos, and the program design and materials were accepted with few adaptations suggested.
Introduction
Childhood obesity is a growing public health concern globally. 1 In the United States, 20.7% of children aged 6 to 11 are obese. 2 Significant disparities are seen between rural and urban areas, where rural children have 30% greater odds of being overweight and obese.3,4 Disparities in childhood obesity rates are also seen among minority groups. In 2020, obesity prevalence was highest in Hispanic children (26.2%) and non-Hispanic Black children (24.8%) compared to non-Hispanic white children (16.6%). 2 Hispanics/Latinos represent the largest minority group in the United States, making up 19.1% of the total population and the largest minority group in rural areas. 5 Yet, there is a lack of literature on childhood obesity prevention programs that are culturally relevant, family-centered interventions specifically designed for Latino children and their families. 6
Current childhood obesity interventions have shown positive results. Lifestyle interventions have a positive effect on weight loss compared with a control group (no-treatment group) or usual care (after the intervention and up to 1 year). 7 Other interventions involving parents8 -10 emphasize long-term changes focusing on health education activities with the family’s ability and autonomy to manage children’s weight change. 11 Another successful childhood obesity prevention strategy includes the use of technology-assisted interventions.10,12 Technology-assisted interventions in childhood obesity prevention interventions can be seen through gamification or exergames, 13 mobile applications, machine learning (ML)-based strategies, or a combination of these strategies and more. 14
However, childhood obesity prevention programs are not without flaws. Studies and first-hand experience of field practitioners have identified difficulties with the lack of motivation by parents, family income, access to health care and community resources, and the sociocultural environment as barriers to success in weight loss management.15,16 These barriers throughout all levels of the social-ecological model show the complexity of implementing a successful obesity prevention program within any community. Some limitations to remote interventions can be curbed by the implementation of in-person interactions, enhancing the use of technology. 17
The Latino population is not monolithic, and there are significant variations in health outcomes and social determinants of health risks based on language barriers, socioeconomic status, social support, and healthcare access. This highlights the need for targeted interventions and culturally sensitive approaches. Therefore, special attention must be given to the methodology of a childhood obesity prevention program for minority populations who may face unique challenges. Latinos are the largest minority group in the U.S. and Nebraska (19% and 12%, respectively),5,18 and Latinos are expected to represent 51.2% of rural Nebraska’s population by 2050. 19 Therefore, it is crucial to comprehend the needs of Latin families and their children about the relevance of technology-based intervention to obese childhood programs for Latin families living in rural areas. This study aims to evaluate the relevance and acceptability of Hispanic Family Connections, a technology-delivered and family-based childhood obesity prevention program for Hispanic/Latino families in rural Nebraska.
Methodology
Study Design
This qualitative exploratory study uses a Focus Group (FG) approach. FG is described in the literature as a form of group interviews, which highlights that this strategy in qualitative research is the interaction between participants as part of the method. In this method, a moderator asks questions about a particular topic that needs to be explored with a group of participants. The advantages of using focus groups are the possibility of including participants with a literacy restriction, and those who would not usually express their opinions out of fear or because they don’t find themselves important may feel encouraged by the group. In addition, the researcher can analyze the types of communication (including non-verbal) that arise in the group as the discussion progresses.20 -22
This study is part of the Hispanic Family Connections program, with the goal to culturally adapt and determine the feasibility of delivering family-based childhood obesity (FBCO) intervention content using interactive voice response (IVR) technology to Hispanic/Latino (H/L) families in rural Nebraska. The data reported in this article is part of phase 1 of aim one of the project’s data collection: “To culturally adapt and determine the relevance, acceptability, and usability of a culturally adapted technology-based FBCO intervention for H/L families in rural Nebraska.” Detailed information about the Hispanic Family Connections design and materials can be found in the protocol paper. 23
Participants and Setting
Recruitment was conducted in the participants’ preferred language (English or Spanish). Community Health Workers (CHW) led recruitment efforts by contacting their own health department’s client list to describe the details of the focus groups to potential participants and reviewing the informed consent document for those who agreed to participate. Participant eligibility were adults aged 19 or older who self-identify as Hispanic or Latino, who are caregivers to children aged 6–12 years, and must read and write in Spanish due to the nature of providing feedback on the Spanish materials for the program. The recruitment process and design of focus group modalities were developed through a collaborative process with Community Working Group (CWG) members. Figure 1 describes the different stages of the recruitment and implementation process, providing a summary of detailed planned actions to screen participants and ensure their comfort and presence during focus group meetings. More details about the CWG formation can be found in the Hispanic Family Connection’s protocol paper. 23

Collaborative plan for recruitment and FG implementation.
FG sessions were offered in-person, virtually through Zoom, or in a hybrid mode, where a Spanish-speaking moderator was present virtually, being able to see and hear participants who were all in-person at a local public site in the community. We collaborated with CHWs to identify preferred modalities among their communities. Therefore, FG participants only attended sessions hosted by their local health department. The preferred modality was virtual, through Zoom. When participants requested sessions where they could be together or when limited internet access was identified, in-person or hybrid modalities were adopted as suggested by CHWs (Table 1). CHWs assisted with scheduling based on participants’ preferred language and modality, and the research team obliged the requested meeting times. We used the strategy of virtual focus groups hosted via Zoom® platform due to the COVID-19 pandemic and the sanitary restrictions that were outlined in this historical moment, and because virtual FG have proven to be a promising strategy to ensure continuity of post-pandemic research.24,25 The hybrid modality was a suggestion from the CWG to try alternatives that fit their needs and resources. Language barrier is a major obstacle to the recruitment and participation of H/Ls; therefore, having a trained moderator who is a native Spanish speaker was deemed a priority for the research team.26,27
Summary of Focus Group Sessions Designed for Different Modalities.
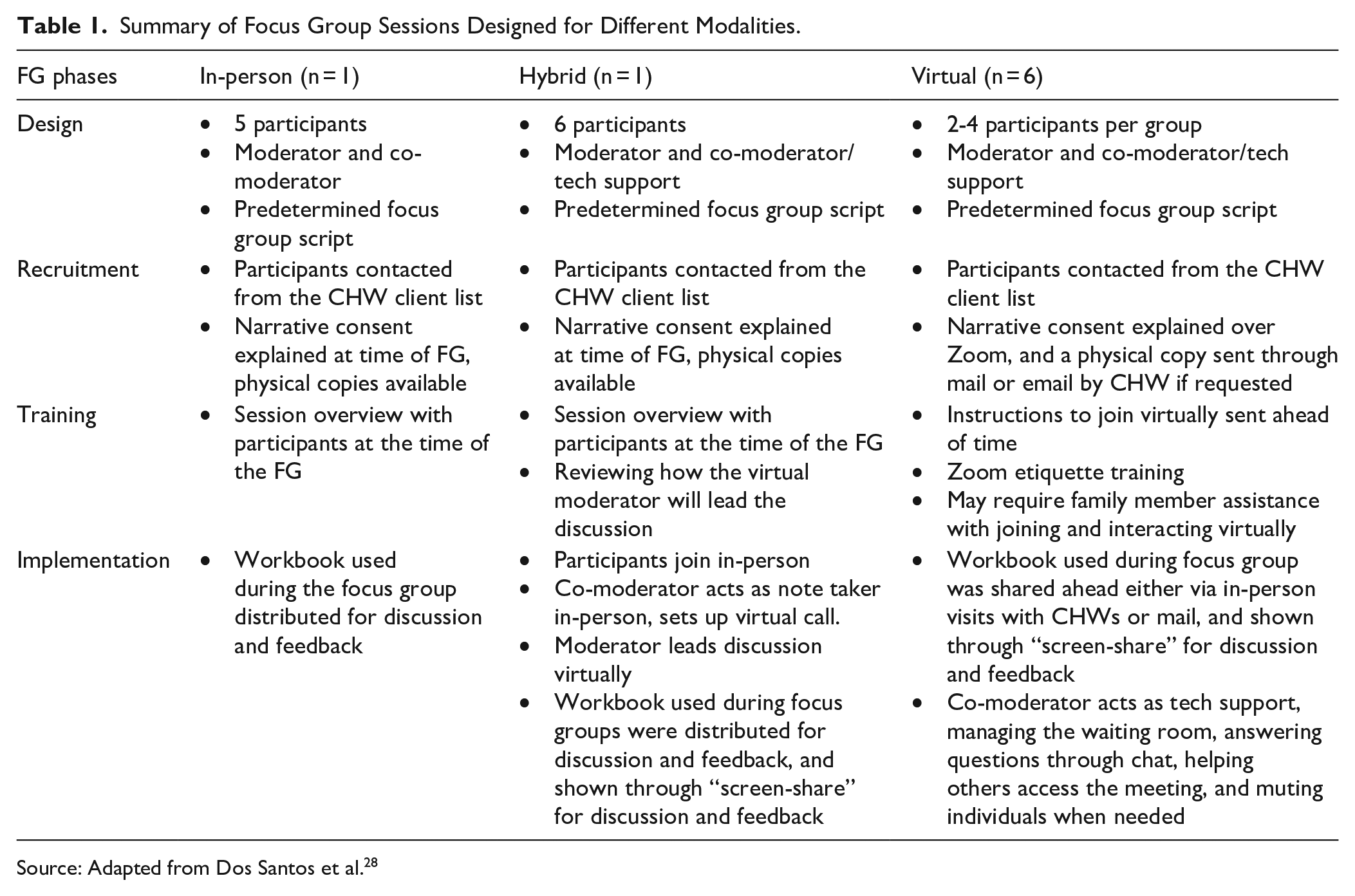
Source: Adapted from Dos Santos et al. 28
Based on the participant’s preferred language– English or Spanish, the research team developed data collection materials, in addition to documents (cited in Figure 1) aimed to assist participants on how to join Zoom meetings, introduce them to virtual etiquette, and describe what to expect during each FG meeting, according to their needs in each FG section. Although FG sessions were conducted in both languages, participants were required to be able to read and write in Spanish due to the nature of providing feedback on the Spanish materials for the program, as described in the inclusion criteria.
Data Collection
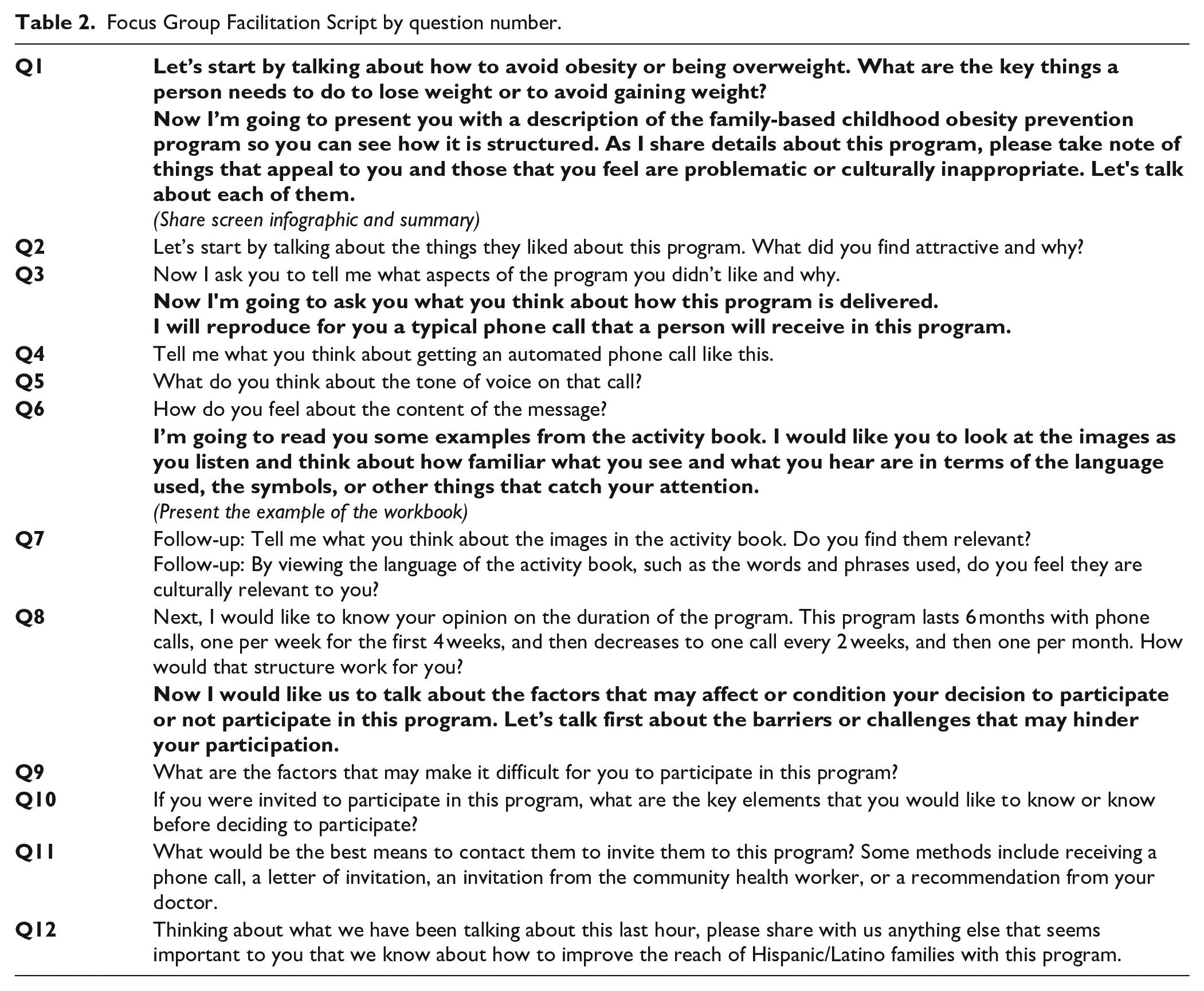
We conducted focus groups from July to October 2021. The research team had 2 staff members present during each of the Zoom® FG, one for mediation/facilitation and one responsible for notetaking and tech support. Both staff members had previous experience in conducting qualitative data collection and were not known to the participants prior to this study. During the FG, the bilingual facilitator presented the project and read the narrative consent; those who agreed to participate remained in the Zoom® section. We used a script with 12 questions (Table 2) based on the project’s conceptual and methodological frameworks – Integrated Promoting Action on Research Implementation in Health Services (i-PARIHS) 29 , combined with the Cultural Relevance Questionnaire (CRQ) 30 and the FRAME framework.29,31,32 We also used the PowerPoint presentation and Zoom® resources to share samples of the workbook and record samples of the IVR to evaluate the material’s relevance and acceptability. All the FG sections were recorded using the Zoom® platform for further transcription and data analysis.
Focus Group Facilitation Script by question number.
Data Analysis
For data treatment, we applied thematic content analysis in 3 stages (pre-analysis, material exploration, and treatment of results) 33 with the support of a codebook developed by the research team. Based on the project’s conceptual and methodological frameworks – i- PARIHS, CRQ and FRAME—we analyzed comments on the program considering the constructs of Innovation (program structure), Facilitation (resources/materials, including functional, conceptual, and linguistic relevance), Beneficiaries (target population), and Adaptations (form or modification, including cultural adaptations). During pre-analysis, we organized the transcriptions and field notes using NVivo® software and revised our objectives, and material exploration and treatment of results consisted, respectively, of coding, grouping, and looking for correlations (Figure 2).

Data analysis process.
The FG transcriptions were coded in their original languages (English or Spanish) using NVivo® software by 2 bilingual team members who are experts in qualitative research. The team members responsible for coding are Doctors of Philosophy with extensive backgrounds in qualitative data analysis using the support of software such as NVivo®. The resulting descriptive categories were compiled in English and Spanish and compared across languages until agreement was reached, evaluating intercoder reliability using Cohen’s kappa (>0.80). Translation of participants was done by one of the English-Spanish bilingual staff who was present during data collection and is familiar with the cultural context, and edits were made to achieve conceptual equivalence of the quotes’ meaning across both languages, and not a word-by-word direct translation.34,35 The transcriptions in their original language are available for consultation with the research team under reasonable request. We maintained participant anonymity by using ID numbers during the transcriptions and data analysis process. The main results per category are presented using participants’ excerpts.
Results
We conducted 8 FG with 26 participants in 4 rural health departments. Seven FG were conducted in Spanish and one in English. The only session conducted in English was through a virtual modality. The most common modality was virtual through Zoom (n = 6) with 15 participants; 1 FG was conducted as a hybrid where 6 participants were together in-person at a community site while the mediator connected through Zoom; one was conducted in-person where 5 participants and the mediator were together in a community site.
Community Health Workers from all 4 health departments invited 40 clients to participate in the FG, and of those, 26 attended the meetings. Most participants were female (96.15%), with a mean age of 39.2 years and a mean number of children of 3.6. Guatemala and Mexico stand out (30.77% each) regarding the country of birth, followed by the USA (15.38%). Regarding technology resources, 92.31% have reliable internet access, 69.23% use Smartphones, and 50% use the IOS/Apple operating system. The carrier most prevalent among the population was Walmart (19.23%), followed by Straight Talk and Verizon (15.38% each; Table 3).
Participants’ Characteristics by FG Modality.
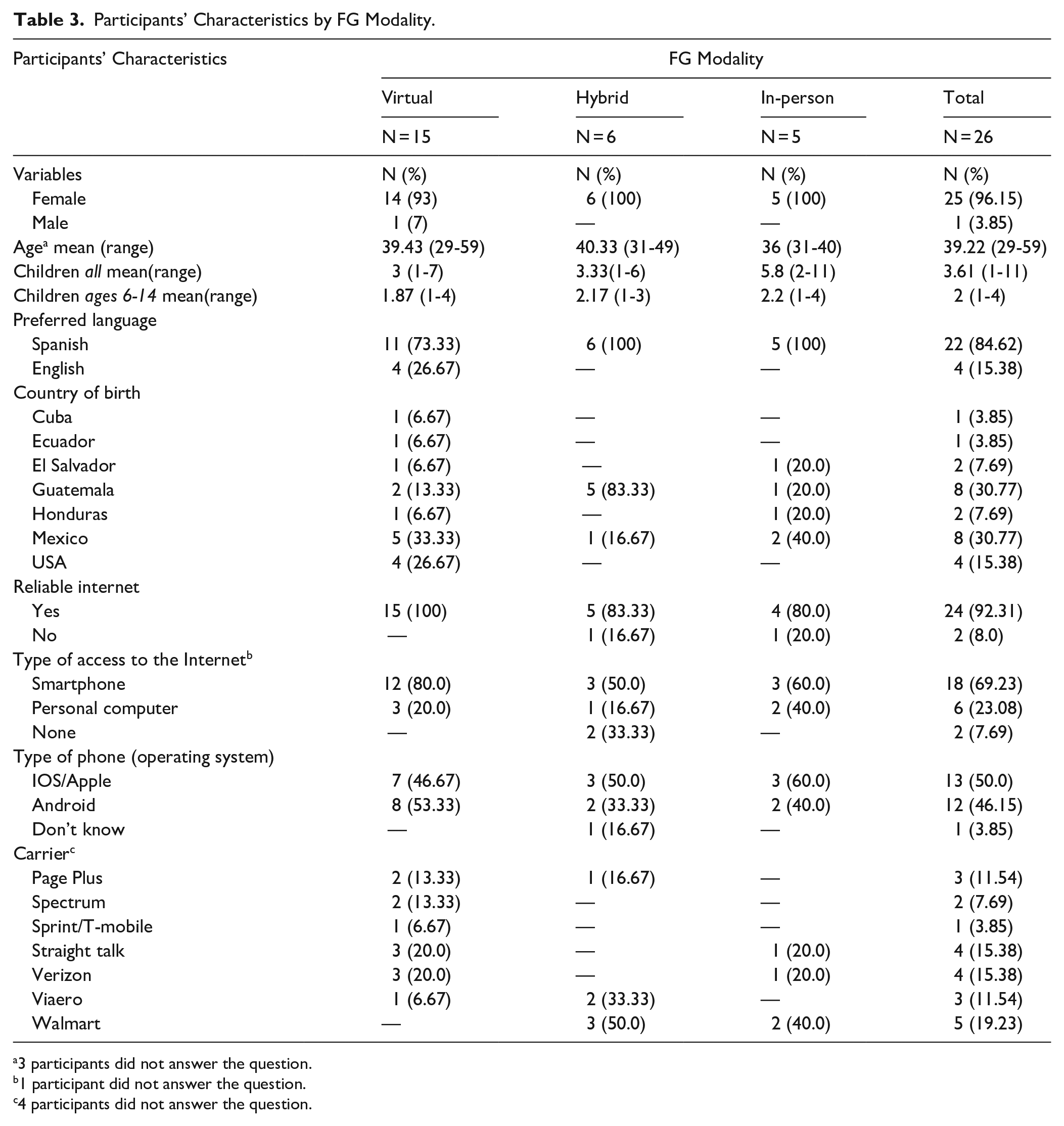
3 participants did not answer the question.
1 participant did not answer the question.
4 participants did not answer the question.
To evaluate the projects’ relevance and acceptability, we explored the participants’ previous knowledge about obesity prevention and categorized the FG results using the main constructs related to our conceptual and methodological frameworks—Innovation, Facilitation, Beneficiaries, and Adaptations—to facilitate translation to practice.
General Perceptions About the Topic
When questioned on how to avoid being overweight or obese, participants seemed to have a consensus about the main factors that influence these conditions, mostly being related to food and exercise habits:
Ah, I think that to avoid being overweight one should know which foods one should not consume or consume in very small quantities. And on the other hand, also how to do some exercises because that also helps not gain too much weight, right? And also drink a lot of water. (Virtual FG 7, Participant 1) What I understand is to avoid sugar plus carbohydrates. . . Too much sugar in the blood can lead to increased weight, it makes you obese and also leads to diseases like diabetes. (Virtual FG 1, Participant 2) Exercising. Eating salads and vegetables. (Virtual FG 2, Participant 4)
However, some participants highlighted the challenges posed by socioeconomic and cultural factors over their behavior and relationship with food:
Has been born and raised in a Hispanic family you have to eat everything with tortillas, or they make everything with like, you know, fatty stuff like ‘aceite’ (oil). Lord, then in my family, my mom always said, ‘eat the tortilla’, you know, so we can get full because she had a lot of us. (Virtual FG 3, Participant 3) I totally agree [. . .] because that was the way that I was brought up also in my in our household, too, it was, you know, five kids. And they also taught us to get tortillas, you know, with your food. So, you’ll get filled up faster and it’s hard to break that habit. [. . .] Everything’s expensive. The cheaper stuff are the fatty foods. . . I mean, the healthy food is more expensive than the fat. (Virtual FG 3, Participant 2)
Innovation
Regarding the proposed innovation characteristics, participants commented on the program structure, including the format, duration, and number of calls. Overall, participants seemed satisfied with the program being delivered using automated personalized technology, giving them the freedom to participate:
If it’s online. . . well, perfect, I’ll join the program. But, if it is something that I have to go to a place and I am going to be very far away, then it is going to be very difficult for me.” (Virtual FG 7, Participant 2) “I like the part that says it’s going to be something automated and personalized. From what I understand about that part, is that personalized means that they are going to treat it as the direct problem, since we are not all the same. (Virtual FG 7, Participant 1)
The idea of having an intervention that involves all family members and helps parents to be role models for their children was also considered a positive side of the program:
What I found appealing about it is that it basically guides you on how to become a better parent or caregiver for your children. And it helps to maintain a better lifestyle for yourself and for your family, you know. . . because with our busy lives, we sometimes forget how to care for ourselves or our children, for that matter. (Virtual FG 3, Participant 2) I feel like with the program, I feel like you kind of have an advocate for the parents’ side because as parents we advocate for our kids all the time, but sometimes we need that person to be right now. (Virtual FG 3, Participant 3)
Considering the program duration and number of calls, most participants expressed the understanding that changing habits can take time and, therefore, seemed to agree with the 6-month intervention and follow-up timeline:
I like it. I think it’s pretty good. So that way it gives us time to work on our workbook in our daily lives with the kiddos and ourselves. And the goal, the main goal, is weight loss for family and the kids.” (Virtual FG 3, Participant 3) At first, I was surprised because it seemed very long, but based on facts, it takes a long time to change a habit. [. . .] Because if we do [change a habit], maybe it will be short term, we will give up very quickly while we do other things. So. . . let’s go step by step. (Virtual FG 2, Participant 3)
Facilitation
Participants evaluated the project materials—IVR calls and workbook chapters – for linguistic, functional, and conceptual relevance. Regarding the calls, they liked that the content involved a reminder about their family goals and tips on how to achieve them. Also, they thought the calls were objective, and the Spanish dialect used was easy to understand:
I heard the call right now, everything is reminding me how to eat, how to drink. So, for me it is very important, [because]maybe we forget. So, when [the IVR system] talks to us, [it] ask us how many times we have eaten fruit or vegetables or something like that?. . . I think it is very important for me and my family. (Virtual FG 7, Participant 4) It was clear, short and precise. It was not something very long or boring, it was direct. (Virtual FG 7, Participant 1) It’s common [language], I think it’s the standard, there’s no problem with that. (Virtual FG 2, Participant 3) Well, [the IVR voice] speaks Spanish, they make themselves understood well and I have no problem, eh? It looks fine to me. It says things clearly that are able to be understood. (Virtual FG 7, Participant 3)
Although a few participants would have liked to have access to more parts of the book before giving their opinion, most of them highlighted the importance and desire to use this resource as an opportunity to take some time to work toward a goal as a family. The images, language, and exercises would help create this habit:
Well, what caught my attention was that it says that the whole family has to get involved. . . We have to do it together so that everything works well. (Virtual FG 4, Participant 3) The graphics help us a lot. Images are always going to be more attractive to children than a book without pictures, right? And it’s very good that you read it and then see it, because for example, if we want to share this story with our children, they can participate while we learn, right? (Virtual FG 2, Participant 3) And also that we have to keep writing down everything we are progressing in the process, such as the hours we are reducing the children screen time. Like the activities and everything is being written down to see what is going, what is improving or what we are not doing well. (Virtual FG 4, Participant 1)
Beneficiaries
We explored some possible barriers that could keep participants from joining the intervention. Factors related to a busy lifestyle, long work hours, and the weather conditions were the most cited:
I work. Sometimes I get tired, and I don’t want to exercise because I say let’s work, make food and exercise. (Virtual FG 2, Participant 1) The problem is that I work and sometimes I don’t have time to receive calls. (Virtual FG 8, Participant 1) Later on as the winter gets very harsh, well, we can’t go outside, but for those that have [a treadmill or a place to walk indoors]. (Virtual FG 2, Participant 3) One factor could be the weather. We here in Nebraska are in very extreme weather. So it may be that when the seasons change, we make a new habit. For example, right now, [we are able to] go for a walk, etc. So, when the weather changes, we have to rethink the activities [we do] and even the foods, because when it’s cold we want breads, chocolate and things like that. (Virtual FG 2, Participant 3)
When talking about how they would like to be invited to participate in a program like this or how they think other members of the community would prefer, participants made it clear that rather than being contacted directly by the research team, the invitation should come through someone the families trust, such as a doctor or community health worker, or through the school:
Well, if we receive an invitation by mail from someone we don’t know, or where they came from, then you wonder ‘how did they find me? How does he know my [child] needs [this program]?’ But if it is through the doctor, I prefer that way . . . I believe that it was the best option. (Virtual FG 7, Participant 1) Right now, we already know that you found us through the doctor. Now if you want to address/talk to us, address us directly . . . If I receive a letter directly from you, I already know who it comes from. I already know that I was referred by my doctor. So now I will know more about you through the letter. (Virtual FG 7, Participant 2) [Another idea would be] integrating the school into sending brochures to parents because many children do not go to the clinic, they go to other places. So, the school gives out brochures so that more parents realize that this program exists. (Virtual FG 4, Participant 1)
Adaptations
Related to content, the participants asked for more specific and personalized information regarding what time to eat and exercise, and resources available in the community that could help them fulfill their goals:
I would think that they could also include [questions on] how many hours a day you are doing sports, how many meals a day, do you do outdoor exercises or things like that with your parents. But if it’s about food, how many meals a day do you want. (Virtual FG 1, Participant 3) That [the workbook] has, for example, a set time for their breakfast and what to do after breakfast. I don’t know, going out to do exercises, going out to play soccer for a little while, setting time for everything. (Virtual FG 1, Participant 2) See if a schedule of some activities could be attached. For example, in a certain school they lend it to the gym or places that have physical activities for children. Because many mothers have [their children] in activities, but some others say ‘oh, I don’t have to pay for them to do this activity’. Because outside of these months when the weather is good, you can’t take the children out to do activities. So, it would be good to implement some type of activities that we could bring the children throughout the program? (Virtual FG 2, Participant 1) I want to have, you know . . . make like my calendar so they can go ahead and, you know, see that book with them, you know, like let’s read this together. Let’s do this on Monday. Let’s go play soccer on Tuesday. And if it rains, then we’ll just go up and down the steps like ten times. I don’t know. (Virtual FG 3, Participant 2)
Considering how the intervention is delivered, even though they praised the convenience of technology, participants would like to meet face-to-face with researchers/practitioners during or at the end of the intervention to track their progress:
. . .at the end of the 6 months I won’t see you again. So, I don’t know if I really progressed or stayed at the same level. I think [there should be] a personal interaction in the end to see how you progressed. (Virtual FG 1, Participant 3) So what I would recommend would be that at the end of those 6 months there was a personal interaction like at the beginning. (Virtual FG 1, Participant 2)
To increase reach and participation, they suggested the use of social media and highlighted the importance of communication among Latino families, so everyone knows that there’s a program made especially for this target population:
I think it’s important to spread the word about this program. I don’t know, maybe Facebook, maybe even TikTok. I don’t know what platforms you guys are on . . . Instagram, possibly, I don’t know. Share with your friends. Share. Share the wealth in health tech. Just encourage each other. I mean, that’s what it’s all about. [. . .] it is very important for Hispanic family word of mouth, because we all have lots of cookouts and we’re always up to the words and, you know, all humans. (Virtual FG 3, Participant 3) People use social media a lot now so I think that [using it] would be good. Good method to let people know that there is someone who is willing to help us. Because the truth is that I didn’t know about that program if it existed, so now that we know more or less so that all of us Latinos who need help, know that there are people who want to help. (Virtual FG 7, Participant 4)
Discussion
Social determinants of health, as they manifest in rural areas, especially among predominantly Latino communities, create implementation challenges for diet and exercise programs and for people to engage in such programs.36,37 To create a more impactful and sustainable long-term intervention, it is crucial to include the voices of minority communities, who are often overlooked in research design. Devoting efforts to a focus group to evaluate the relevance and acceptability of an obesity prevention program by creating a personalized, remote program focusing on Latinos and their culture has the potential to mitigate barriers.
General Perceptions About the Topic
Whether one follows a strict diet or not, most people can describe what constitutes healthy habits to prevent weight gain and develop chronic diseases such as diabetes. The participants in this study are aware of the importance of eating a well-balanced diet, including exercise in their daily routines, and drinking water. They also echoed realities faced by many, highlighting the challenges posed by socioeconomic and cultural factors in implementing their vision of wellbeing.
Dietary habits developed during childhood can play an important role in the tendency to recreate adverse diet practices, 38 and participants spoke of this topic as a unique challenge among Latinos. Examples of parental influence shared by participants emerged in the FG when they shared histories of how their mothers used to prepare foods with carbohydrates and fats for satiety and made sure they ate it all. Literature on how parental behaviors influence diets suggests that Latinos throughout the United States face a similar challenge. 39 This aligns with the findings from this research and highlights the importance of addressing the topic with this specific population to avoid a repeating cycle of overconsumption.
Economic realities play a large role as parents struggle to find time and resources to feed their families. 40 The cost of healthy food has been debated over time, mainly due to the differences in metrics and measures used.41 -43 While some studies suggest that the price of healthy foods is similar or cheaper to less-nutrient-dense foods, 44 others shift the focus of expense between short- and long-term costs, citing the high price tag of chronic diseases caused by poor diet and exercise as the true expense. 45 Although the actual cost of food in rural areas may vary, participants perceive healthier options as more expensive. This perception, combined with limited store options and resources, forces low-income families to prioritize immediate affordability in their dietary decisions.
Innovation
The necessity to reduce the gap between research and practice is not a new discussion, but there is an increasing debate about how technologies can help fill this gap in rural areas and for different health conditions.46 -49 Finding the right technology can increase the reach and access of rural communities facing different barriers to up-to-date and reliable health information.
In healthcare, innovation can be an idea, service, product, or new patient care practices that show clear benefits. 50 Thus, to be successful, innovation needs to be usable and desirable. 51 When we discussed the innovation characteristics with participants, they were excited about the possibility of using personalized technology that provided the freedom to participate remotely, which indicates the acceptability of its format.
One reason for this acceptance is the specificity of our study population. Over a third of Nebraska’s population lives in rural areas. 52 Unfortunately, rural communities experience some barriers to accessing health services, such as a lack of transportation, increasing healthcare costs, and the distance and location of services. 53 Therefore, being able to complete the program remotely could help increase participation and long-term involvement with the intervention and among family members.
Another aspect of the innovation that was well received by participants was that all family members were involved in making the changes, with a special focus on parenting skills and role modeling. Literature suggests that family-based interventions, including for children’s weight management, are used globally and with good results. 9
Facilitation
Not all Spanish is created equal, with an estimated 10 different dialects in Latin America. 54 Within this focus group, participants’ country of origin varies between 6 Latin American countries, most from Mexico (30.77%) and Guatemala (30.77%). In the workbook development phase, it was crucial to design the language and images in a manner that reflects the diversity of the Latino population the workbook serves. The recognition of the didactic material as something culturally accepted and translated into Spanish deemed acceptable by all, seems to be a key element that can facilitate the adoption of the program, along with flexible schedules, to facilitate family involvement, respecting their daily routines.
A challenge experienced during this focus group was that although the inclusion criteria required participants to be able to read and write in Spanish, we did not specify at what level. When developing or adapting materials for diverse audiences, careful consideration should be given to both readability levels and image selection to expand accessibility and improve program effectiveness. Compared to other minority groups in the US, Latinos have the lowest health literacy levels, 55 highlighting the importance of developing accessible and culturally relevant materials to implement equitable practices.
Beneficiaries
When developing any behavior change intervention, it is crucial to invest in understanding the context in which its participants live. Many theories and models56 -58 identify the relationship between one’s environment and its influence not only on behavior change, but program adoption. In this FG, participants spoke about the reality of working hard jobs with long hours and how it hinders their ability to implement healthy behaviors. Literature on similar population groups has shown that a lack of social safety nets, in addition to demanding work conditions, can play a role in deteriorating health.59 -61 Whereas rural areas experience a lack of resources, participants especially identified that a lack of spaces for physical activity is an added challenge to being physically active. This barrier in their built environment is especially debilitating during the long and harsh winter months.
Adaptations
Participants provided suggestions on adaptations to the intervention content and delivery, and how future recruitment and retention could be improved. Even though they liked the remote format of the intervention, as it provides flexibility and easy access, participants expressed their need to have in-person interactions with the research team, CHW, or each other at the end of the 6-month intervention to review their progress. Although technology-based interventions show to be effective and accepted by rural communities,46,62,63 there are still challenges to overcome. The use of technology-based interventions needs to consider the technology literacy level of the participants, their access to technological devices and internet connection, as well as the aspect of trust and connections that in-person interactions can help build between the research team and participants.64,65 Participants would like to have access to content that gives them specific directions on how to incorporate the new information and create new exercise and eating habits.
Structural and social contexts that create barriers for participants also create distrust and skepticism in participating in research.66,67 Participants identified how recruitment efforts should consider where information is being shared and by whom. Participants trusted information being shared from their children’s schools and valued referrals from their doctors and community health workers. This matches recent literature targeting immigrants in health research,68,69 and the need to cultivate trusted allies within the community.
For future project implementation, FG participants also suggest reaching the target population through their community settings and social media to increase recruitment and participation. Literature supports our FG findings, demonstrating that social media recruitment can represent not only a feasible but also a low-cost option for rural communities and that word-of-mouth remains an essential strategy alone or associated with other recruitment efforts.70,71
Study Limitations
Although FG was elected as an important method to comprehend the relevance and acceptability of the Hispanic Family Connections program to reach its sample target population, some changes were necessary in this study. The COVID-19 pandemic and the sanitary restrictions forced the research team to conduct the FG sessions in a synchronous virtual format, which may have caused a barrier due to difficulties in the use of technology among participants or may have inhibited sharing views openly due to the unfamiliar format. In addition, the hybrid and in-person FG conducted in August 2021 imposed different challenges to the research team: In both modalities, all participants were wearing masks due to sanitary requirements and placed in a public site selected by the CWG, which led to a decrease in the audio quality recorded noticed by the research team during the transcription process; participants also engaged less in discussion with their group when comparing to the engagement we observed during the FG conducted virtually, which may have been caused due to fear or uncertainty of socializing towards the end of the pandemic. Specifically for the hybrid modality, we faced technology limitations with internet access and challenges setting up the space to connect with the mediator via Zoom.
Study Strengths
However, this study has its strengths. The use of qualitative methods ensured a more detailed and in-depth analysis of participants’ perceptions of the program. Another point was to offer bilingual facilitators, allowing participants to express themselves in the language they felt more confident. Another strength was the availability of materials before the focus group day, allowing more time for participants to be more familiar with the FG content. The recruitment made by Community Health Workers (CHW) was another positive point because they chose participants with the same profile as the program’s target audience. Finally, this study investigates the relevance and acceptability of the Hispanic Family Connection program amongst H/Ls, which is crucial given that the program is exclusively designed for this social group, which holds the potential to reduce health disparities.
Conclusion
Overall, the technology-delivered childhood obesity intervention was considered relevant amongst Latinos, and the program design and materials were accepted, with few adaptations suggested. The importance of involving the whole family appears in multiple constructs, highlighting how the family is seen as a unit and requires a multifaceted approach to engage individual family members in behavior change. Also, participants showed satisfaction with the program being delivered using automated personalized technology, giving them the freedom to participate at their convenience, without the burden of excessive workload, costs, and transportation acting as barriers.
Footnotes
Acknowledgements
The authors and research team would like to express their sincere gratitude to the Community Health Workers and local health department administrators who assisted with the recruitment, facilitation, and relationship building with community members during the development of the Hispanic Family Connections program.
Ethical Considerations
This study was approved by the University of Nebraska Medical Center Institutional Review Board (# 0745-20-EP) and is available for consultation in ClinicalTrials.gov (Identifier: NCT04731506).
Author Contributions
FB, FA, CE, and TFA were involved in the study design and planning. TFA, NS, CS, and FM were involved in data collection and analysis. TFA and NS were responsible for final manuscript formatting with supervision from FB. All authors provided a critical review of the manuscript’s final version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health Center of Biomedical Research Excellence (COBRE) via Nebraska Center for the Prevention of Obesity Diseases through Dietary Molecules (NPOD) grant number P20GM104320.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The transcriptions in its original language are available for consultation with the research team under reasonable request.