
Abstract
In March 2020, the worldwide outbreak of COVID-19 led to the declaration of a global pandemic by the World Health Organization. As a result of the rapid spread and severity of the disease, health services experienced unprecedented pressure on acute hospital systems. Many strategies were implemented to both curb the spread of the disease and manage its impact on health services. Field hospitals were one such measure, deployed as surge capacity facilities to provide solutions to patient flow challenges due to spikes in hospital admissions associated with COVID-19. In Ireland, a temporary Intermediate Care Facility (ICF) was established on the grounds of a university campus in response to the pandemic. Designed as a step-down interprofessional care facility for local acute hospitals, this service had capacity for 84 patients and was operational for 4 months. A qualitative study was conducted to explore patient’s experience of receiving care in the ICF. Thirteen patients participated in semi-structured interviews post-discharge. Following inductive thematic analysis, 3 main themes emerged: the ICF as a (1) Novel healthcare setting, (2) Person-centered care and (3) Psycho-social climate. This study describes patients’ experience of care in the ICF during the COVID-19 pandemic which may inform future policies and practice initiatives targeting patient care and patient outcomes, as well as pandemic preparedness and response plans.
Keywords
In March 2020, the World Health Organization (WHO) declared Coronavirus disease (COVID-19) a global pandemic. 1 This highly transmissible infectious disease caused by the SARS-CoV-2 virus was observed to typically result in mild to moderate illness for most people who contracted it. Older people and those with underlying health conditions were identified to be at greater risk of developing acute illness, however, it was acknowledged that anyone at any age could develop serious illness or die due to the virus. 2 Throughout the initial stages of the pandemic, many countries experienced ‘waves’ of significant increases in infection rates which led to spikes in hospital admissions and elevated death rates. 3
The unprecedented nature of COVID-19 led to unforeseeable strain placed on local health care services, which warranted an immediate and coordinated response. The first disease outbreak was detected in early 2020 in Wuhan, China, where field hospitals were implemented quickly in response to the need for surge capacity. 4 Field hospitals by definition are mobile, self-sufficient facilities developed rapidly in response to a health-related emergency to provide additional resources.5,6 Many countries followed suit from the experiences in Wuhan and established field hospitals to cope with the increase in demand for healthcare associated with the virus. Such facilities were often developed within locations that lacked any preceding health service provision infrastructure such as convention/exposition centers and concert halls7-9 and the army or national guard were often involved in their rapid establishment.10,11 Examples include the Nightingale Hospital London in England, 12 the Javits New York Medical Station in the USA, 8 the Officine Grandi Riparazioni Temporary Hospital in Italy 7 and the Fairground Exhibition Center in Spain. 9 Their period of operation varied across sites from weeks to months depending on local requirements and resourcing.8,13 The patient profile also differed, with some tailoring their service provision to COVID-19 patients only, while others admitted both patients with COVID-19 illness and those without COVID-19.11,13
The Intermediate Care Facility
This research focuses on a field hospital established in the Mid-West region of the Republic of Ireland arising as part of a joint COVID-19 pandemic response initiative between the local hospital network and its academic partner, the University of Limerick. 14 The field hospital known as the Intermediate Care Facility (ICF) was set up in the sports arena on the grounds of the university. An ICF offers a variety of services designed to: promote faster recovery from illness, prevent unnecessary acute hospital admissions and early entry into long-term care, support timely hospital discharge and maximize independent living. 15 The ICF in this instance supported timely hospital discharge by providing interprofessional care to non-COVID-19 patients and post-COVID-19 patients who were no longer infectious. It was developed in response to an urgent requirement for additional healthcare capacity during the COVID-19 pandemic. This region had a lower baseline bed capacity compared to national rates and limited access to private hospital facilities relative to other regions in Ireland. The building location was chosen due to its strategic proximity to the acute hospital it was serving, and the availability of essential infrastructure to support a large-scale healthcare operation. Additionally, the university location provided opportunities to leverage the university’s resources including healthcare and research expertise, healthcare staff and students. The facility was rapidly established with support from the Irish Defense Forces who assisted in infrastructure set up (Table 1).
Chronology of Emergence and Closure of the ICF.

Operational from June 2020 to October 2020, the field hospital served as a solution to regional patient flow and crowding challenges. 16 The facility was laid out in partitioned wards with bays of 16 partitioned beds (8 at each side) designed to optimize patient care and infection control. There were 4 enclosed rooms for patients requiring isolation or additional privacy. In addition, typical ward support accommodation included clean and dirty utilities, pharmacy, pantry, clinical treatment areas and 2 recreation areas were available. It had capacity for 84 beds and treated a total of 188 patients. A floor plan of the ICF is outlined in Appendix 1.
The ICF functioned as a fully staffed and equipped Model 1 hospital that provided comprehensive bed-based, intermediate care for non-Covid-19 patients. In Ireland, a Model 1 hospital is a community or district hospital. The ICF differed from traditional hospitals in several keyways. Unlike acute care hospitals, which provide emergency and intensive care services, the ICF focused on integrated services for patients requiring short-term sub-acute care, rehabilitation, convalescence, respite and palliative care. Healthcare delivery in the ICF was informed by existing intermediate care guidance 15 and adapted to the COVID-19 context. These models are designed to support patients who no longer require acute hospital care but continue to need medical and rehabilitative services before they can be safely and independently discharged home or to long-term care placement. Staff, students and educators were re-deployed on site, including the disciplines of dietetics, medical social work, medicine, nursing, occupational therapy, pharmacy, physiotherapy and speech and language therapy. A patient advocacy liaison service (PALS) was also onsite. PALS is a free, independent and confidential advocacy service for patients in public acute hospitals in Ireland. In the ICF, PALS served as the main contact between patients, their families, carers and the facility ensuring that the patient voice was heard, and their needs were met. Patients transferred to the ICF received a range of coordinated rehabilitative services aimed at improving patient outcomes and satisfaction, maximizing recovery, quality of life and independence in preparation for discharge with a longer-term aim of readmission reduction. Within Ireland 2 other COVID-19 contingency facilities were developed for varying patient groups, however, there is no published information on how these facilitates were operationalized.
The ICF maintained a strong focus on interprofessional collaboration, education and practice from the site’s initial conception through to its operationalization. The global health crisis has since highlighted the central role of interprofessional working in pandemic management. 17 Interprofessional education occurs when students from differing healthcare professions work together to learn about, from and with each other. 18 Similarly, interprofessional collaboration occurs when healthcare professionals from various backgrounds work together to deliver high quality care.18,19
The importance of researching patients’ experience of health care, including their expectations and level of satisfaction, is well recognized.20-22 Patient satisfaction can serve as an outcome of patient experience and may indicate whether the service they received matched their expectations and needs 22 and may also serve as a useful means of ensuring accountability amongst health systems and policymakers. 22 Due to the novel nature of the COVID-19 pandemic and the field hospital setting, the aim of this study was therefore to explore patient experiences of receiving interprofessional care in an ICF setting during the COVID-19 pandemic. It is anticipated that findings from the current study may inform interprofessional working both in the acute and post-acute setting, future field hospital or ICF care and inform pandemic preparedness and response plans.
Materials and Methods
Study Design
A qualitative descriptive methodology was used as it allows for an exploratory investigation of novel situations and is thus well suited to pandemic-related studies. 23 It is a valuable methodological approach used to uncover the ‘who, what and where’ of novel events 24 and has been identified as particularly suitable for exploring patient experiences. 25 The Consolidated Criteria for Reporting Qualitative Research (COREQ) tool was used to ensure the research was reported in line with qualitative principles. 26
Author Positionality
The authors are part of an interprofessional research team consisting of faculty, staff from a local university and clinical staff and management from a local university hospital. During regular team meetings the authors reflected on their positionality and how it informed their perspective on the various stages of the research. At the time of data collection, the lead author was a clinical staff member in the ICF hence data was collected by a research assistant who had no previous relationship with participants and was employed by the faculty. To reduce the potential effects of social desirability, 1 author conducted data collection while the remaining authors limited their roles to study design, recruitment, secondary analysis and manuscript development.
Ethical Approval and Participant Recruitment
Ethical approval was obtained from the Irish Health Service Executive Research Ethics Committee (reference number 092/2020). The lead author contacted potential participants by letter and provided participants with an information leaflet written in plain language as well as a consent form. Participants were given time to consider their participation and were provided with an opportunity to ask questions prior to commencing the interview. Participation was voluntary and participants were fully informed of the study’s purpose prior to engaging in the research. Consent was gained by all participants prior to participation and could be withdrawn at any time throughout the research process. All participants provided written informed consent prior to commencement of an interview. Pseudonyms were assigned to all participants to ensure anonymity.
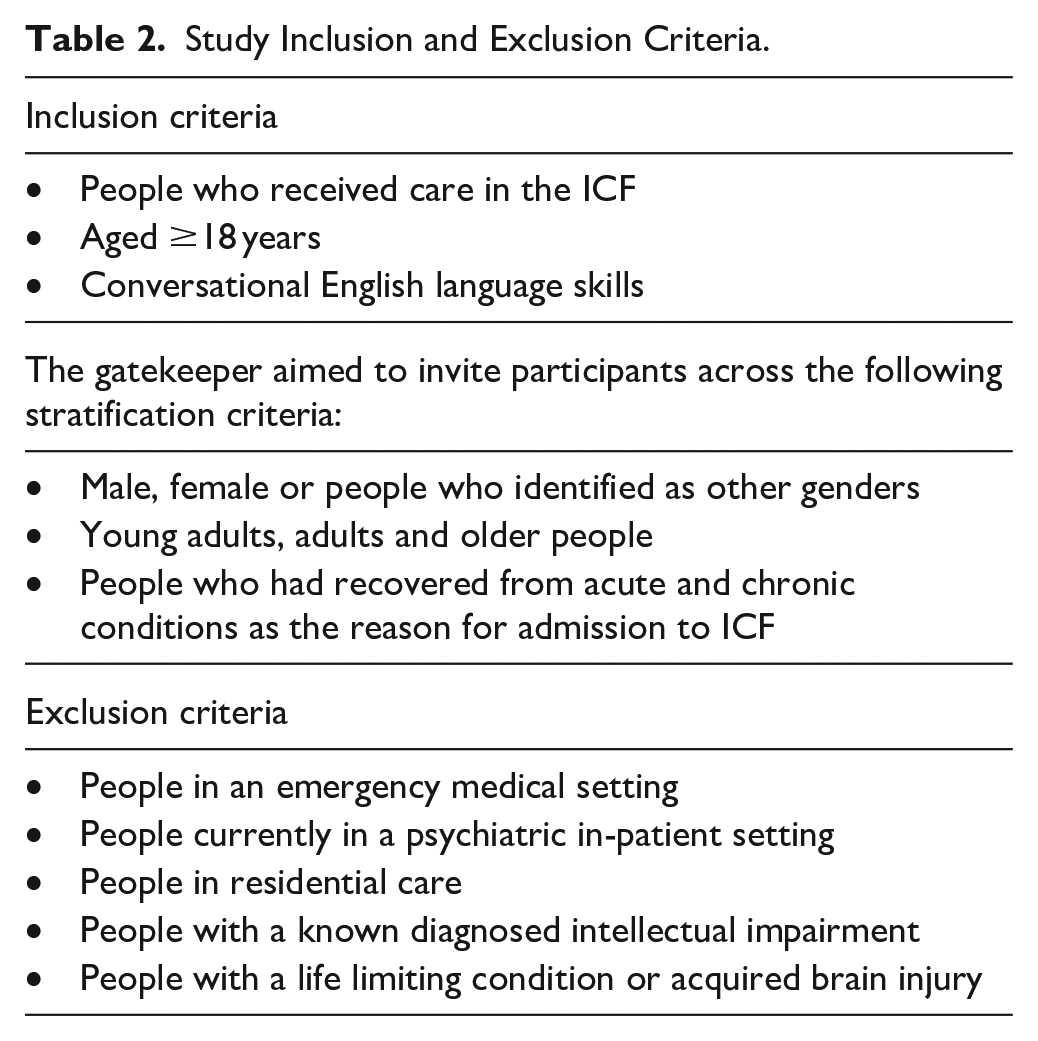
Consistent with qualitative descriptive research design, purposive sampling was adapted initially for the recruitment of participants followed by snowball sampling methods with a focus on maximum variation to select a range of participants who met the inclusion and exclusion criteria (see Table 2). Purposive sampling is a participant identification and recruitment technique which is commonly adopted in qualitative research as it involves the selection of participants most knowledgeable about the research topic. 27 Snowball sampling methods are often used in conjunction with other sampling methods such as purposive sampling to increase participant numbers in difficult to access or limited-sized populations. 28
Study Inclusion and Exclusion Criteria.
Recruitment of 12 participants occurred between November 2020 and February 2021. After the completion of 12 interviews during the recruitment period, it was identified that qualitative data saturation had been achieved, which was later confirmed by the 13th and final interview.
Qualitative Procedures
A semi-structured interview guide was developed with 11 open-ended questions designed to elicit participants’ experience of being a patient in the ICF (see Appendix 2). Questions included ‘What was your initial impression of the facility?’ and ‘Can you tell me about the staff you met during your stay in the ICF?’ A script was prepared to be used at the beginning of each interview clarifying the study’s purpose, confidentiality agreement and provide an opportunity for participants’ to ask questions. The interview guide was developed with reference to the literature and refined by the research team which consisted of representation from practice and academia. The research assistant completed semi-structured phone-based interviews with 13 discharged patients. The interviews varied in duration from 25 to 76 min. All interviews were conducted in English via speaker phone and manually recorded using a digital voice recorder. Recordings were uploaded and saved to a secure General Data Protection Regulation (GDPR) compliant online research folder with additional backups saved to another secure platform. All interviews were transcribed verbatim by the research assistant.
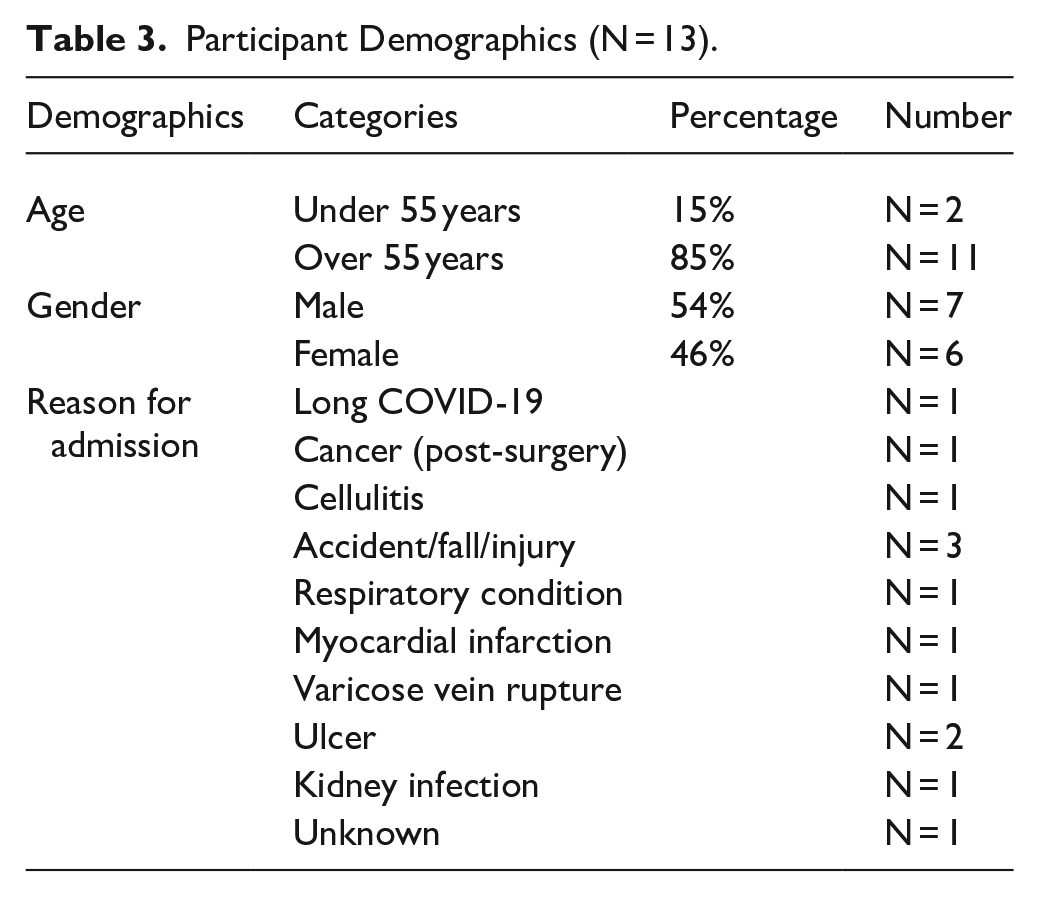
Table 3 outlines participant demographics and reason for admission to the ICF.
Participant Demographics (N = 13).
Data Analysis
Thematic analysis can serve as a flexible approach to exploring the generated data and can assist in yielding rich knowledge from large qualitative data sets. 29 Data was analyzed using Braun and Clarke’s 6 stage thematic analysis process: familiarization with the data/transcription of verbal data; generating initial codes; searching for themes; reviewing themes; defining and naming themes and producing the report. 30 Inductive thematic analysis was deemed appropriate for this study due to its ability to identify themes and patterns of meaning amongst the data within the context of the research aim. 30 NVivo qualitative data analysis software (QSR International NVT20) was used for data coding. 31 Each interview was assigned a memo in which the research assistant made analytical notes on each transcript (stage 1), and then coded each individual transcript (stage 2). Authors 2, 3, 4 and 9 each separately reviewed 2 different transcripts and the associated codes to support coding accuracy. Transcripts were read through (stage 3) and candidate themes were generated and discussed and agreed upon with all authors (stage 4). These were then refined and finalized into the study’s main themes (stage 5) to produce the final report/findings (stage 6).
Schwandt et al 32 4 dimensions criteria for ensuring rigor – credibility, dependability, confirmability and transferability – were applied throughout the research. A reflective journal that captured reflective commentary by the research team was maintained throughout the analysis process. This included the identification of any potential known bias held prior to the coding process. Described as the engagement by researchers in the ‘explicit self-aware meta-analysis’ 33 reflexivity is an important component in ensuring quality and transparency within qualitative research. Rigor was also supported through regular meetings and consultation with the wider research team to discuss progress and agreement throughout the analysis stages.
Results
Three main themes were identified following Braun & Clarke’s 6-phase thematic analysis: (1) Novel healthcare setting, (2) Person-centered care and (3) Psycho-social climate. Each main theme contained categories as outlined below 30 :

Novel Healthcare Setting
Theme 1 describes participant’s reflections on the novel nature of the ICF as a temporary healthcare setting established in a non-medical facility during a global pandemic, their initial impressions, the wider impact of the COVID-19 pandemic context and the responsive infection control procedures in place.
Initial Impressions
Cormac outlined how the novelty of the setting and context led to a feeling of being part of something unusual.
Also, it [felt] that you were taking part in something new something. . .a little bit strange.
One participant, when discussing admission to the ICF reflected on her surprise at receiving hospital care in a university sports arena.
I ended up in the. . .basketball arena . . .a place I never thought I would inhabit but then again.
Tina associated the ICF with historical imagery pre-admission.
I was thinking of all the war photo pictures and war films that I would have seen, where there were tents put up (laughs). . .and the army and beds and the nurses looking after them.
Other participants such as Ted spoke of their initial shock upon entering the facility.
Yeah yeah it was quite shocking when I wound up out in the. . .the gym as I call it.
The facility evoked contrasting emotions for patients. For 1 participant, the sports arena induced sadness:
I’m not here going to rugby matches, which I love, I love rugby. . .but it’s gone
In contrast, this novel facility acted as a source of comfort and hope for another patient by conjuring memories of sports played in the arena and envisioning a future where such activities would resume post-pandemic:
Others were laughing at it, but to me, it was nice because, I could visualise all the sports that had taken place in that area and all the sports that would continue when this pandemic had finished
Physical Environment
Commentary on the design of the physical environment was predominantly positive, although some patients disliked the ‘Nightingale’ ward plan. Nightingale-style layouts, such as that in the ICF, consist of 1 large room divided into bays containing partitioned beds. Conversely other patients described this layout as conducive to social interaction amongst patients and staff. Participants spoke of the reassurances they felt by being observed by staff on a regular basis.
There was people around you all of the time. . .in ICU you’re. . .you’re isolated. . .you only see a nurse when they come into a room or you call them. . .in [the ICF], you’re like you were open there. . .you could talk to your neighbors and all
Melanie also outlined how the ward layout counteracted feelings of isolation that may be experienced in other settings:
Because I suppose the fact that there was no walls. . .you could kind of just look over the half wall ‘Howya neighbor’ like d’you know?. . . and we were all sort of in in in in like kind of a boarding school you know all in our little beds.
Patients had varied perspectives on the privacy offered in the ICF facility. For instance, Marcus felt that the privacy provided in the ICF was superior to that in the acute hospital.
I had more privacy than I ever had in the hospital, we all had our own cubicle, and you didn’t have people kind of looking, gawking at you all the time you literally had a private room.
Cormac’s quotes illustrate how individual personalities affect perceptions of the healthcare physical environment. Initially, Cormac, who described himself as a private person, expressed a strong preference for a single room to support his recovery.
I was looking at this long aisle with all of these beds and to be honest with you I am a private kind of ward person. I simply like to be in a room on my own . . .
However, Cormac’s views evolved during his stay in the ICF, and he spoke about how the physical layout encouraged mutual support among patients.
Actually, I got friendly with one man, we got on very well together. . . and another thing I noticed actually after a day or two, people looked out for each other. . .
Comparisons were made to typical hospital buildings. The sports arena facility supported rehabilitation and provided ample space for walks, helping patients stay active.
Yeah, compared to the hospital I felt it was very kind of a great feeling of space you know and expansive. . . There were just loads of kind of space in the facility where you’d go for kind of walks on your own.
COVID-19 Context
Participants spoke of the impact the wider COVID-19 context had on their admission. Additionally, some participants spoke of the reassurance they felt being in the ICF during the pandemic due to the infection control procedures in place and the knowledge that all patients had tested negative for COVID-19 prior to admission. Cormac spoke of his fears around contracting the disease in the community and the reassurance he felt when in the ICF.
We were all terribly frightened I was really frightened, being in town having to go into town to do shops shopping you know. . .But ahm that was one of the things that struck me that, ‘relax Cormac, you’re in a COVID free environment’
When speaking about her feelings prior to transferring from the acute setting to the ICF, Una outlined the relief she felt regarding the pre-admission testing regime:
I felt wonderful. . . for the fact that I was getting out of the hospital because I knew that COVID numbers were were already very very high and ahm I wanted to be in an environment where everyone was swabbed and proved negative
Participants also outlined their sense of safety in the ICF due to the cleanliness of the environment.
It was just so pristine. . .so clean and you felt really safe when it came to any kind of cross infection which wasn’t there . . .you just felt you could recover there.
It was clean, very clean. . .oh god it was. . .very clean
Person-Centered Care
Theme 2 describes the participant’s experience of person-centered care provision. Participants described interprofessional care that they considered compassionate and reassuring. Patients outlined how they felt staff often went above and beyond the call of duty to provide a holistic service and meet patients’ medical and non-medical needs.
Individualized Care
Participants perceived that ICF staff were genuinely interested in their individual needs and preferences, from health professionals to support personnel.
Everybody there was interested in you, from the girls working in the kitchen, the nurses, the nurses’ assistants, the doctors, everybody was interested. The girls in the kitchen, who I assume were only working for a catering company, even they were interested in my dietary needs. . .now this was without instruction from me she knew already
Cormac outlined a time where he received support from staff following a bereavement. He described how a care assistant provided a listening ear in the absence of friends and family.
I always remember she looked at me and she said ahm ‘if I could’, she said, ‘I’d give you a big hug’
Participants spoke highly of the amount of time and attention they received from staff which led to a sense of being supported, reassured and listened to during a period in which they felt vulnerable due to their care needs.
When you’re in hospital generally you, you feel vulnerable and that’s one thing I didn’t feel vulnerable out in the care center. . .I think they gave more, they they gave you more reassurance all the time
Patients received care from a variety of disciplines within the ICF. Una spoke of her positive experience from receiving regular and consistent contact with doctors and support from other team members when required.
So that’s another positive they were always around, the doctors, and when I did come to the stage where I needed physiotherapy I saw the physiotherapist twice a day
Cormac’s quote highlights his appreciation for the holistic and interprofessional approach adopted in the ICF.
What impressed me was the thoroughness and by that, I mean: I saw the occupational therapist they took me down to the occupational therapy room and they made me sit on seats of different sizes to make sure I could stand up. . . I used to go for long walks around the arena and they sent the physiotherapist to see me. They gave me a whole lot of connections to my local Health Center. Different disciplines there, the pharmacist when I was leaving. . .came and chatted with me for about half an hour about my different drugs.
Eddie described how staff appeared to work together which was seen to optimize patient outcomes.
I just got a feeling that there was ahm you know different ah. . . different departments that were kinda wor- working together to ah. . .give a good out- outcome to people you know
Patients provided compelling examples of how care received in the ICF changed peoples’ outlooks and supported their recovery:
There was one particular guy that came in, now he was in a bad way, he had cancer. Rather than say hello to me he said I’m terminal he said I’m finished and the face, long face everybody could see he was clearly unhappy. . .within two days a wide smile in his face and he was walking up and down the ward on a frame with the nurses
Notably, during a time where visitation could not be facilitated due to infection control restrictions relating to COVID-19, the Patient Advocacy Liaison Service (PALS) initiative was positively appraised by many participants. One patient shared their experiences as follows:
“another thing ahm that meant a lot was. . .ah that was with PALS. . .that meant a lot she was bringing me in little bits from the shop”. . . little things, mi- might not mean a lot to most people. . .but
Una’s description highlights the multidisciplinary, coordinated, individualized approach in preparing patients for discharge.
The physiotherapist wanted to know did I have stairs at home, the occupational therapist wanted to know had I little rails along the wall, did I need a commode in my room, oh it was second to none, oh twas twas. . .they were all. . .all of the disciplines they were all involved in the discharge
Across participant narratives, there was a unanimous view that this type of rehabilitative unit should be available to support patients’ recovery.
That was incredible, like when you’re getting that kind of care, it’s the way the hospital should be. . . I described it as a perfect hospital. That is the way that people should be dealt with. . . but this is the first time that I got that level of care afterwards. . . you need some kind of a step down, you need some kind of proper care as you come down. There’s no point in saying, ‘look you’re grand, go away home,’ and then you can swing for it
Dignity and Comfort
Although participants outlined many elements of the ICF that enhanced their care experience, others outlined challenges around maintaining dignity and comfort. Many participants described the need to use a commode at their bedside due to mobility issues. Some spoke of the negative impact this had on their sense of privacy and dignity in the space, despite the use of screens to partially address privacy.
Well I it’s it’s its just if you were on a commode people could see you on the commode. . . that’s where you know your privacy. . .people could actually see you.
Additional shortcomings were outlined, such as the challenges of temperature control in the facility, the open nature of the layout which led to an increase in noise at times and the lack of outdoor space.
But the one thing that used to annoy me was it had a tin roof and the. . .the. . . .the. . .there was lashing rain at the time and you know, when you’re, when you’re confined to a space like that and you can hear the rain pouring off the roof. . .
The coldness of the facility was overcome by the warmth of the staff’s interactions with patients as illustrated by the following quotation:
It was damn cold (laughs), but then, once you kind of settled in, I had the nice bed. I know it wasn’t; you know, it was kind of open, which was fine. And of course, the staff were beyond nice. . . the nurses were lovely
Participants’ sense of comfort was attributed to the more relaxed ICF environment, continuous availability of care and the smaller, more attentive staff-to-patient ratio.
There was an ease about it; you were a lot more comfortable. There was care available all the time. Even the consultant herself was extremely nice. I think the secret to the place is the smaller numbers; there seemed to be more staff, and you got more attention. There was a relaxation about the place, unlike the pressure you normally feel in a hospital.
Psychosocial Climate
Theme 3 describes the participant’s experiences of the inclusive atmosphere in the ICF and the emotions experienced on discharge.
Inclusive Atmosphere
Cormac, who had experienced inpatient care in various healthcare systems, reflected on the distinct ICF atmosphere. He suggested that the culture in the ICF, free from entrenched practices and hierarchies of traditional healthcare settings, fostered a more open, flexible and inclusive environment for staff.
The atmosphere there was lovely, you know. There was a buzz and energy about the place . . . I think staff went into a situation and there were no rules, there was no tradition. You didn’t have a nurse manager on the ward who had been there for 15 years and things were done her way or no way. . .
Another factor that contributed to the psychosocial climate was the positive multidisciplinary team ethos, as illustrated by Cormac’s description of his interaction with a ward manager who shared her experience of setting up the ICF.
We arrived here in June and started setting up. Initially, I thought, ‘This is where we’re going to work.’ We came from diverse backgrounds — some from orthopedics, others from general nursing. Some had returned from the UK, others from Australia. But for some reason, this group gelled. It worked. We all realized we were part of something new, something worthwhile, and we were creating something different
Marcus reflected fondly on how staff and patients would get together to sing songs. This contributed to an atmosphere of ease within the ICF.
There was a ladies section in this in this unit. . .and they were having sing songs every night. . .they seemed to be having a great time and it came down from the staff helping to do it. There was an ease about it there was no you know. . . there was care available all the time.
Melanie described the ICF as a ‘joyous place’. She spoke of friendships she formed with fellow patients on the ward and the contribution of the nursing staff to creating an inclusive atmosphere. This simple act of offering tea fostered dialog and cultivated feelings of trust, safety and normalcy.
We were the, the four trouble makers at the end. . . the nurses would be bringing about tea and slices of toast and even birthday cake on occasion (laughs).
Violet drew comparisons between the ICF and being at home or with family:
Ahm. . .you know you, in the in the finish I was treating the staff as family, you know we. . .yeah they were very friendly. You know ‘twas so, ‘twas homely, ‘twas home[ly], yeah.
This inclusive psychosocial environment characterized by supportive relationships and a sense of community, played a key role in promoting healing, recovery and rehabilitation:
When people relax they kind of heal better and, and, the pressure is gone and the fear because your out of the hospital but you’re still being looked after.
Many participants described feeling emotional upon discharge. Tina outlined how she had come to know people in the ICF and how she would miss the reassurance she felt when meeting a doctor each day.
I felt a bit emotional leaving because. . .I suppose I had come to know them all. . .and I was settled and I was happy. . .and ahm I suppose one of the things (laughs) ah I was going to miss the most important thing I was going to miss there. . .was the fact and a very realistic fact for me was I had a doctor every morning.
Melanie reflected on the positive memories she had of the ICF and how emotional she was when leaving.
I actually cried the day I left.
Violet also described an emotional departure and how she would miss the ICF:
Well sure everyone loves to go home you know but. . .I missed, d’you know a. . .a tear came to my eye. . .the nurses, absolutely you know they were, they were lovely.
Discussion
This study describes the experience of 13 patients who received care in the ICF during the COVID-19 pandemic. Three main themes emerged following analysis of the data: the ICF as a novel healthcare setting; person-centered care and psycho-social climate. It highlights pertinent factors relating to the patient experience of receiving care in a field hospital during the COVID-19 pandemic.
The experience of being a patient of the ICF in the backdrop of the COVID-19 pandemic was a recurring theme throughout the interviews. Receiving care during the pandemic has been identified as an altered patient experience. 34 Patients’ experiences of acute healthcare during the COVID-19 pandemic were significantly different from their pre-pandemic experiences. Changes to routine care, delays in treatment, reduced staff responsiveness, the use of personal protective equipment, social distancing measures and visitor restrictions led to higher levels of fear, anxiety and stress, and changed the dynamics of patient-provider interactions.35,36 Key et al 37 conducted a quantitative survey on patients in the UK who had received in-patient care during the pandemic (N = 704). The research highlighted that during their period of care, patients had worries relating to contracting the virus and experienced loneliness during their admission. 37 In the ICF, participants spoke of their own fears of contracting the virus primarily prior to admission, however the large, open-air nature of the facility and the testing regime pre-admission were commented on by patients as being protective factors against the spread of infection in the ICF. Patients reflected on being able to see staff walking by and the ‘Nightingale’ style layout appeared conducive to ameliorating feelings of loneliness and to the forming of friendships between patients. Nightingale-style layouts, increases visibility between staff and patients and may enhance monitoring and communication. Patients perceive healthcare provider accessibility as a key dimension of high-quality healthcare. 38 Furthermore, patient visibility is a high priority for safety and healthcare facility design may shape the dynamic flow of interaction and communication between patients. 39
Conversely, certain design features of the ICF were negatively perceived by patients, such as the nighttime drop in temperature, the noise levels and lack of privacy and dignity. A narrative review conducted by Lin et al 40 concluded that the physical environment can influence patient’s perceived feelings of being dignified in the in-patient setting. Furthermore, the physical healthcare facility may be a key factor in relation to recovery and rehabilitation of the patient and impact on patient satisfaction. 41 In this regard the open and communal nature of this ICF led to privacy concerns for some patients. Field hospital design needs to consider how patient privacy can be optimized in a field hospital facility, whilst implementing infection prevention and control measures. The ICF was not constrained by typical hospital designs. Findings suggest that healthcare facilities with a rehabilitative focus may benefit from alternative designs that do not evoke associations with illness.
The psychosocial climate of the ICF emerged as a key feature of the patient experience and served to moderate the limitations of the physical environment. The literature acknowledges that a supportive psychosocial caring climate may improve patient outcomes by reducing anxiety, stress, reduced rehabilitation times, increased healing and shorter periods of hospitalization and healthcare costs. 42 Browall et al 43 reported that the psychosocial climate of the ward was most important in the context of creating a caring environment, more so than the physical space itself. An empathetic approach by staff in which patients were afforded time to talk to them, as well as staff showing an interest in their patients, created an atmosphere of partnership and patient empowerment. Our study also reports that some participants saw the staff almost as family, an indication of the caring atmosphere created within the ICF. This was further evidenced when participants spoke of being tearful at the thought of discharge. The relaxed atmosphere described by participants is notable during a time of a global pandemic, and patients were likely at their most vulnerable while receiving hospital care in a temporary facility. Such a sense of belonging has also been hypothesized as serving as a protective factor against patient vulnerability. 44
Participants acknowledged the role of PALS, serving as a point of contact for patients and their families and offering advice and support. 45 Previous research in the UK has identified the value of PALS teams who act as navigators of services and concluded that this service has the potential to increase patient satisfaction with a service. 46
A patient-centered approach was evident across participants’ descriptions of care. Patient-centered care is a primary approach to health service provision and seen as an important component of high-quality care, which can lead to improved health outcomes and higher service user satisfaction amongst patients.47,48 Creating a partnership between providers and patients, placing emphasis on patient’s needs from their perspective and adopting a flexible method of service delivery are all avenues through which patient-centered care can be applied in health care settings. 49 Patient-centeredness as an approach embodies the use of a compassionate and empathetic service which acknowledges the personal preferences and subjective needs of those receiving care. 50 As well as respecting individual’s values and preferences, the provision of emotional support, attention to physical comfort, coordinated and integrated service delivery and the involvement of family are all recognized components of patient-centered care. 50
Findings of this study described patient-centered care through the provision of a multi-disciplinary interprofessional service which met the subjective needs of patients through individualized supports. Participants spoke of how their emotional and non-medical needs were tended to by staff as well as their physical rehabilitative needs. These staff interactions align with the principles of patient-centered care and were seen as imperative to patient wellbeing given the absence of direct family and/or friend involvement on site due to COVID-19 restrictions.
Despite the evidenced benefits of patient-centered care, research outlines how its real-time application in practice can be challenging. 48 Routines in practice that ‘initiate, integrate and safeguard’ such an approach are required to ensure its application on a day-to-day basis. 48 One factor that may have supported the implementation of a coordinated and patient-centered approach was the high level of resourcing provided for the operation of the ICF, which may have afforded staff the time to meet the multifaceted needs of their patients, both rehabilitative and otherwise. And while patient-centered care is more often framed as a positive approach, it is essential to critically examine how it is actualized in ICF type facilities and if the design and branding genuinely prioritize patients or if they serve institutional goals, such as efficiency and throughput.
In terms of the scalability of ICFs, future research should explore the feasibility of implementing ICFs in various healthcare settings and if this approach can be adapted for other health crises or diseases, particularly those that require a step-down approach. The principles of ICFs – interprofessional collaboration, person-centered care and a focus on rehabilitation – can be beneficial in managing chronic illnesses, post-surgical recovery and even during non-pandemic situations where hospital capacity is strained. However, the design and operational protocols may need to be adjusted to attend to the needs of patients with different conditions, ensuring that the care environment remains conducive to their recovery.
Recommendations
The findings of the present study identified common quality dimensions that are important to patients accessing a field hospital during a health-related emergency and that health policy makers can take into consideration when planning and designing a field hospital.
Priority areas for consideration include availability of the interprofessional team to progress patient care, provision of patient-centered care, involvement of a variety of services and the importance of the physical and psychosocial climate to patient experiences. Pre-admission information on the healthcare facility including infection control procedures in place may prepare patients for the physical environment of care. Field hospitals set up to respond to a crisis need to consider involving services such as PALS which has the potential to support patients to navigate a new service.
Conclusions
The findings of this study are relevant for health care and related staff, health service managers and policy developers both in the context of post-acute care, in-patient rehabilitative care and pandemic preparedness and response. Although the ICF was not without its challenges, in this study, patients spoke about their time in the ICF as a mainly positive experience. Infection control procedures in the time of a pandemic, person-centered care, physical layout and design elements and the psychosocial climate emerged as key features of the ICF, all of which should be considered for future initiatives of a similar nature.
Footnotes
Appendices
Appendix 2
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
All authors were employed by the health service and/or the host university in which the ICF was situated during the conduction of the research. Ethical approval was obtained from Irish Health Service Executive Research Ethics Committee (reference number 092/2020). Participation was voluntary and participants were fully informed of the study’s purpose prior to engaging in the research. All participants provided informed consent. Ethical approval has not been granted for data sharing.