
Abstract
Background:
Influenza in India is increasingly shifting from seasonal outbreaks to an endemic presence with potential pandemic risks. Despite ongoing surveillance to monitor regional virus circulation, it’s crucial to assess the unique socio-economic impact of influenza compared to other respiratory illnesses.
Methodology:
A retrospective study was conducted from October 2023 to October 2024, analysed 3 years of data from a south Indian tertiary care hospital. Children hospitalised with any subtypes of influenza infection were classified as Group 1, while those vaccinated with at least one dose of influenza vaccine from the hospital’s immunisation centre formed Group 2. Trends in infection burden and vaccine utilization among paediatric population were detailed, with separate calculations of the economic burden for each group, leading to a summarized cost-benefit analysis.
Results:
Over three-years, Group 1 included 93 children were with a confirmed positive influenza test, while Group 2 consisted of 453 children who received at least one influenza vaccine at the study site. Hence the study site marked an influenza infection rate of 13.62% and a vaccination rate of 6.93%. Infections were more frequent in children over 1 year (74.19%), while vaccine utilization was highest in those under one (91.83%). Boys had a higher infection rate (65.59%) and demonstrated greater vaccine utilization (56.51%). Vaccine underutilization was evident, with only 1.99% receiving timely boosters, and 23.84% missing them. Infections were more prevalent among middle and lower-income children (86.02%), while vaccination rate was higher in upper income families (81.01%). Vaccination cost was 7.76 times lower than treatment; averaging INR 3252.21 (38.73 USD) per child, compared to treatment at INR 25 237.1 (300.14 USD). Net benefit ranged from INR 611 658.99 to INR 1 135 938.12, based on ±30% wage variations within the study community.
Conclusion:
The study underscores the economic benefits of influenza vaccination; with costs nearly eight times lower than treatment. However, socio-economic disparities in vaccine utilization emphasize the need for targeted strategies to improve access in lower-income groups.
Introduction
The twentieth century witnessed three major influenza outbreaks caused by different antigenic subtypes: H1N1 (1918), H2N2 (1957) and H3N2 (1968). These outbreaks were named after their presumed sites of origin as Spanish, Asian and Hong Kong influenza respectively. 1 In addition to these pandemics, there were numerous epidemics, pseudo-pandemics and outbreaks of influenza such as those in 1947, 1976 and 1977, highlighting the potential of these viruses to escalate into pandemics. The Spanish flu, for instance, resulted in 20 to 50 million deaths in 1918. Comparatively, the COVID-19 pandemic (2019), saw an estimated mortality of over 3.4 million.2,3 Despite the novel Corona-virus being more virulent than the influenza virus, the timely introduction of COVID-19 vaccines averted approximately 14.4 million deaths within the first year of the pandemic. 4
The global burden of influenza infection is estimated to result in 290 000 to 650 000 respiratory deaths and 3 to 5 million severe illnesses each year. 5 In 2018 alone, there were approximately 109.5 million influenza episodes worldwide among children under 5 years old, leading to 15 300 (4%) deaths and 870 000 (7%) hospital admissions. 6 In low and middle income countries (LMICs), the expenditure related to annual seasonal influenza infections is estimated to range from 2% to 6% of Gross Domestic Product (GDP) per capita, while in developed countries, it accounts for 0.04% to 0.13% of GDP. 7 Estimation the actual mortality rate of influenza infections is challenging because it is not always listed as an underlying cause of death certificates. Hence, national vital records and consistent surveillance data are utilized to determine the socio-economic burden. However, the availability and the quality of such data resources in LMICs are often compromised. 8
India’s tropical climate and its diverse population, which accounting for 17% of the world’s population, create a conductive environment for the circulation of seasonal influenza virus. Although the timing of influenza varies across the country, peak circulation is typically observed during the monsoon season (June-September), with a secondary peak during the winter months (November-February). 9 Children are found to be 20% to 30% more vulnerable than adults, likely due to their low exposure to previously circulating virus strains. In addition to the socio-economic burden resulting from recurrent school absenteeism and hospitalisation of infected children, they may also act as potential carriers for an extended period (with high virus titres observed for up to 2 weeks). 10 This underscores the importance of introducing influenza vaccines as mandatory childhood vaccination in the country.
The recent substitution of quadrivalent influenza vaccines for the traditional trivalent-vaccines (which were used up to 2018-2019 in India), ensures improved protection against the circulating influenza virus subtypes. 7 However, the unpredictability and variability in climate, along with the constant circulation of the virus and the emergence of new viral strains, pose challenges in determining the optimal timing for vaccination in the country.5,7,9 Additionally, the lack of data for estimating the burden of influenza further complicates. 9 The Indian Academy of Paediatrics (IAP) Advisory Committee on Vaccines and Immunization Practices (ACVIP) has updated the recommendation for influenza vaccination to include individuals for all ages, rather than limiting it to higher risk groups. 11 Children aged 6 to 23 months are particularly vulnerable to seasonal influenza infections, hence the current recommendations suggests administering the first dose at 6 months of age, followed by a second dose after 1 month (with at least 4 weeks between doses), followed by an annual booster dose up to 5 years of age. 11
Optimizing the usage of influenza vaccination still poses a challenge due to varying characteristics of the virus strains. However, studies have shown that the effectiveness of influenza vaccine, particularly in children ranges from 44% to 74% depending on the type and strain of the virus. 12 This study aims to correlate the socio-economic burden experienced by infected children with the cost-benefit analysis of regular vaccination in children under age of five. It will examine various economic aspects such as hospital admissions, loss of parental work pay, school absenteeism, medication cost, secondary illness and more in influenza-infected children. Additionally, the study will analyse current influenza vaccination trends and utilization patterns as well as discuss the safety profile and benefits of regular vaccination.
Methodology
The study was conducted retrospective in the paediatric department of a tertiary care hospital in the southern India. The study duration was 1 year, from October 2023 to October 2024 and involved retrieving relevant study data from previous 3 years (2021-2023). The study population was divided into two groups. Group I included all children under 18 years of age who had been admitted to the paediatric ward for at least for 1 day with suspected influenza infection in the past 3 years. Group II consisted of children less than 18 years who had received at least one dose of influenza vaccine from the immunisation centre at the study site during the same three-year period. Adults over 18 years of age and those who were not interested in participating in the study were excluded from the study.
The details of children admitted with suspected influenza infection were obtained from the notifiable-disease registry maintained in the paediatric ward of the study site. This information included admission details, diagnosis, microbiology reports, treatment charts, duration of hospital stay, previous vaccination history, any medical complications and contact details. All patient medical files are maintained by the Medical Record Department of the study site. To estimate the economic burden of influenza infection, various medical and related expenses associated with each patient calculated separately (obtains from the medical file). These expenses included registration fees, bed charges, laboratory charges (bio-chemistry, pathology and microbiology), nebulisation charges, surgical dressing materials charges, special equipment charges, service charges and miscellaneous expenses. Additionally, medication costs, including discharge medications were estimated based on the treatment chart of each patient. The cost of medication was determined by multiplying the frequency of medication by the cost per tablet/sachets/product and then summing up these costs for each patient.
Indirect expenses incurred during the hospital stay, including costs for food, bystander expenses, and transport were estimated based on the duration of stay and number of bystanders. These expenses were then compared to the national average cost of living per day. The socio-economic burden on the patient such as the number of school days missed and the loss of income for parents or bystanders was approximately calculated by multiplying the family’s daily or monthly income by the number of lost working or school days. The socio-economic status of each patient’s family was assessed using modified Kuppuswamy socio-economic scale (2021-2023), based on the hospital admission year of the child, to understand the broader impact of the infection on the community. Additionally, any information required to estimate the indirect cost related to the hospitalisation of this population was obtained through direct telephone contact with the parents (using contact details available from the patient’s medical file). The severity associated with different subtypes of influenza virus and their incidence rates were noted separately. Any additional complications or secondary illness occurring alongside the influenza infection were differentiated and categorised based on the system organ classification list.
Similarly, the study team gathered comprehensive details of influenza vaccine beneficiaries at the study site over the same time period (2021-2023). Information such as the number of doses administrated, vaccine brand and type, utilization rates, safety profiles and previous infection details (if any) was retrieved from the ‘Childhood Immunisation Registry’ – a digital database maintained by the study site. Basic demographic information including age, gender, contact details and socio-economic status (assessed using the Kuppuswamy scale (2021-2023) based on the child’s year of vaccination), was collected for each vaccines. The cost of each administrated vaccine dose/s was estimated based on current market prices to calculate the total expenses incurred by each vaccine beneficiary in the study. The safety profiles of the influenza vaccine were also obtained from the digital registry, which collects data through both active and spontaneous reporting systems at the study site. Additionally, any expenses associated with Adverse Events Following Immunisation (AEFIs) during the study period were documented for each vaccine beneficiary. The study site is one among the World Health Organisation’s (WHO) recognised sentinel site for multi-country collaborative vaccine safety studies in 2018. 13 Hence all the reported Adverse Events (AEs) and their causality assessments were extracted from the database of the study site.
Statistical Analysis
The incidence rate of influenza infection among the study population was calculated by dividing the total number of influenza cases by total number of children hospitalised (at the study site during the same period of time) with any respiratory tract infection multiplied by 100.
A cost-benefit analysis was conducted between the influenza vaccine utilizers and patient’s hospitalised with influenza infection in the study site during the same period of time (2021-2023). A sensitivity analysis was conducted by varying the daily wages across the different socio-economic classes, reflecting the broad range of income levels in the study population. The daily wages were calculated by dividing the monthly income brackets by 26 (the average number of working days in a month). The analysis considered variations in daily wages from a low of ₹384.65 (for participants in the lowest income bracket) to over ₹7686.23 (for those in the highest income bracket). The socio-economic class was determined based on the Kuppuswamy scale included in the Supplementary Table for the reference.
Results
A total of 683 children were admitted to the paediatric ward of the study site over the past 3 years with various Respiratory Tract Infections (RTIs). Of these, 17.13% (n = 117/683) were hospitalised on suspicion of influenza infection, as identified through the notifiable disease registry of the study site, and 13.62% (n = 93/683) were confirmed with a positive laboratory test for influenza. Among the children with suspected influenza infection (n = 117), 7.69% (n = 9/117) tested positive for COVID-19, 9.4% (n = 11/117) had influenza like symptoms but tested negative for influenza, and 3.41% (n = 4/117) had flu like symptoms that were not associated with the influenza virus upon further differential diagnosis. Therefore the incidence rate for influenza infection at the study site was estimated to be 13.62% (n = 93/683), after excluding the cases positive for COVID-19, negative flu test and different diagnoses. The second group comprised 578 children who received influenza vaccine at the study site during the same period (2021-2023). The percentage of influenza vaccination utilization at the study site was calculated as 6.93%, which is the number of children received the influenza vaccine (n = 453) divided by the total number of children who received various childhood vaccines during 2021 to 2023 (n = 6536) multiplied by 100. A detailed representation of the two study cohorts is illustrated in Figure 1.

Outline of the study population participated in the study.
During the study period, the incidence of influenza infection was notably higher among boys (65.59%, n = 61) compared to girls (34.41%, n = 32). Similarly, boys (56.51%, n = 256) accounted high utilization of influenza vaccination as compared to girls (43.49%, n = 197). The majority of vaccine beneficiaries (76.38%) received one dose of the influenza vaccine, while 21.63% received two doses and a very few (1.98%) received booster doses. A high incidence of infection was reported among children aged 1 year to 5 years (87.09%), while the highest vaccine utilizers (91.83%) were children less than 1 year old. The burden of influenza infection was predominantly seen in the upper-lower and lower-middle classes (86.02%), while maximum vaccine utilization was among the upper and upper-middle classes (81.01%). The demographic characteristics and socio-economic comparisons of both study cohorts are depicted in Figure 2.
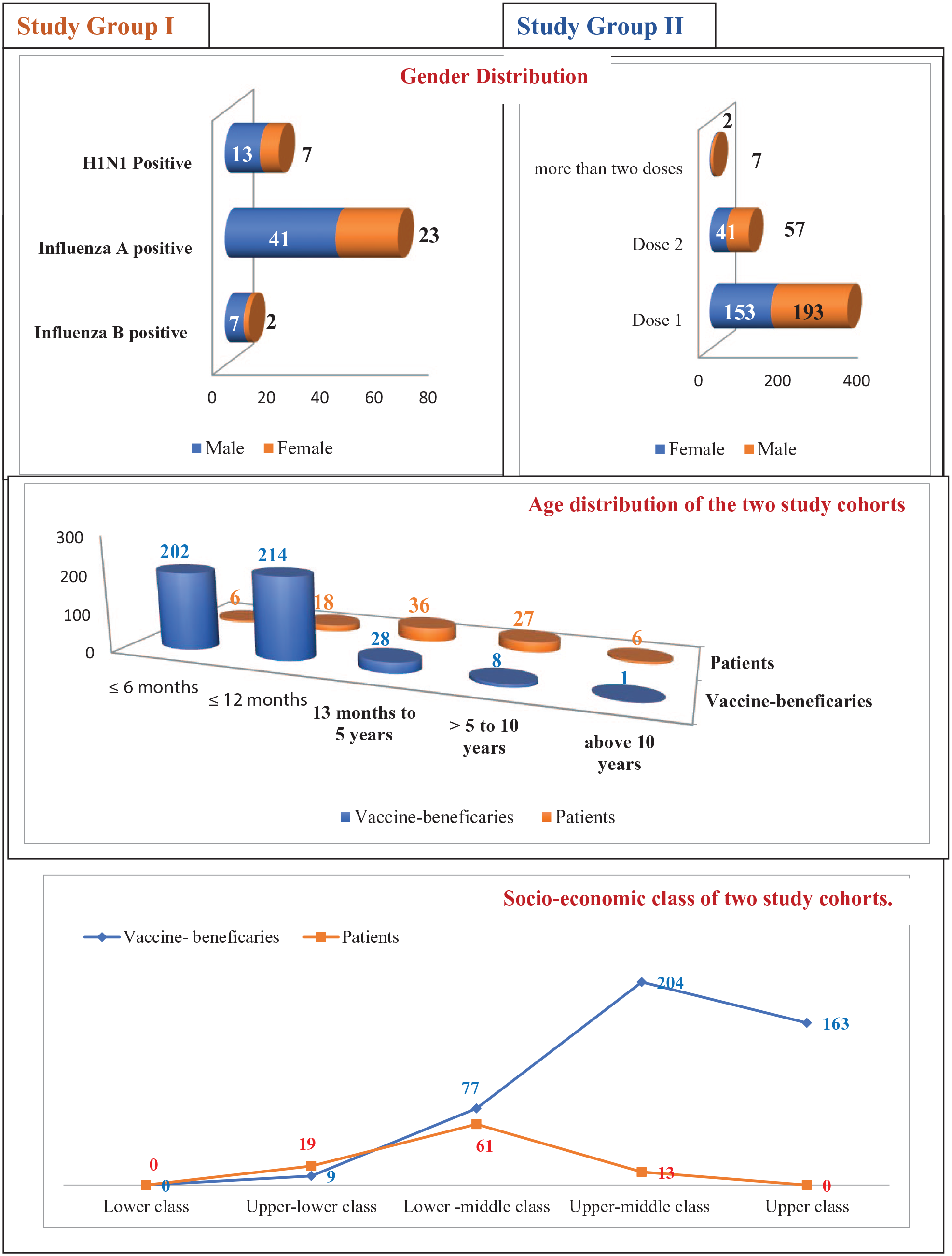
Demographic characteristics of the study population.
In 2021, no hospital admissions related to influenza infection were observed, and the utilization of the influenza vaccine (2.5%) was also low at the study site. Influenza vaccination uptake began in the late phase of 2021 and gradually increased in the following (2022-2023). The first influenza case requiring hospital admission at the study site occurred in May 2022, with a peak admission in August (11.83%). In 2023, there was a significant increase in hospital admissions related to influenza infection (74.19%). A detailed distribution of both study cohorts during the study period was shown in Figure 3.

Distribution of two study population during the study period.
The Burden of Influenza Infection (Group 1) and Incidence of Adverse Events Following Immunisation (AEFI) Among Vaccine Beneficiaries (Group II)
The highest incidence of influenza infection was observed in children aged 5 to under 10 years, with a rate of 37.63% (n = 35). The total incidence of Influenza infection among the study population was estimated to be 13.62%, with 30.11% (n = 28) of the affected children having multiple diagnosis and 5.38% (n = 5) having known medical conditions, such as Type 1 Diabetic mellitus, Inborn errors of metabolism (IEM), G6PD deficiency, seizure disorders. Additionally, an AEFI incidence of 8.83% (n = 40/453) was recorded among the influenza vaccine beneficiaries during the study period. The distribution of various diagnoses (including co-infections) in Group 1 and AEFIs reported in Group 2 were categorised and depicted based on System Organ Classification (SOC) in Table 1.
Distribution of Diagnosis (Study Group I) and Incidence of AEFIs (Study Group II) Based on System Organ Classification (SOC).

More than one diagnosis in a patient, provided a count of 117 disorders in 93 patients.
A total of 117 different diagnoses related to influenza infection were made among the study population (n = 93) during the study period. Respiratory-related disorders were the most frequently reported diagnosis (57.26%), followed by general (14.53%) and gastro-intestinal (11.11%) disorders. The burden and complications related to the infection among the study population (study Group 2) are depicted in Table 1. Each patient had an average hospital stay of 5 days and exhibited minimum of 2.64 ± 1 symptoms. The most common symptoms reported were cough (persistent for an average of 4-15 days), fever (2-6 days), vomiting (1-3 days), loose stools (2-6 days), breathing difficulties (3-5 days) and generalised weakness and body pain (7-30 days). Additionally, six patients experienced severe symptoms such as febrile seizures, convulsions and acute encephalitis during the study period. Among the vaccine beneficiaries (Group 2), general disorders and administration conditions were the most frequently reported AEs (82.5%). Majority of the events were mild to moderate reactions, while two children experienced serious anaphylactic reactions following the first dose of the influenza vaccine, which required hospitalisation.
Economic Burden Caused by Influenza Infection in Children (Group I)
The total economic burden associated with influenza infection in Group I was calculated by adding both the direct and indirect costs related to hospitalisation and other intangible expenses. The average cost per person associated with each variant of the influenza virus was calculated separately, along with the total cost (Table 2). Overall, the study estimated the total expenditure related to influenza infection as Rs.2 347 047.48 (27 913.39 USD), with an average of Rs. 25 237.1 (300.14 USD) per person (total expenses divided by number of infected children, n = 2 347 047.48/93) in study Group 1. The direct costs (Rs. 1 243 635.46, that is, 14 790.53 USD) related to influenza infection were higher than the indirect costs (Rs. 1 103 412.02, i.e., 13 122.20 USD). The average economical burden associated with H1N1 cases (32 606.70 per person) was found to be higher than that of other subtypes reported in the study. However, the average cost per case for influenza B subtypes (Rs. 28 857.54) were higher than for other influenza A subtypes (Rs. 22 424.93).
The Economic Burden Among Influenza Infected Children at the Study Site (Calculated Both Direct and Indirect Cost).

Several parameters used to calculate the total indirect expenditure related to the infection. Such as the loss of pay per guardian was determined based on the monthly income of the parent or family head (according to modified Kuppuswamy scale). Additionally, 61.29% (n = 57/93) of the children were of school-going age, so the loss of school days was calculated by categorising these children into different socio-economic classes using Kuppuswamy scale. This categorization provided an approximate monetary value for the indirect expenses related to the infection.
The overall expenditure for influenza vaccine beneficiaries was estimated to be Rs. 1 473 248.93 (17 545.85 USD), with an average cost of Rs. 3252.21 (38.73 USD) per person (calculated as n = 1 473 248.93/453). The total direct expenses related to vaccination amounted to Rs. 874 704.39 (10 417.45 USD), while the indirect costs was Rs. 598 544.54 (7128.55 USD). Both direct and indirect expenses associated with influenza vaccination in the study Group 2 are detailed in Table 3.
The Economic Burden Among Vaccinated Children at the Study Site (Calculated Both Direct and Indirect Costs Related With Vaccination).

Direct costs include the price of the vaccine, vaccination charges, physician consultation fees and any costs related to AEs and Over the Counter (OTC) medications for managing AEFI for each dose received by Group 2. Indirect costs were calculated by considering lost work days of parents who accompanied their children to the immunisation centre. These were determined by multiplying the number of hours or days lost due to the vaccination by the parent’s daily wage. The individual calculation of lost work hours or days is presented in the Table 2 for the reference. It is important to note that most of the vaccine beneficiaries who experienced an AEFI were not school-going children; hence expenses related to missed school days were not applicable in this cohort.
The cost benefit analysis conducted between group 1 and 2 provided a positive net benefit value, represented in Table 4. However sensitivity analysis was performed by adjusting the indirect costs based on variations in daily wages, considering 10%, 20% and 30% variations respectively. Here we assume that the indirect costs are proportional to the daily wages, hence we apply the percentage changes to the total costs to estimate the total cost and net benefit variations under different scenarios (Table 5). Table 5 shows that the recalculated net benefit remains positive across all scenarios, demonstrating that the benefits of vaccinating children against influenza outweigh the associated infection-related costs.
Cost-Benefit Analysis Between Influenza Infections Affected Children (Group 1) and Influenza Vaccine Beneficiaries (Group II).

Sensitivity Analysis of Recalculated Net Benefit Based on Changes in Daily Wages Across Different Socio-economic Classes.

Discussion
Despite the long-standing recognition of the threat posed by viral infections and the protective power of vaccines, seasonal influenza continues to impose a significant burden on the Indian population. During the study period, 11.21% of paediatric admissions were due to respiratory-related illnesses. Of these, 17.13% were suspected of having an influenza infection, and 13.62% were confirmed cases. In contrast, 6.93% of children received at least one influenza vaccination at the study-site, while only 3.46% had completed two doses. This highlights both the considerable burden of influenza compared to other respiratory illnesses and the underutilization of vaccines among the paediatric population. Although Influenza vaccines have been available in India since 2004, they are still excluded from national childhood immunization programs due to limited data on the disease’s burden and the vaccine’s safety and effectiveness.14,15
Although the study did not excluded children with a history of vaccination or pervious infection from Group 1 and Group 2 respectively, none of the infected children (Group 1) had received any vaccine doses and none of the vaccinated children (Group 2) contracted influenza during the study period. This may be attributed to the fact that the majority of infected children in Group 1 belonged to lower-middle class families, who faced financial barriers to vaccination and were at higher risk of community-based infections. On the other hand, vaccine utilizers in Group 2 predominantly came from upper-middle class families, who could afford the vaccine and had a lower risk of exposure due to their socio-economic status and living conditions. A similar socio-economic gradient in immunization coverage across the country was observed in a study conducted using data from the National Family Health Survey (NHFS-4) 2015 to 2016. 16 The infection patterns identified in this study align with those reported by India’s Integrated Disease Surveillance Program (IDSP), showing a high incidence of influenza A viruses, an increase in H1N1 infections from previous years, low rates of influenza B infections and similar seasonal spikes. 17 Although multiple influenza outbreaks recorded in India since 2006, the study-site had documented only a few cases in previous years (just two cases since 2017, with no prior reports in children). The gradual rise in infections since 2021 (at the study-site) may be due to increased patient in-flow, favourable climatic conditions, low herd immunity and post-COVID immunity alterations. Globally, studies have observed that pandemic-related behaviours reduced the genetic diversity and circulation of influenza viruses.18,19 However, the recent post-pandemic surge in influenza cases across India can be linked to alerted individual immunity, as well as non-adaption of flu vaccines following the pandemic.20,21
The study also observed a steady increase in the utilization of influenza vaccines from 2021 to 2023. No vaccines were utilized among the study-population until October 2021, followed by a rapid uptake in 2022 and 2023, particularly in the months of April and November. A previous study conducted at the site indicated low usage of optional childhood vaccines, but influenza vaccine uptake surged post-pandemic as parents became more willing to pay out of pocket. 22 Before the pandemic, the influenza-vaccine coverage was low in the country due to its cost, hesitancy, safety concerns and limited awareness among Healthcare workers (HCWs).23,24 However, this study found that influenza vaccine utilization was highest among children under 1 year of age (91.83%), whereas infections were more common in those over one-year (74.19%). Additionally, booster doses (recommended for children up to 5 years in the country) were underutilized at the study-site. Only 1.99% of children received timely booster vaccinations, and 23.84% (n = 108) of eligible children remained unvaccinated. This highlights the need to track and educate partial-vaccinators to maximize the benefits of regular vaccination. A cross-sectional study based on the NFHS 2015 to 2016 found that only 62% of the children aged 12 to 23 months received full vaccination coverage as recommended, 25 and only 38% to 39% of the eligible children were benefited with optional vaccines. 26 Low or partial vaccination coverage in the country is attributed to various socio-demographic factors, including maternal education, financial constraints, birth order and social category.25-27
This study also could highlight certain socio-economic disparities in the utilization of influenza vaccination. Vaccination rates were higher in boys (56.73%) than in girls (43.27%), and the likelihood of receiving multiple doses was also greater among boys (9.49%) compared to girls (5.52%). This observation is consistent with the study conducted by Panigrahi et al, 28 which observed a male preference for all optional vaccines including influenza, apart from varicella doses among Indian children. Furthermore, children from upper (35.98%) and upper-middle-class families (45.03%) had the highest vaccine utilization, while only 1.97% of children from upper-lower families could afford it. This indicates that affluent segments of society benefited most from vaccination, while infections were more common among lower-middle and upper-lower families. Mathew et al 29 points out that these inequalities among disadvantaged groups have not been adequately addressed by existing policies and immunization programs, where optional vaccines are often treated as consumer-driven products rather than being guided by scientific considerations.
The burden of infection was mainly associated with influenza A subtypes, with lower severity in H1N1 at the study-site. Neurological complications were more common in other influenza A subtypes (4.27%) compared to H1N1 strains (0.85%). In contrast, a study from south India reported a higher incidence and severity of paediatric H1N1 cases over eight-years. 30 The burden of AEFIs among vaccine-beneficiaries (Group 2) was 8.83% with 0.44% experiencing serious reactions like anaphylaxis. Vaccine safety studies conducted among Indian children under five shown a favourable safety profile with low rates of serious AEs. 31 However, vaccine utilization at the study site was significantly lower than recommended. Of the required five doses per child by age five, only 679 doses were administered to 453 children, reflecting just 30% of the recommended vaccination coverage. Additionally a 2016 study by Mark et al, 32 demonstrated no significant difference in the Vaccine Effectiveness (VE) between partially and fully immunized children, though two doses before the infection season led to higher VE. Here, the vaccination cost analysis focused on children who received at least one dose, disregarding their partial or full vaccination status to facilitate easier comparison.
Overall, the average cost of influenza infection from any subtype (INR 25 237.1 or 300.14 USD) far exceeded the average cost of vaccination (Rs. 3252.21 or 38.73 USD), making treatment approximately 7.76 times more expensive than prevention. Furthermore, the study estimated a net benefit of INR 873 798.55 (10 392.07 USD), emphasizing that a vaccinated child saves approximately INR 21 984.89 (261.41 USD) than an infected child. Putri et al 33 estimated the 2015 annual total economic burden of seasonal influenza in the United States at $11.2 billion (ranging from $6.3 to $25.3 billion), with indirect costs ($8 billion) surpassing direct costs ($3.2 billion). This study estimated that 52.99% of expenditure were related to direct costs, while 47.01% were indirect costs, likely because the study focused solely on paediatric population. de Courville et al 34 found that secondary illness among infected children accounted for 34.98% (INR 434 980.78) of total direct costs, suggesting fewer complications within the study group. However, Macias et al 35 noted a severe infection burden from secondary complications beyond the respiratory system. The study population included a socioeconomically mixed community, results in variable average expenditures per infected child, ranging from INR 17 665.95 to INR 32 808.19 (±30% based on wage variations). Limited research has estimated the economic burden of influenza in India, though Ram et al 36 reported monthly out-of-pocket expenses for infectious disease at INR 881.56 per out-patient case and INR 1156.34 per in-patient case. These findings underscores the specific economic impact of influenza infection across different populations in developing country.
Though influenza type A variant infections were more common, children with the H1N1 strain faced the highest expenses, averaging INR 32 606.7 per case, followed by those with influenza type B, with an average cost of INR 28 857.54 per head. The economic-burden of any influenza variants imposed similar financial strain on the study population, as the majority came from middle or lower-income backgrounds. At this point, the role of influenza vaccination in reducing the economic burden of infections becomes evident. Even though this study was limited to partial vaccine users; it estimated an average vaccination cost of INR 3252.21. This suggests that while vaccination helps prevent infections, covering all recommended doses still imposes a substantial financial burden. Ortiz et al 37 highlighted additional obstacles in LMICs beyond cost, including annual revaccination needs, frequent vaccine re-formulation, and weak delivery and tracking infrastructures due to differing age patterns from traditional childhood immunization. Hence expanding favourable vaccine policies to increase access across all socio-economic groups is essential to broaden the economic benefits of vaccination nationwide.
India hosts the world’s largest immunisation programme, the Universal Immunisation programme (UIP) established in 1985, however cost and implementation disparities across districts and states impact vaccine affordability and access, particularly for underprivileged groups. A recent study on district-level public finance estimated that providing all basic vaccines nationwide would cost 784.91 million USD, while 1.73 billion USD would be needed to fund all vaccines recommended by the government. 36 The study also pointed that in order to achieve universal immunisation, the budget for India’s UIP should be increased form its 2020 level of 1.58 billion USD. 37 Despite a significant budget increase for child and women’s health in 2024, influenza vaccines are excluded from the UIP, can be due to limited burden data, regional variability, and costs for frequent re-formulation to match changing strains.11,35 Hence, advancements in national policies and initiatives for more efficient vaccination coverage are essential to help mitigate potential financial losses.
Conclusion
The study reaffirms that prevention is economically more advantageous than treatment. Infectious diseases have had a significant economic impact on the population over the years, highlighting the need for timely interventions to support the economy, especially in a country with diverse ethnic backgrounds. Favourable climatic conditions, frequent strain variations, low adaptability of vaccine formulations, prioritization of other childhood vaccines and limited funding for state immunisation efforts all signals an urgent need for action. However, in a developing country like India, prevention care remains largely accessible to wealthier is segments of society, with affordability as a primary factor contributing to major health inequalities.
This study highlights two key observations; firstly, influenza imposes a significant economic burden, particularly among paediatric population, indicating that many remain untreated, which could lead to unexpected regional outbreaks. Second, there has been an increased acceptance of influenza vaccines, spurred by the COVID-19 pandemic, among parents. However, access remains largely limited to wealthier segments of society. Additionally, the prevalence of partial or incomplete vaccination suggests a lack of awareness, as most children received only some of the recommended doses. A gender preference favouring boys for optional vaccines and booster doses also raises questions, warranting further in-depth evaluation. Overall, the study concludes that while vaccination provides clear economic benefits, these advantages are currently skewed toward wealthier segment, with the infection burden disproportionately affecting disadvantaged groups.
Limitation of the Study
The study was limited to children admitted to a single centre, so it could not document the full community burden of infection. However, the study showed a steady increase in influenza incidence compared to previous years, indicates a potentially greater burden in the area. Unlike Group 1, which included only children who could afford tertiary care, Group 2 represented a mixed community, with access to both free mandatory vaccines and paid optional vaccines, allowing insights into vaccine preferences and behaviours. However, the choice for influenza vaccination was solely at the discretion of parents, and this study did not explore various factors influencing their decision due to its retrospective design. Still, the study observed specific trends in vaccine utilization patterns.
To estimate the indirect costs, parental daily wage losses were calculated using the Kuppuswamy scale for Indian socio-economic status, based on profession and income. Variability in income status led to a sensitivity analysis to reduce differences in the calculated net benefit between infected and vaccinated children. Finally this study could not evaluate the long-term impact of vaccines, such as vaccine effectiveness or the benefits of natural immunity acquired by infected children.
Supplemental Material
sj-jpg-1-jpc-10.1177_21501319251332150 – Supplemental material for Correlating the Socio-Economic Burden of Influenza Infections and the Cost-Benefit of Vaccination in Paediatric Populations
Supplemental material, sj-jpg-1-jpc-10.1177_21501319251332150 for Correlating the Socio-Economic Burden of Influenza Infections and the Cost-Benefit of Vaccination in Paediatric Populations by Merrin Mathew, Narayanappa Doddaiah, Sakeer Hussain, Nandana Suresh Nambiar, Rovin Mathew Theempalangad, Sinchana Narayanappa and Rattehalli Ashwath Narayan Shrisagar in Journal of Primary Care & Community Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.