
Abstract
Background:
Hypertension and obesity are major public health problems in the United States and Maryland.
Objectives:
To assess the impact of Medication Therapy Management (MTM) on controlling hypertension and obesity in a sample in Southern Maryland: Prince George’s, Calvert, Charles, and St. Mary’s counties.
Methods:
171 patients with high blood pressure were enrolled in an MTM program for 12 months. Patients received at least one pharmacist consultation between September 2021 and September 2023. We employed a pre-post prospective study design to assess the impact of MTM on patients’ blood pressure management. We examined the association between MTM and systolic blood pressure (SBP) and diastolic BP (DBP) as the primary outcome, and weight and body mass index (BMI) as secondary outcomes. We used descriptive analysis and fixed effect regression models to present the association between outcome variables and enrollment time in the program.
Results:
Our findings showed that the MTM reduced uncontrolled hypertension by 17.5 percentage points, weight by 3.6lbs (10.2), and BMI by 0.6 kg/m2 (2.1). The regression model showed that the MTM intervention reduced the prevalence of uncontrolled hypertension (−1.81, CI: [−3.11, −0.51]), and obesity (BMI > 30, −1.85 (CI: [−3.12, −0.57]), by 12 months of enrolling in the program. During this time SBP reduced to −10.37 mmHg (CI: [−19.62, 1.2]).
Conclusions:
Our results suggest that policymakers should prioritize promoting MTM services as an effective means of blood pressure control. Combining a community health worker (CHW) model with community-based pharmacists can further improve health outcomes for patients with hypertension.
Keywords
Background
Hypertension and obesity continue to pose significant public health challenges across the United States, 1 including Maryland, particularly among populations with limited access to quality healthcare. In response, Prince George’s County Health Department (PGCHD) leads the PreventionLink project, named PreventionLink by PGCHD in reference to the linking of preventative services and health care, has implemented strategies such as Medication Therapy Management (MTM) and the involvement of Community Health Workers (CHWs) to enhance care processes and improve health outcomes for patients with high blood pressure, heart disease, stroke, diabetes, and obesity in Maryland.
Awarded by the Centers for Disease Control and Prevention (CDC)’s Division of Diabetes Translation’s Innovative State and Local Public Health Strategies to Prevent and Manage Diabetes, Heart Disease, and Stroke in October of 2018, PreventionLink (DP18-1817) was a five-year cooperative agreement (2019-2023) with PGCHD, working to identify and improve the quality of life for residents at risk of or living with a chronic condition in underserved communities by providing easier access, and affordable solutions to good healthcare through a patient-centered approach, evidence-based programs, and technology. In addition to Medication Therapy Management (MTM), PGCHD’s PreventionLink provided other programs including Diabetes Self-Management Education Services (DSMES), Diabetes Prevention Programs (DPP), Cardiac Rehabilitation, and Remote Patient Monitoring (RPM).
By the end of 2023, PreventionLink formed data use agreements and bi-directional e-referral capacity with more than forty-six (46) health care systems and primary care practices serving more than 187 722 patients in the Prevention Link Service Area: Calvert, Charles, St. Mary’s, and Prince George’s Counties in Southern Maryland. PGCHD supported our 46 partners with internal central referral specialists, community health workers, and contracted practice transformation consultants to provide technical assistance and clinical decision support.
In the PreventionLink Service Area, the rates of hypertension are Calvert at 33.1%, Charles at 35.2%, Prince George’s at 34.3%, and St Mary’s at 36.0% (See Appendix 1). Additionally, the obesity rates in these counties are 34% in Calvert, 40% in Charles, 37% in Prince George’s, and 37% in St. Mary’s. 2 At the same time, Maryland ranks among the top 14 states with the highest cholesterol levels, standing at 37.6%. 3 PreventionLink uses a technology-based, patient-centered collaborative approach to improve healthcare outcomes, including multi-directional e-referral and mobile health technology (mobile app, blood pressure devices, tablets). 4
Medication Therapy Management (MTM), defined by the American Pharmacists Association as a service or group of services that optimize therapeutic outcomes for individual patients has emerged as a comprehensive, patient-centered approach to optimizing medication use and improving therapeutic outcomes. 5 MTM shows promise in managing chronic conditions such as hypertension and obesity, where medication regimens can be complex and adherence challenging. 6 MTM encompasses a range of activities including medication review, personal medication records, and intervention plans and can be implemented within different patient settings. MTM services, often community-based, have been rendered by various healthcare professionals and several studies have proven their effectiveness.7,8
Given their unique expertise in pharmacology, medication safety, and patient counseling, pharmacists have long played a pivotal role in successful implementation of MTM services for patients with chronic diseases. 5 Community pharmacist interventions positively influenced patients’ medication adherence, 9 and led to a significant reduction in systolic and diastolic blood pressure in hypertensive patients.10,11 These services indicate improved disease management in under-served populations. 12 These findings are further supported by a 2014 meta-analysis which found that blood pressure management improved more with pharmacist interventions compared to the usual care practices. 13
Primary care physicians (PCPs) are crucial in Medication Therapy Management (MTM), particularly for patients with multiple chronic diseases or complex medication needs. 14 They identify candidates for MTM, 15 assess patients’ full medication regimens, 16 and coordinate with pharmacists and other healthcare professionals to develop tailored medication action plans. 17 PCPs also educate patients, monitor their progress, 18 and ensure care continuity across various healthcare settings. 19 Overall, their involvement is vital for enhancing medication management, improving patient outcomes, and increasing care quality. Through these roles, and many other activities PCPs are crucial in ensuring effective medication management, improving patient outcomes, reducing healthcare costs, and enhancing the quality of care delivered.
Concurrently, the valuable role of Community Health Workers (CHWs) in the delivery of MTM services for chronic disease management, particularly among underserved populations, is recognized. 20 CHWs often share the cultural, linguistic, and socioeconomic background of populations they serve, have the trust of the community, and can help underserved populations navigate complex and fragmented healthcare systems. There is evidence that involvement of CHWs in medication management leads to improved blood pressure control and medication adherence, 21 and that interventions by CHWs are efficacious and cost-effective in the management of chronic health conditions particularly in underserved communities. 22 Integrating CHWs into healthcare teams has also been shown to help overcome participation and retention barriers in chronic disease management programs, as seen in Diabetes Prevention Programs (DPP), 23 and improve access and outcomes when attached to structured CHW-tailored management compared to those not attached. 24 While the sole impacts of pharmacist-led MTM and CHW interventions have independently been researched, the synergistic effect of the two is not well understood. Redressing this knowledge gap presents a significant opportunity for enhancing chronic disease management, particularly in underserved populations.
The consistent engagement between pharmacists and patients within the medication synchronization program provides many advantages. These include the early detection of errors, 25 enhanced adherence to medication regimens,26,27 improved oversight by pharmacists in managing medication-related issues effectively, and fewer missed doses. 28 This approach facilitates the coordination of care and enables the identification and mitigation of barriers associated with social determinants of health to better patient outcomes and overall healthcare quality. 29
The study has been approved by the Institutional Review Board (IRB) at the Johns Hopkins Bloomberg School of Public Health.
Objective
This study evaluates the impact of MTM by community pharmacists and primary care physicians to improve health outcomes for their patients with high blood pressure, weight and BMI in Maryland.
Methods
Study Design
The CDC-funded PreventionLink Program, led by the Prince George’s County Health Department, partnered with the University of Maryland P3 (Patients, Pharmacists, Partnerships) Program to recruit community pharmacists to implement MTM services for patients referred by their primary care providers. 23 The Prince George’s County Health Department created PreventionLink to facilitate participating primary care physicians and other health providers to connect their patients to support services in the community to prevent or better manage chronic conditions such as diabetes, obesity, and hypertension.
Under PreventionLink, 34 local medical practices used a bi-directional e-referral system to refer to their patients diagnosed with hypertension for MTM. These patients then received MTM services from pharmacists, who counseled and assisted them in improving their self-management of hypertension and cholesterol levels. P3 provided training, technical assistance, and tracking tools to equip community pharmacists to review and assess patients’ medical and medication histories; assess patients’ knowledge and behaviors, including adherence to medications, proper device use, smoking status, and acute care utilization; identify and solve potential and actual drug-related problems, and assist patients in setting and achieving short-term self-management goals. Pharmacists identified potential or actual medication-related problems and healthcare risks and recommended solutions to healthcare providers that can help mitigate those risks, with documentation provided to the primary care providers (see Diagram 1).

CHW driven POC workflow: MTM.
Implementation
The project partnered with 3 pharmacists from P3, 6 community pharmacies, and 16 referring physicians. The project used e-prescribing to monitor medication adherence, involving CHWs to assist patients with their devices. An e-prescribing company (DrFirst) helped monitor medication adherence across multiple pharmacies by collecting refill data. REDCap captured pharmacist information and referrals. CHWs were trained to support patients with biometric devices for medication therapy management, delivering virtual and in-person aid (see Diagram 1).
CHWs activities included but were not limited to patient enrollment and SDoH assessment involving multiple steps (obtaining schedule and patient eligibility details, providing consent forms and informational materials, completing MTM forms, confirming eligibility with lab data, entering referrals in Chesapeake Regional Information Exchange for our Patients (CRISP), and uploading SDoH assessments) and connecting patients with the P3 team during virtual online meetings. See Appendix 2 for more details.
Study Population
Using the Cochran formula with α = 0.05 (95% CI and β = 0.8 (power), probability of having hypertension of 35%, and with considering 20% missing, and 12% reduction, the P3 team recruited 226 patients between September 29, 2021, and September 29, 2023. From these 226 patients, 55 patients didn’t participate, and 171 patients were engaged in the program and received interventions.
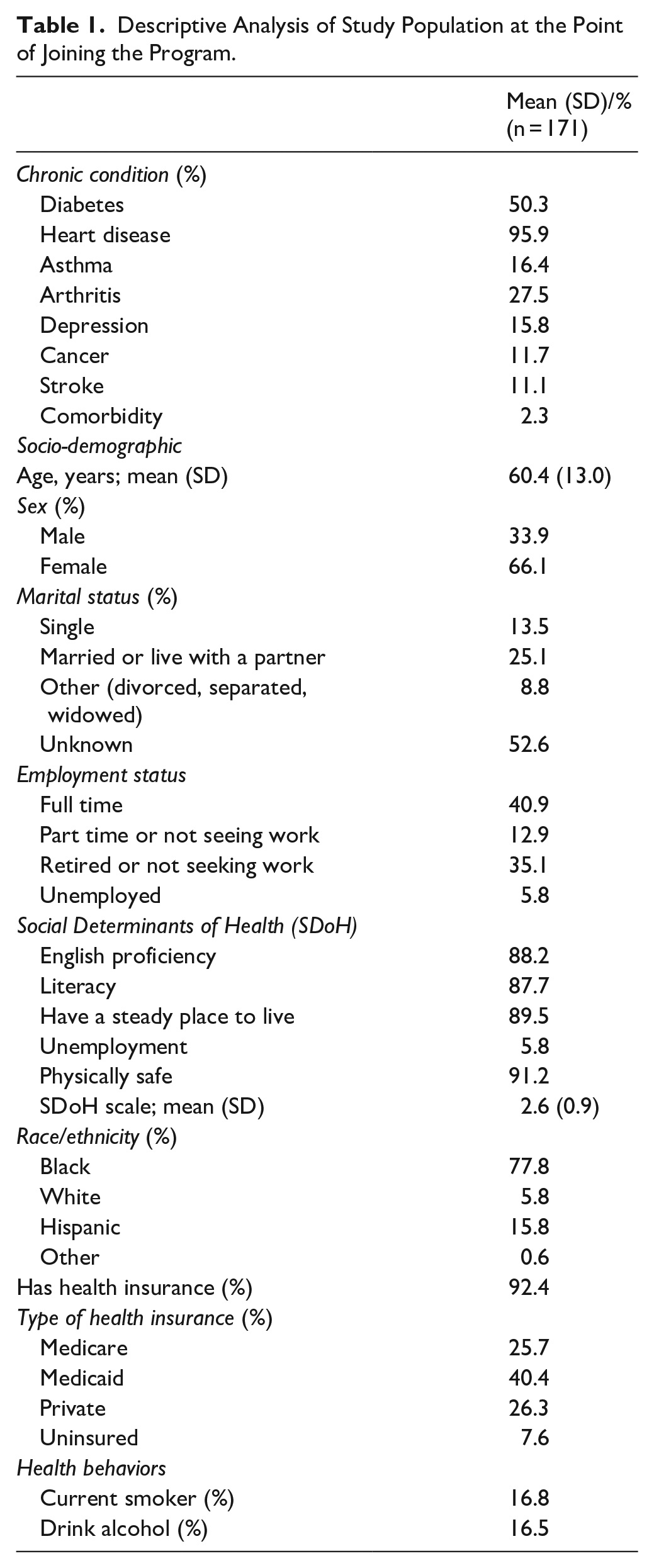
Patients meeting the following study criteria were included: (1) The participant must meet one of the following criteria for hypertension: uncontrolled hypertension with blood pressure over 130/80, diagnosed with hypertension at their last primary care provider (PCP) visit, issues with medication adherence (such as adverse reactions to specific medications or the need for dosage adjustments), use of two or more medications for hypertension, more than six medications for chronic diseases and conditions, or a primary or secondary diagnosis of uncontrolled hypertension during hospitalization. (2) Participant who met the social determinants of health criteria. We included participants who met one or more of the following criteria: proficiency in English, literacy, having a stable place of residence, unemployment, and being physically safe. We summed these elements to create a social determinants scale, which ranged from 1 to 5 (see Table 1).
Descriptive Analysis of Study Population at the Point of Joining the Program.
Data Sources
Patient clinical outcomes were systolic blood pressure (SBP) and diastolic blood pressure (DBP), body mass index (BMI) and weight. PreventionLink had Data Use Agreements with partner practices/providers to have access to Electronic Medical Records, so this electronic health information (including demographic information, medication history, chronic disease history, blood pressure readings, lipid panel, and social history, for example, alcohol drinking, and smoking status) was securely shared with the study team, also included as part of the referral, and shared with the study’s Pharmacy Partners, University of Maryland P3.
We collected this information at baseline, 6 months after intervention and 12 months after intervention. The control variable are patients’ demographic variables (age, sex, marital status, and race), number of chronic diseases, health insurance status, smoking and drinking behaviors.
Statistical Methods
We employed a pre-post prospective study design to assess the impact of MTM on patients’ blood pressure, weight and BMI. We analyzed the data using bivariate and multivariate statistical techniques. The bivariate analysis compared the semi-annual change in the blood pressure systolic and diastolic; weight, and BMI from the baseline to the corresponding evaluation year, using the patients EMR records. T-tests determined whether patient outcomes changed before enrolling in the program and after joining and staying an average of 12 months under the provider monitoring system. We ran a logistic regression using patients with hypertension (SBP ≥ 130 mmHg and DBP ≥ 80 mmHg), and obesity (BMI ≥ 30 kg/m2) after joining the program. Additionally, we performed a fixed effect model to determine the association between changes in SBP, DBP, weight, and BMI and time of being enrolled in the program (<6, 6-12, and >12 months). We controlled models for patient age, gender, race/ethnicity, health insurance status, number of chronic conditions, smoking, and drinking status.
Results
The average age of the study participants was 60.4 ± 13.0, and 33.9% were men. More than 13.5% of the population was single, 77.8% were Black, 15.8% were Hispanic, approximately 16.5% were current smokers, and 16.8% were drinkers. About 92.4% of the samples had health insurance coverage, with 40.4% covered by Medicaid. While 88.2% of participants were proficient in English and the same proportion (87.7%) could read and write, about 89.5% had a steady place to live, and 5.8% were unemployed (see Table 1).
Association Between MTM and Hypertension
At baseline, the average systolic blood pressure (SBP) and diastolic blood pressure (DBP) in the study population were 137.3 mmHg (SD: 18.9) and 80.3 mmHg (SD: 13.8), respectively. After participation in the program, the SBP and DBP were reduced by 11 mmHg and 6 mmHg to 126.3 mmHg (SD: 15.7) and 74.3 mmHg (SD: 11.9), respectively. The findings showed that at baseline, 38.2% of the study population experienced uncontrolled hypertension. After joining the program, this figure was reduced by 17.5 percentage points to 20.7%. All reductions were significant at P < .01 (see Table 2).
Descriptive Analysis of Study of Population Health Outcomes.

Hypertension is defined as systolic BP ≥ 130 mmHg and Diastolic BP ≥ 80 mmHg.
To estimate the association between MTM and hypertension, we used a fixed effect logistic regression model, using the prevalence of hypertension after joining the program. The results of the adjusted model showed that 12 months after joining the MTM, the hypertension odds ratio had reduced (Beta: −1.81, CI: [−3.11, −0.51]; see Table 3). The results of the adjusted model showed that 12 months after joining the MTM, the SBP was reduced by 10.4 mmHg (Beta: −10.37; CI: [−19.62, −1.12]), and 12.4 mmHg reduced DBP (CI: [−19.8, −5.01]) by being in the program between 6 and 12 months but the effect diminished after 12 months.
Logistic Regression Model Estimates on the Impact of MTM on Hypertension, and Obesity.

Adjusted models have controlled patient age, gender, race/ethnicity, number of chronic conditions, smoking and drinking behaviors.
P < .05. **P < .01. ***P < .001.
Association Between MTM and Obesity
As presented in Table 2, before joining the program the participants had an average weight of 208.6 lbs (SD: 52.5), and BMI of 34.4 kg/m2 (SD: 8.1). After joining the program, average weight and BMI reduced slightly by −3.6, and <1 points. We did not find significant reductions in weight and BMI in the regression analysis (see Tables 3 and 4).
Regression Model Estimates on the Impact of MTM on Hypertension, and Obesity.
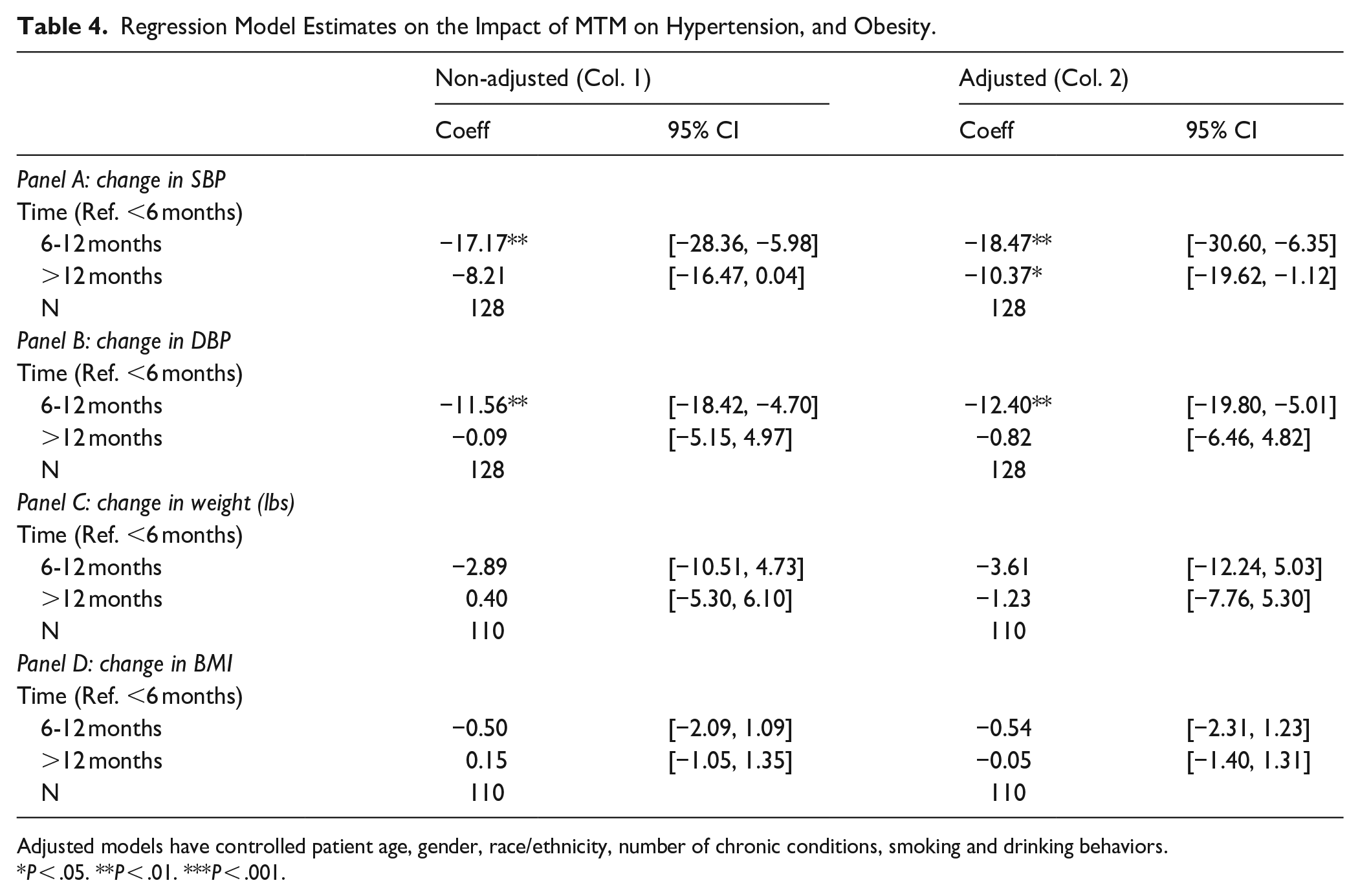
Adjusted models have controlled patient age, gender, race/ethnicity, number of chronic conditions, smoking and drinking behaviors.
P < .05. **P < .01. ***P < .001.
Discussions
This study investigated the association between MTM and blood pressure, BMI and weight. We found that participation in MTM led to a decrease in SBP of 10.8 mmHg and DBP by 5.6 mmHg. The prevalence of hypertension also significantly decreased in patients participating in the program for more than 12 months. Our findings align with those reported in previously published studies. Hirsch et al 30 demonstrated that a collaborative MTM service between PharmD and Primary Care Physicians (PCPs) effectively lowered blood pressure over usual care at 6 months for all patients, and at 9 months for those continuing with the pharmacist. Similarly, Planas et al 31 reported that a 9-month community pharmacy-based MTM program significantly improved blood pressure control among diabetics with hypertension, reducing mean SBP by 17.32 mmHg. Tilton et al. (2018) found that MTM clinic patients experienced more substantial reductions in both SBP and DBP at 6 and 12 months compared to controls. Prudencio et al 32 also noted improvements in hypertension control through comprehensive medication management. Moreover, a systematic review highlighted that MTM interventions typically resulted in clinically significant improvements in chronic conditions. 33 However, some studies report no significant changes, attributing this to small sample sizes. These findings suggest that while MTM can be effective in managing hypertension, outcomes may vary.34,35
MTM may prove particularly beneficial for populations with multiple chronic conditions or individuals residing in socially disadvantaged areas affected by SDOH, similar to the population in this study, 95.9% of whom had heart disease, and 50.3% of whom were diabetic (see Table 1). This approach will highlight the importance of information exchange and co-design, allowing us to better understand and prioritize the unique needs and preferences of populations affected by SDOH. Studies have shown that team CHWs model, 23 combining the Evidence-Based Pathways Community Coordination model 36 with community-based pharmacists, may play a critical role in the new MTM model by assisting patients in using biometric devices, such as blood pressure monitors, necessary for the MTM effort. This study showed that CHWs can play a critical role by assisting patients with biometric devices, supporting adherence to medication regimens, and providing virtual and in-person assistance. They can also collaborate with healthcare providers to identify high-risk patients, collect medical information, educate patients, facilitate communication, and contribute to quality improvement efforts. By leveraging the skills of CHWs, the new MTM model can improve patient outcomes and improve access to health care.
The consistent engagement between pharmacists and patients within the medication synchronization program provides many advantages. These include the early detection of errors, 25 enhanced adherence to medication regimens,26,27 improved oversight by pharmacists in managing medication-related issues effectively, and fewer missed doses. 28 By fostering proactive communication and collaboration, this approach facilitates the coordination of care and enables the identification and mitigation of barriers associated with social determinants of health. Ultimately, these efforts contribute to better patient outcomes and overall healthcare quality. 29
Lessons learned from PreventionLink should inform the development of new models of care delivery for Medicare beneficiaries. 37 MTM enables providers to monitor patients’ blood pressure outside conventional office settings. Although practices initially showed little interest in and telehealth MTM until the COVID-19 pandemic, 38 Federally Qualified Health Centers and PCPs are now recognizing its benefits. However, new challenges emerged related to reimbursement by payers.
Limitations
The COVID-19 pandemic impacted on the intervention’s implementation negatively, with staff shortages and turnover leading to delays and disrupted workflows, affecting data collection. The bi-directional electronic referral system launched at the end of Year 2 (August 24, 2020), and the MTM program launched on September 16, 2020, with no patient referrals in Year 2 due to system launch timing. While 17 pharmacies were interested in MTM participation, only 6 pharmacies and 9 pharmacists participated. The lack of involvement was attributed to sudden escalations in pharmacists’ workloads caused by the pandemic. The higher English proficiency and literacy of the study population predominantly may limit the generalizability of the findings to non-English speaking and/or low literacy populations.
Conclusions
MTM programs implemented by care teams consisting of community pharmacists, primary care physicians, and community health workers can significantly improve patient outcomes related to hypertension. Policymakers should promote MTM services and reimburse for CHW support and remote patient monitoring services as critical interventions for hypertensive populations, especially those affected by social determinants of health.
Footnotes
Appendix
CHWs Activities.

| CHWs activities |
|---|
| CHWs activities included but were not limited to: |
| (1) Patient enrollment and SDoH Assessment, including: |
| – Obtain schedule and patient eligibility list from provider |
| – Obtain consent form and provide PreventionLink one pager flyer to patient |
| – Complete the supplemental form for MTM |
| – P3 pulls labs, progress notes, and medication list to confirm eligibility |
| – Enter referrals for eligible patients identified by provider into CRISP |
| – Fax the consent form to PreventionLink |
| – Complete SDoH screening and upload SDOH assessment to SharePoint Folder (Community Health Workers—CHW Referrals—PreventionLink SDoH Initial Screening) |
| – Provide devices to patients who are referred to MTM and assist with connectivity and downloading the iHealth app. |
| (2) Connect patients with P3 during online virtual meetings. |
Acknowledgements
The rigorous evaluation was conducted by a team headed by Darrell J. Gaskin, PhD, the William C. and Nancy F. Richardson Professor in Health Policy and Director of the Center for Health Disparities Solutions, Johns Hopkins Bloomberg School of Public Health. The team, consisted of Darrell J. Gaskin, PhD; Hossein Zare, PhD; Roland J. Thorpe, Jr., PhD, Michelle Spencer, MS, Lois Dankwa, PhD, and Laurine Thomas, PhD, an independent health services research consultant, with expertise in qualitative methods. The PGCHD Evaluation team consists of Amber C. Allen, MPP, Jacob Riley MS, Debra Collier MPH, and formerly Donna Perkins, MPH, and Christina Gray MS. We thank you all members of the Prevention Team at the PGCHD including Twarnisha Stokes, MHSA, Augustine Amuta MD MSHIA, Deborah McGruder, MPH, Princess Clark, Monique Bowler, Ayanna Johnson, our primary care provider network, our CHWs, and our partners Totally Linking Care Maryland (TLC-MD), Health Quality Innovators (HQI), and University of Maryland School of Pharmacy P3 (Patients, Pharmacists, Partnerships).