
Abstract
This paper presents findings from a study focused on establishing Postgraduate Nurse Practitioner (NP) and/or Physician Assistant (PA) Training Programs within federally funded health centers and look-alikes. The study aimed to identify facilitators and barriers encountered by participating health centers in the Health Resources and Services Administration (HRSA) funded Postgraduate NP and/or PA Training Programs Learning Collaborative. Of the 78 health centers that participated in the learning collaborative since 2016, 47.44% (n = 37) responded to the survey. The top facilitators for launching a program were leadership support, clinical support, and dedicated time for planning and implementation. The top barriers for not launching a program were lack of financial resources, competing priorities, and limited dedicated time for planning and implementation. Interviews echoed these findings, as well as highlighted additional facilitators of grant funding and mission-driven workforce pathway planning. Survey results from those that launched a training program revealed that 215 graduates have completed the program, with 86 employed within the health center. These findings provide valuable insights and guidance to support health centers in their journey towards building and launching a Postgraduate NP and/or PA Training Program, as well as informing future HRSA policies, programs, and funding.
Keywords
Introduction
Health centers are community-based and patient-directed organizations that deliver comprehensive, high-quality primary care services to over 31 million patients across the United States (U.S.). Since their inception in the 1960s, health centers have played an important role in improving the health and well-being of the communities they serve, as well as in understanding the impacts of social drivers of health (SDOH). Additionally, health centers are crucial to increasing access to primary care by reducing barriers, including distance, language, and lack of insurance. 1
In November 2022, the National Center for Health Workforce Analysis (NCHWA) under the Health Resources and Services Administration (HRSA) released workforce projections through 2035 with the hopes of understanding how changes in population will affect workforce demands within health centers. Nationally, across all physician specialties in the U.S., there is a projected shortage of 81,180 full-time equivalent (FTE) physicians. Conversely, these workforce projections also demonstrate an excess of nurse practitioners (NPs) and physician associates (PAs). However, the over-projected NP and PA workforce could mitigate the projected physician shortage in primary care, but only if these advanced practice providers are fully prepared for practice in the challenging setting of health centers. 2
In response to the projected workforce shortages, health centers must begin to establish career development pathways to educate trainees across all disciplines who provide care for the medically underserved. Rather than filling a job vacancy, “growing your own” presents the opportunity to increase competence and confidence of pre-licensure and postgraduate health professionals. 3 New graduates often lack training in settings that welcome vulnerable populations, and therefore are often overwhelmed by the complexity of the patients that health centers serve. 4
In 2005, Dr. Margaret Flinter, Senior Vice President/Clinical Director for Community Health Center, Inc. (CHCI) and Moses/Weitzman Health System (MWHS), and a family nurse practitioner who started at CHCI in 1980 as a National Health Service Corps (NHSC) scholar, published her observations on the very difficult transition that new NPs often experience when coming into primary care in the setting of a community health center. 5 Dr. Flinter identified the absence of formal postgraduate training for new NPs as the major contributing factor. 5 The new graduates were well-educated and fully committed, but simply had not had the breadth and depth of clinical experiences needed to prepare for the level of complexity presented in health centers. In response to this, CHCI launched the country’s first Postgraduate NP Residency Program in 2007. As of March 2025, there are now approximately 550 NP and joint NP/PA postgraduate residency and fellowship training programs found in 48 states across the U.S. Of those 550 programs, 20% are located in health centers. 6
In 2020, CHCI sought to understand the impact of the Postgraduate NP Residency Program on the subsequent career paths of the NP alumni (n = 90; 86 family nurse practitioners and four psychiatric mental health nurse practitioners) who completed their program between 2008 and 2019. From the 65 survey respondents (72% response rate), most (74%) were practicing as primary care providers, and the majority (57%) were practicing at a federally qualified health center. As for the perceived impact of the program on their current practice/career, the majority of the participants indicated that the program impacted their clinical practice (89%), career development (74%), and leadership development (52%) “to a great degree” or “to a considerable degree.” The participants perceived that they were very well qualified for practice and better prepared than their peers who had not completed a residency program, and some indicated that they were qualified with clinical skills beyond other experienced providers. Ultimately, all of the participants indicated that the Postgraduate NP Residency Program was important in today’s healthcare environment. The overarching theme of the mixed methods study was that the residency program was foundational to a successful career in community-based primary care and that the impact of the program continues to evolve. 7
Elements of a Postgraduate NP and/or PA Training Program
Since CHCI launched the country’s first Postgraduate NP Residency Program, the model has successfully demonstrated scalability as hundreds of programs across the country have subsequently launched. Typically, this model is a 12-month period of full-time employment, with a post-residency commitment ranging from 1 to 2 years. The Postgraduate NP and/or PA Training Program typically begins in August or September following the completion of graduate level study allowing for new graduates to complete their qualifications for licensure and begin practice in the state in which the health center is located. As fully licensed, board-certified NPs or PAs, new graduates are eligible for credentialing, privileging, and appointment to the health center staff.
As published in the Training the Next Generation Residency and Fellowship Programs for Nurse Practitioners in Community Health Centers Book, 3 the NP and/or PA training program combines clinical practice, didactics/seminars, and quality improvement and leadership training, consisting of about 2,000-hours following a 40-hours per week over 50-week schedu. Direct clinical experience make up 80% of the residents’ time in the program: 40% for Precepted Continuity Clinics, 20% Mentored Clinics, and 20% Specialty Rotations. The remaining 20% of time is for residents to attend didactic education sessions (15%) and quality improvement (QI) training (5%) for the remaining. For the entire year long residency, residents keep a reflective journal, which they submit to the program faculty weekly for review and response. See Table 1 for a complete description of each element of CHCI’s Postgraduate NP Residency Program.
Elements of CHCI’s Postgraduate NP Residency Program.

Postgraduate NP and/or PA Training Programs Learning Collaborative
In 2015, CHCI was awarded the National Training and Technical Assistance Partners (NTTAP) grant on Clinical Workforce Development funded by HRSA. 8 This funding has supported CHCI’s efforts to offer health centers nationally free training and technical assistance (T/TA) focused on Postgraduate NP and/or PA Training Programs. One of the NTTAP’s T/TA offerings is a hands-on learning collaborative opportunity, which provides a comprehensive overview of the residency program, taking health centers from building the case (e.g., program drivers, mission and vision, and gaining support from leadership and board of directors) through program accreditation. The objectives of the learning collaborative include: building the case for starting a program; identifying the clinical and financial resources required; identifying the operational and administrative support; determining the structure and curriculum; establishing the processes for evaluating learner outcomes and the impact of the program; and preparing for program accreditation.
The opportunity to participate was communicated through CHCI’s email blasts and HRSA’s weekly newsletter, Primary Health Care Digest. Interested health centers submitted applications and provided written acknowledgement from leadership of the learning collaborative’s expectations. Upon receiving the health center’s application, interviews were held with each applicant. Interviews focused on the team’s organizational goals, commitment that their teams would have the time and resources to participate in the collaborative, and confirmation that the health center team could make decisions about organizational change related to establishing a Postgraduate NP and/or PA Training Program. The interviews were also an opportunity to review the learning collaborative goals, objectives, and syllabus. Once the health center was accepted into the learning collaborative, they confirmed their participation by sending the names, titles, and emails of their team members and team coach. Health center team members typically comprised of NPs, PAs, Chief Executive Officer (CEO), Chief Medical Officer (CMO), Medical Director, Chief Operating Officer (COO), and staff members from Human Resources. For health centers that are strongly committed to launching, the team coach is typically an NP or PA that will serve as the Clinical Program Director.
The learning collaborative is led by two expert faculty members, CHCI’s Postgraduate NP Residency Program Director and the Executive Director of the Consortium for Advanced Practice Providers, who served as CHCI’s Postgraduate NP Residency Program Director from 2009 to 2019, as well as launched the NTTAP on Clinical Workforce Development in 2015 with Margaret Flinter. The expert faculty, along with experts specific to learning session topics from other health centers and/or academic institutions, led six 90-minute learning sessions. See Table 2 for a complete list of learning session topics. The learning collaborative also included bi-weekly 60-minute intensive coaching calls for health center team coaches, which allowed the expert faculty to discuss health center progress, answer questions around barriers, review deliverable drafts by the participating organizations, and/or expand upon learning session topics as needed based on the cohort’s progression through the curriculum. Upon request, expert faculty met one-on-one with health center teams to discuss any barriers or roadblocks in more depth that they were struggling to overcome.
CHCI’s NTTAP Postgraduate NP and/or PA Training Programs Learning Collaborative Overview.

Although the literature describes the impact of postgraduate residency training programs on new NPs and PAs during early practice transition, this study was the first to explore the facilitators and barriers of launching a program in a community health center. Previous research studies reported on the value of Postgraduate NP and/or PA Residency or Fellowship Program, 9 as well as the sustained impact of the residency program. 7 This study explored the following research questions: (1) How many health centers from the seven cohorts of the Postgraduate NP and/or PA Training Programs Learning Collaborative successfully launched a program?; (2) What is the implementation process of launching a Postgraduate NP and/or PA Residency or Fellowship Program in a health center?; and (3) What can we learn from those that were successful and unsuccessful in launching a Postgraduate NP and/or PA Residency or Fellowship Program? Ultimately, this study aimed to support health centers in their journey towards building and launching a Postgraduate NP and/or PA Training Program.
Methodology
This mixed-methods study was approved by CHCI’s Institutional Review Board (IRB ID: 1219). Informed consent to participate was obtained at the beginning of the survey and interview with the following statement: “This survey is confidential and will only be reviewed by the research team. Names and organizations will not be published. If at any point you feel the need to withdraw your survey response, please reach out to the researchers.” For the interviews, participants also signed a consent for participation.
The confidential survey was created in Qualtrics, a web-based survey tool, and was sent via email using with an anonymous survey link. The survey was developed through a literature review and reviewed by subject matter experts to ensure clarity, relevance, and comprehensiveness. The survey was administered to the 78 health centers that participated in the CHCI’s NTTAP Postgraduate NP and/or PA Training Programs Learning Collaborative from 2016 to 2023. The survey was distributed to all 78 health centers on March 4th, 2024 and the survey closed on April 19th, 2024. See Table 3 for the participating health centers per cohort. On average, 44.56% of the cohort completed the survey.
Participating Health Centers Per Cohort.

Survey questions included health center and participant characteristics (e.g., organization location, survey respondent name and title, learning collaborative cohort), and the status of their Postgraduate NP and/or PA Residency or Fellowship Program, including:
Yes, and have active Postgraduate NP and/or PA Residency or Fellowship Program.
Yes, but the Postgraduate NP and/or PA Residency or Fellowship Program is now inactive.
In the process of launching a Postgraduate NP and/or PA Residency or Fellowship Program.
No, have not launched a Postgraduate NP and/or PA Residency or Fellowship Program.
Unsure.
For those that had launched a program (active and inactive), the survey respondent was asked to rank the facilitators for launching their Postgraduate NP and/or PA Residency or Fellowship Program. For those that were in the process of launching a program or have not launched a program, the survey respondent was asked to rank the barriers for launching their Postgraduate NP and/or PA Residency or Fellowship Program. If the survey respondent selected “unsure,” the survey ended. See Appendix A for a full list of survey questions.
At the end of the survey, participants were invited to participate in an interview with the following question: “We hope to conduct interviews with a number of individuals who have completed this survey. May we contact you to discuss participation? If yes, please include your email.” Those who indicated interest in an interview by providing their email were contacted to arrange an interview date and time, as well as sign a consent document. Interviews were conducted over a secure Zoom link by the two main researchers. These structured interviews were aimed to gain a deeper understanding of the facilitators and barriers to launching their Postgraduate NP and/or PA Residency or Fellowship Program. See Appendix B for a full list of interview questions.
Data Analysis
Survey data on facilitators and barriers to launching a program were analyzed using Friedman’s test to assess differences in their rankings. 10 This test was selected due to the nature of the survey responses, where participants ranked multiple factors, resulting in dependent (paired) data. Additionally, the data did not meet the normality assumption, making a parametric alternative, such as repeated-measures ANOVA, inappropriate. While Friedman’s test effectively identifies differences in rankings, it does not account for potential confounding variables, such as institutional differences or respondent characteristics. To pinpoint specific differences between facilitators and barriers, Wilcoxon signed-rank tests were conducted as post hoc analyses. A Bonferroni correction was applied to control for multiple comparisons and minimize the risk of Type I error. Data were analyzed using SPSS Version 27 (IBM, Armonk, NY, USA).
To address potential non-response bias, qualitative data from interviews were incorporated to provide deeper insights into potential gaps in the survey findings. Interview data were transcribed via Zoom and then reviewed by Meaghan Angers for initial impressions and later assigned codes to identify major themes using a predominantly deductive approach with additional themes emerging inductively. 11 Final themes were determined through team consensus.
Results
Survey
Of the 78 health centers that participated in CHCI’s NTTAP Postgraduate NP and/or PA Training Programs Learning Collaborative since 2016, 47.44% (n = 37) responded to the survey. Health centers were located throughout the U.S. with a majority from HRSA Region 9 (24.32%) and Region 1 (16.22%). See Table 4 for details on the HRSA Regional Operations Locations. 12 As for the individuals that completed the survey, the majority (43.24%) served in a leadership role at their health center. Finally, the majority of respondents were from the 2022 to 2023 learning collaborative cohort (35.13%). See Table 4 for participant characteristics.
Participant Characteristics.

Facilitators to Launching a Postgraduate NP and/or PA Residency or Fellowship Program
Of the 37 survey respondents, 48.65% (n = 18) have an active Postgraduate NP and/or PA Residency or Fellowship Program, while 2.70% (n = 1) have an inactive program. These survey respondents were asked to order the following facilitators from most influential (1) to least influential (7): leadership support, clinical support (e.g., preceptors, mentors), administrative support, dedicated time for planning and implementation, demonstrated financial benefit and return on investment, dedicated and motivated staff members, and existing student or postgraduate training programs at your health center.
For their most influential facilitator to launching their program, survey respondents ranked leadership support as the most influential facilitator to launching their program, followed by clinical support (e.g., preceptors, mentors) as their second most influential facilitator. Survey respondents expressed that existing student or postgraduate training programs at your health center was the least influential facilitator to launching their program. See Table 5 for the complete ranking of facilitators from most to least influential. Statistically significant differences were found in launching a program depending on the ranking order of the facilitators, X2(6) = 61.64, P < .001. Further details on these differences are available in Appendix C (Table C1). Post hoc analysis using Wilcoxon signed-rank tests, with a Bonferroni correction setting the significance level at P < .002, showed statistically significant differences in ranking for certain facilitator comparisons. For example, leadership support was ranked significantly higher than administrative support (Z = −3.75, P < .001).
Facilitators to Launching a Postgraduate NP and/or PA Residency or Fellowship Program (n = 18). a

X2(6) = 61.64, P < .001.
One respondent did not rank the facilitators of their program.
Barriers to Launching a Postgraduate NP and/or PA Residency or Fellowship Program
Of the 37 survey respondents, 40.54% (n = 15) have not launched a Postgraduate NP and/or PA Residency or Fellowship Program, while 8.11% (n = 3) are in the process of launching a Postgraduate NP and/or PA Residency or Fellowship Program. These survey respondents were asked to order the following barriers from most influential (1) to least influential (10): lack of financial resources, no leadership buy-in, lack of administrative support, lack of clinical staff to support residents (e.g., preceptors, mentors), limited dedicated time for planning and implementation, competing priorities, limited clinical space, recruitment of residents, staff turnover, and the Coronavirus Disease 2019 (COVID-19) pandemic.
For their most influential barrier to launching their program, respondents ranked lack of financial resources as the most influential barrier to launching their program, followed by competing priorities as their second most influential barrier. Survey respondents expressed that recruitment of residents was the least influential facilitator to launching their program. See Table 6 for the complete ranking of barriers from most to least influential. Statistically significant differences were found in launching a program depending on the ranking order of the barriers, X2(9) = 70.55, P < .001. Further details on these differences are available in Appendix D (Table D1). Post hoc analysis using Wilcoxon signed-rank tests, with a Bonferroni correction setting the significance level at P < .001, showed statistically significant differences between certain barriers. For instance, lack of leadership buy-in was ranked significantly lower than lack of financial resources (Z = −3.75, P < .001).
Barriers to Launching a Postgraduate NP and/or PA Residency or Fellowship Program (n = 18).
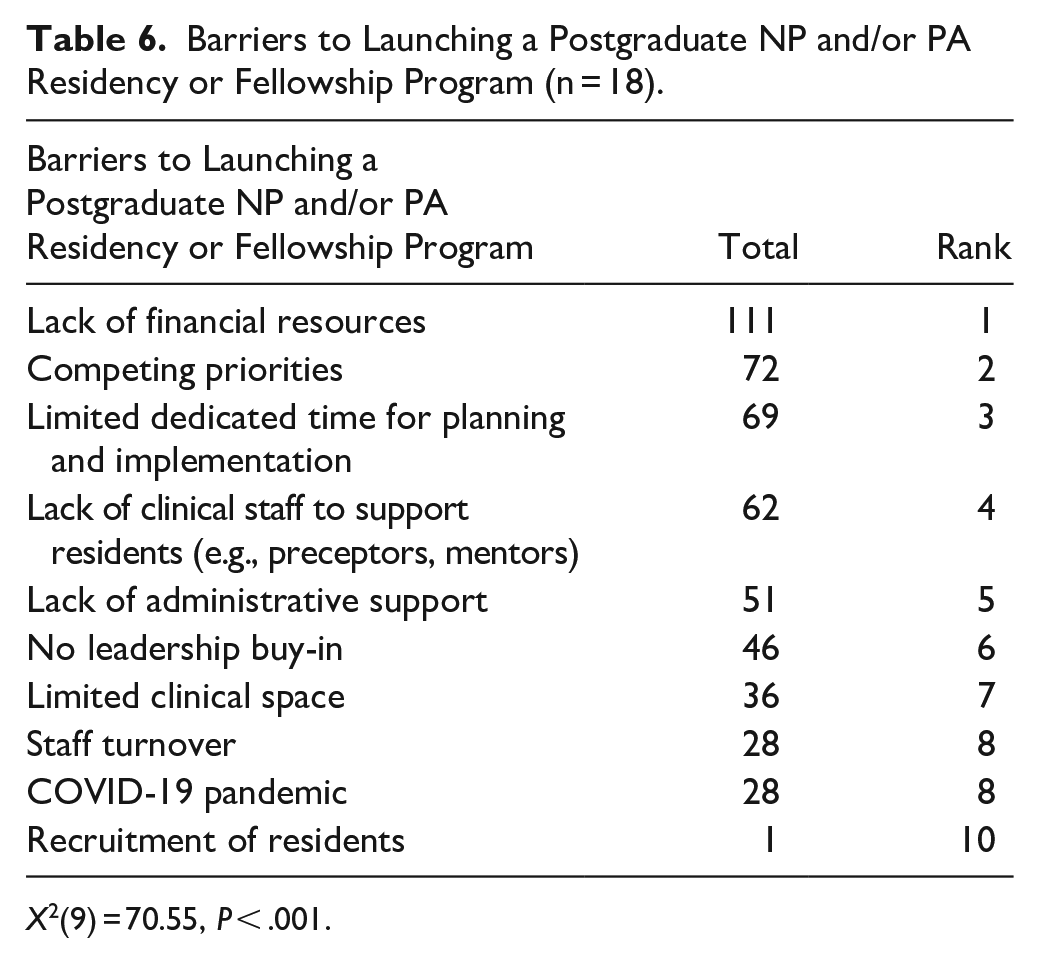
X2(9) = 70.55, P < .001.
Interviews
Of the 37 health centers that responded to the survey, 75.68% (28) agreed to be contacted to be interviewed. Ultimately, 37.84% (n = 15) of the 37 health centers completed interviews with the research team. Of the 15 completed interviews, 66.67% (n = 10) had launched a program, while 33.33% (n = 5) had not launched a program. Analysis of the interviews resulted in the below themes:
Those with a launched program echoed the sentiments of the survey responses that without leadership support, they could not have launched their program. They did face financial barriers and lacked clinical support, but because of the strong leadership support at their health center, they were able to overcome those barriers and launch the program. a. “Always leadership support on the concept, but when it came to financial and support needed was challenging. Until we had a senior leader that worked at an FQHC with a residency and participated as faculty, we were actually able to get going.” b. “No barriers to launching because we had full leadership support. There were no obstacles, even with finding preceptors and mentors—they are so used to rotations, new hires, and students.”
Those with a launched program expressed they faced financial barriers, but were able to secure grant funding.
a. “I think the one barrier we would have perceived would have been financial, but we were awarded the HRSA grant and that became not a barrier.” b. “Our program did start with a HRSA grant so the grant funding allowed for financial breathing room.”
Those with a launched program expressed mission-driven workforce pathway planning was a facilitator.
a. “There was a period time with new graduates and 50% of them ended up leaving after the first year—so recognized we needed to invest more in the new graduate providers.” b. “Need to have a more trained family NP workforce—definitely think that was the main driver.” c. “Need for residency to promote that workforce.” d. “The people who were motivated to do it and the real reason was several new graduate NPs were hired and only lasted 4 to 5 months because it was so overwhelming to be in full scope primary care and did not get the support to stay on and succeed. The residency was created in an effort for a longer onboarding practice and support first year of practice so NPs could stay with our organization.” e. “To be honest, another driver is we are continually wanting to hire a diverse group of providers to reflect community and Medical Directors not wanting to hire a new graduate that has not worked with us, and that was getting in the way of hiring a diverse group.” f. “A lot of turnover and attrition with providers, especially new graduates. They come for loan repayment and leave. This drove us to find the training they need and help us to train them to stay for the long haul.” g. “Looking to retain primary care providers—new primary care providers outside of school had a high turnover.” h. “Recognition that the broad scope of comprehensive primary care was overwhelming for new graduates and people were quickly leaving primary care.”
Those without a launched program echoed the sentiments of the survey responses that barriers of finances, time, and clinical support for preceptors and mentors prevented their organization from launching a Postgraduate NP and/or PA Training Program. They also expressed barriers of limited clinical space.
a. “Finances—it has been difficult to secure funding and budgeting.” b. “We have above average leadership and of all the barriers that I can think of the main ones are time and money.” c. “Space is limited with the brick and mortar clinic.” d. “Space issues and capacity for preceptors/mentors. You can create everything, but need someone that is engaged in the program.” e. “Space allocation is another—initially when we started we procure another spot, but already lost clinical space there.”
Those without a launched a program expressed the learning collaborative set them up for success to launch a program. a. “It was really great to see a broad overview of everything we would need and starting at foundation and building up.” b. “Just the availability of support from the training program.” c. “All of the print materials that would help develop and implement a program.” d. “If I were to make this from scratch, it just wouldn’t have happened, so having a framework from you guys that I can develop and tweak to fit us has been just perfect for my leadership style and for our organization and because we know we want. . . . .knowing that your program is along the guidelines for accreditation helps a lot with that.”
Discussion
The intention of the HRSA-funded Postgraduate NP and/or PA Training Programs Learning Collaborative hosted by CHCI’s NTTAP on Clinical Workforce Development is to provide free training and technical assistance to support federally funded health centers and look-alikes across the country in their journey to launch a Postgraduate NP and/or PA Training Program. By evaluating seven completed cohorts of the learning collaborative, this study found several key findings that would support health centers and look-alikes in their journey towards program implementation.
Facilitators to launching a program is heavily reliant on (1) leadership support, (2) clinical support (e.g., preceptors, mentors), and (3) dedicated time for planning and implementation. For these findings, there is a significant difference between the first and second facilitator. Between leadership support and clinical support (e.g., preceptors, mentors), there was a 26 point difference, thus showing the integral need for leadership support. Additionally, a majority of interviews with launched programs revealed a facilitator that was not a part of the survey, a commitment to mission-driven workforce pathway planning. Interviewees revealed that prior to the learning collaborative opportunity, their health center had made a commitment to develop a training program to train new NPs and/or PAs and decrease burnout.
The least influential facilitators were (1) administrative support, (2) demonstrated financial benefits and return on investment, and (3) existing student or postgraduate training programs. Interestingly, having an existing student or postgraduate training programs at the health center was the least influential facilitator for supporting a launch of a Postgraduate NP and/or PA Training Program. In fact, 47% of the launched programs (n = 17) did not directly sponsor other health professions training programs prior to the launch of their Postgraduate NP and/or PA Training Program.
Furthermore, some interviews with launched Postgraduate NP and/or PA Training Programs revealed their health center had grant funding to support the launch of their program; therefore, their health center did not have the additional financial strain due to loss revenue in patient visits. Grant funding significantly reduced the barrier of demonstrated financial benefit and return on investment. For programs that were in the progress of launching, they did not launch due to significant barriers around financial support, but they were still in the pursuit of launching due to a strong leadership and organizational support for the program. For those that had not launched a program and did not have plans to launch, they saw the value in the program to train the next generation, but did not have the organization’s financial support for a program.
On the other hand, barriers to launching a program included (1) lack of financial resources, (2) competing priorities, and (3) limited dedicated time for planning and implementation. For these findings, there was a significant difference between the first and second barrier. Between lack of financial resources and competing priorities, there was a 39 point difference, thus showing the clear number one barrier and integral need for financial resources. The interviews also echoed the sentiments of financial barriers preventing the launching of their Postgraduate NP and/or PA Training Program, along with barriers of time, clinical support, and space. Interestingly, we saw that the third most important facilitator as dedicated time for planning and implementation, therefore, validating the importance of having time to plan and implement the program.
For some participating health centers, the COVID-19 Pandemic was a major barrier. Although it is one of the bottom three barriers, it is important to recognize that the COVID-19 pandemic halted many health centers from launching a Postgraduate NP and/or PA Training Program. When the COVID-19 Pandemic began in March 2020, CHCI’s NTTAP was in the course of wrapping up the 2019 to 2020 learning collaborative cohort. Additionally, CHCI’s NTTAP continued to host the learning collaborative for the 2020 to 2021 cohort. For those learning collaborative cohorts, health centers participated with the intention of launching a program, but due to the COVID-19 pandemic, their priorities and resources were shifted.
Through the HRSA-funded Postgraduate NP and/or PA Training Programs Learning Collaborative hosted by CHCI’s NTTAP, dozens of federally funded health centers and look-alikes have successfully launched a Postgraduate NP and/or PA Training Program. Among the 18 health centers that completed the survey and have launched a program, the researchers learned that 215 residents or fellows have graduated from a Postgraduate NP and/or PA Training Program created due to the learning collaborative opportunity. Of those 215 graduates, 86 (40%) have stayed on to be employees at the health center. These findings highlight the significant impact of the learning collaborative in equipping health centers with the foundational knowledge and resources needed to establish their own training program, ultimately strengthening their primary care workforce and improving care for their patient populations.
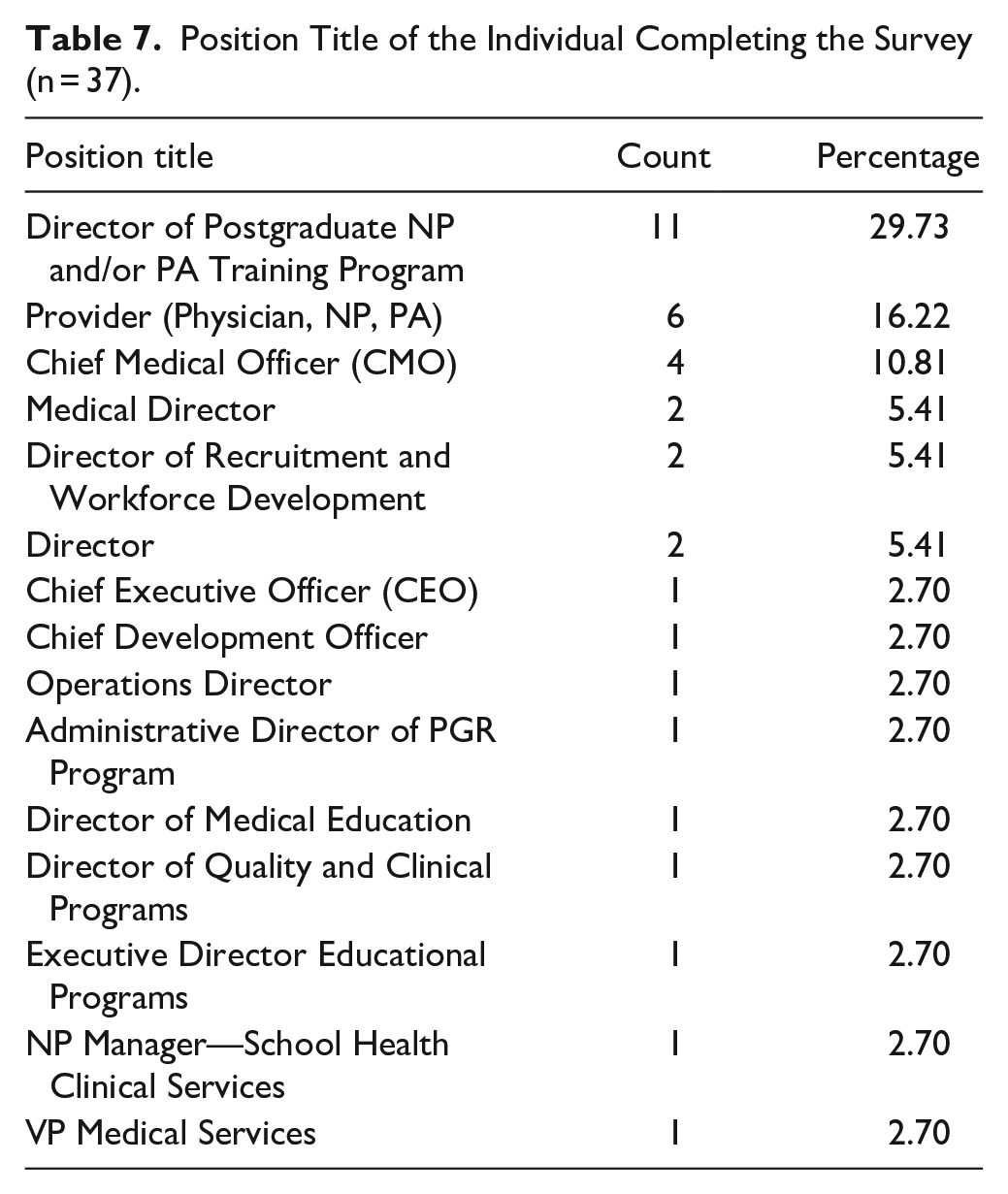
Among survey respondents, the most common position held was the Director of the Postgraduate NP and/or PA Training Program, followed by Provider (Physician, NP, PA), and Chief Medical Officer (CMO). While Table 4 highlights that leadership roles made up the majority of respondents (43.24%), a more detailed breakdown in Table 7 reveals the majority of individuals were the Director of the Postgraduate NP and/or PA Training Program (29.93%). This demonstrates the robust data received from both leaders at the health center, as well as those directly affiliated with the Postgraduate NP and/or PA Training Program, providing a well-rounded perspective on program development and execution.
Position Title of the Individual Completing the Survey (n = 37).
Participation from the seven completed cohorts of the Postgraduate NP and/or PA Training Programs Learning Collaborative was varied, but responses were received from every completed cohort. The largest response rate was from the 2022 to 2023 cohort with 71.43% (n = 10) of the 14 health centers responding to the survey. Considering this was the most recent cohort of the learning collaborative, the contact information was up-to-date and the survey respondent was familiar with the learning collaborative and the researcher, Meaghan Angers. In comparison, the lowest response rate was from the 2018 to 2019 cohort with 8.11% (n = 3) of the 12 health centers responding to the survey. Those from earlier cohorts may have not responded to the survey as they may have left their health center, forgotten about the learning collaborative opportunity, and/or was not familiar with the researcher’s contact information. Interestingly, the 2016 to 2017 cohort had a high response rate with 54.55% (n = 6) of the 11 participating health centers responding.
Conclusions
To our knowledge, this was the first study to explore the facilitators and barriers of launching a Postgraduate NP and/or PA Residency or Fellowship Program in a community health center. The findings highlight that strong leadership support was the most significant facilitator in successfully launching a program, while lack of financial resources was the most significant barrier. Additionally, grant funding and mission-driven workforce pathway planning emerged as influential facilitators. Through the HRSA-funded Postgraduate NP and/or PA Training Programs Learning Collaborative hosted by CHCI’s NTTAP, dozens of federally funded health centers and look-alikes have received free training and technical assistance to launch their program, and as a result have trained 215 residents or fellows, with 86 employed within the health center.
By evaluating the seven completed cohorts of the Postgraduate NP and/or PA Training Programs Learning Collaborative, this study provides health centers and look-alikes with valuable insights and guidance into the facilitators and barriers that influence program implementation. The findings of this research study may also inform HRSA on policies, programs, and funding. By investing in Postgraduate NP and/or PA Training Programs, community health centers can strengthen their workforce and improve access to high-quality primary care for underserved populations.
Footnotes
Appendix A: Qualtrics Survey
Appendix B: Interview Questions
Appendix C
Post Hoc Wilcoxon Signed-Rank Test Results Comparing Facilitator Rankings for Program Launch.

| Facilitator comparison | Z | Asymp. sig. (2-tailed) |
|---|---|---|
| Clinical support (e.g., preceptors, mentors)—leadership Support | −3.035 | .002 |
| Administrative support—leadership Support | −3.751 | <.001 |
| Dedicated time for planning and implementation—leadership Support | −3.433 | .001 |
| Demonstrated financial benefit and return on investment—leadership Support | −3.709 | <.001 |
| Dedicated and motivated staff members—leadership Support | −2.671 | .008 |
| Existing student or postgraduate training programs at your health center—leadership Support | −3.804 | <.001 |
| Administrative support—clinical support (e.g., preceptors, mentors) | −2.166 | .030 |
| Dedicated time for planning and implementation—clinical support (e.g., preceptors, mentors) | −1.237 | .216 |
| Demonstrated financial benefit and return on investment—clinical support (e.g., preceptors, mentors) | −3.145 | .002 |
| Dedicated and motivated staff members—clinical support (e.g., preceptors, mentors) | −0.942 | .346 |
| Existing student or postgraduate training programs at your health center—clinical support (e.g., preceptors, mentors) | −3.755 | <.001 |
| Dedicated time for planning and implementation—administrative support | −1.132 | .258 |
| Demonstrated financial benefit and return on investment—administrative support | −1.696 | .090 |
| Dedicated and motivated staff members—administrative support | −0.550 | .583 |
| Existing student or postgraduate training programs at your health center—administrative support | −3.660 | <.001 |
| Demonstrated financial benefit and return on investment—dedicated time for planning and implementation | −2.329 | .020 |
| Dedicated and motivated staff members—dedicated time for planning and implementation | −0.286 | .775 |
| Existing student or postgraduate training programs at your health center—dedicated time for planning and implementation | −3.753 | <.001 |
| Dedicated and motivated staff members—demonstrated financial benefit and return on investment | −1.494 | .135 |
| Existing student or postgraduate training programs at your health center—demonstrated financial benefit and return on investment | −3.088 | .002 |
| Existing student or postgraduate training programs at your health center—dedicated and motivated staff members | −3.742 | <.001 |
Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied, resulting in a significance level set at P < .002.
Appendix D
Post Hoc Wilcoxon Signed-Rank Test Results Comparing Barrier Rankings for Program Launch.

| Barrier comparison | Z | Asymp. sig. (2-tailed) |
|---|---|---|
| No leadership buy-in—lack of financial resources | −3.753 | <.001 |
| Lack of administrative support—lack of financial resources | −3.391 | .001 |
| Lack of clinical staff to support residents (e.g., preceptors, mentors)—lack of financial resources | −3.042 | .002 |
| Limited dedicated time for planning and implementation—lack of financial resources | −2.999 | .003 |
| Competing priorities—lack of financial resources | −2.489 | .013 |
| Limited clinical space—lack of financial resources | −3.591 | <.001 |
| Recruitment of residents—lack of financial resources | −3.749 | <.001 |
| Staff turnover—lack of financial resources | −3.628 | <.001 |
| COVID-19 Pandemic—lack of financial resources | −3.315 | .001 |
| Lack of administrative support—no leadership buy-in | −1.076 | .282 |
| Lack of clinical staff to support residents (e.g., preceptors, mentors)—no leadership buy-in | −1.072 | .284 |
| Limited dedicated time for planning and implementation—no leadership buy-in | −1.706 | .088 |
| Competing priorities—no leadership buy-in | −1.615 | .106 |
| Limited clinical space—no leadership buy-in | −0.394 | .693 |
| Recruitment of residents—no leadership buy-in | −3.128 | .002 |
| Staff turnover—no leadership buy-in | −1.049 | .294 |
| COVID-19 Pandemic—no leadership buy-in | −1.508 | .132 |
| Lack of clinical staff to support residents (e.g., preceptors, mentors)—lack of administrative support | −0.969 | .333 |
| Limited dedicated time for planning and implementation—lack of administrative support | −1.340 | .180 |
| Competing priorities—lack of administrative support | −1.273 | .203 |
| Limited clinical space—lack of administrative support | −1.367 | .172 |
| Recruitment of residents—lack of administrative support | −3.768 | <.001 |
| Staff turnover—lack of administrative support | −1.819 | .069 |
| COVID-19 Pandemic—lack of administrative support | −1.783 | .075 |
| Limited dedicated time for planning and implementation—lack of clinical staff to support residents (e.g., preceptors, mentors) | −0.840 | .401 |
| Competing priorities—lack of clinical staff to support residents (e.g., preceptors, mentors) | −0.765 | .444 |
| Limited clinical space—lack of clinical staff to support residents (e.g., preceptors, mentors) | −2.404 | .016 |
| Recruitment of residents—lack of clinical staff to support residents (e.g., preceptors, mentors) | −3.763 | <.001 |
| Staff turnover—lack of clinical staff to support residents (e.g., preceptors, mentors) | −2.584 | <.001 |
| COVID-19 Pandemic—lack of clinical staff to support residents (e.g., preceptors, mentors) | −2.495 | .013 |
| Competing priorities—limited dedicated time for planning and implementation | −0.556 | .578 |
| Limited clinical space—limited dedicated time for planning and implementation | −2.318 | .020 |
| Recruitment of residents—limited dedicated time for planning and implementation | −3.778 | <.001 |
| Staff turnover—limited dedicated time for planning and implementation | −3.011 | .003 |
| COVID-19 Pandemic—limited dedicated time for planning and implementation | −2.667 | .008 |
| Limited clinical space—competing priorities | −2.075 | .038 |
| Recruitment of residents—competing priorities | −3.754 | <.001 |
| Staff turnover—competing priorities | −3.530 | <.001 |
| COVID-19 Pandemic—competing priorities | −2.934 | .003 |
| Recruitment of residents—limited clinical space | −3.568 | <.001 |
| Staff turnover—limited clinical space | −1.076 | .282 |
| COVID-19 Pandemic—limited clinical space | −1.510 | .131 |
| Staff turnover—recruitment of residents | −2.180 | .029 |
| COVID-19 Pandemic—recruitment of residents | −0.264 | .792 |
| COVID-19 Pandemic—staff turnover | −1.292 | .196 |
Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied, resulting in a significance level set at P < .001.
Acknowledgements
The authors of this article would like to acknowledge and thank all experts and participants for their valuable contributions leading to the successful completion of this research study.
Consent to Participate
Consent to participate was obtained at the beginning of the survey and interview with the following statement: “This survey is confidential and will only be reviewed by the research team. Names and organizations will not be published. If at any point you feel the need to withdraw your survey response, please reach out to the researchers.” In email communication, participants were told: “If you are willing to participate, please take 5 to 10 min to complete the following survey by Monday April 1st.” For the interviews, participants also signed a consent for participation.
Declarations Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Community Health Center, Inc. Institutional Review Board (IRB ID: 1219).
Data Availability
Data is provided within the manuscript and can be made available upon reasonable request.