
Abstract
Objective:
Metabolic syndrome is a cluster of cardiovascular risk factors (central obesity, hypertension, dyslipidemia, and insulin resistance) that affects between 12.5% and 31.4% of adults worldwide. It correlates with increased risks of cardiovascular disease, diabetes, cancer, and overall mortality in a dose-dependent fashion. This review aims to provide primary care clinicians an updated review of the evidence on metabolic syndrome, with a focus on treatment.
Design:
Scoping evidence review.
Eligibility Criteria:
English-language studies of evidence Level I or II that focused on defining, diagnosing, and treating metabolic syndrome or its components.
Information Sources:
PubMed and Cochrane Database of Systematic Reviews.
Results:
Though evidence is still lacking for improved outcomes with treating the syndrome per se, addressing its individual components reduces risks. Lifestyle changes like weight loss and increased physical activity are first line. Surgical options assist with weight loss for certain patients. Pharmacotherapies like glucagon-like peptide-1 receptor agonists, sodium-glucose cotransporter-2 inhibitors, statins, and antihypertensives also have efficacy.
Conclusions:
Metabolic syndrome is an independent risk factor for many poor health outcomes. Its individual components should be treated with medication and behavioral changes to reduce cardiovascular risk and prevent diabetes and its complications. More research is needed on how to treat the syndrome itself. A diagnosis of metabolic syndrome may be useful for motivating patients toward lifestyle changes, though more research is needed on how to treat the syndrome versus its components.
Key Points
This research is focused on providing an updated review of the evidence on metabolic syndrome for primary care clinicians by exploring the diagnosis and treatment options for metabolic syndrome.
Treating individual components of metabolic syndrome can reduce atherosclerotic cardiovascular disease risk while treatment of the syndrome as a whole has unclear outcomes. Intensive lifestyle change based behavioral interventions are effective for ≥5% weight loss and diabetes prevention aspects of metabolic syndrome management (SORT level B). Medications and surgeries are effective for weight loss ≥5% to 20% and diabetes prevention in patients with metabolic syndrome (SORT Level B).
This research may help improve the management of patients with metabolic syndrome in primary care settings.
Introduction
Metabolic syndrome is a group of health conditions that occur together and increase the risk of developing serious health problems. Global metabolic syndrome prevalence ranges from 12.5% to 31.4%. 1 One in 20 adolescents worldwide had metabolic syndrome in 2020, as well as about 3% of children 2 ; it is more common in the US (34.5 ± 0.9%) 3 and Canada (19.1%). 4 Metabolic syndrome correlates with cardiovascular disease (CVD), nonalcoholic fatty liver disease (NAFLD), inflammation, cancer risks, chronic kidney disease (CKD), dyslipidemia, type 2 diabetes (T2DM) and insulin resistance, childhood obesity, and overall mortality. However, primary care providers can treat this syndrome with a combination of effective behavioral techniques, growing medical management options, and surgical interventions.
Primary care clinicians frequently manage patients with risk factors and/or a diagnosis of metabolic syndrome. This article offers an updated review of the evidence about the prevalence, pathophysiology, associated conditions, assessment tools, and treatment of metabolic syndrome.
Methods
The prevalence of metabolic syndrome makes it a frequently studied condition, so high-level evidence was available for review. A total of 340 articles found through searches of the PubMed and Cochrane databases were reviewed by the authors May to September 2023. Keywords included metabolic syndrome, MetS, ASCVD, blood pressure, lipid, Homa-IR, Waist circumference, A1c, and their equivalents/abbreviations/pluralities. Date range of articles was 2002 to 2023. These 2 databases were chosen for their broad reaching scope, and no others were included due to time limitations of the team. The title and abstract screening was performed by 1 author. A total of 69 articles were excluded based on abstract being irrelevant. A detailed annotated bibliography was performed for 271 articles with abstracts in Microsoft Word. There were 2 articles on A1c and MetS, 2 on ASCVD and MetS, 60 on Blood pressure and MetS, 212 on lipids and MetS, 49 on Homa-IR and Mets (or 30 on fasting glucose and Met S), and 15 on Waist circumference (or BMI) and Met S. No efforts were able to be made to pursue acquiring the 31 articles for which the team did not have access. About 72 English-language studies with Level I or Level II quality of evidence underwent full text review by 1 author, with 2 authors reviewing. No interrater review calculations were performed, but the authors all agreed on the final annotated bibliography and which articles to include in drafts. The reasons that articles were excluded were lack of Level I-II evidence, inability to access the full study, irrelevance to this study, or lack of space in final document (definitions, pathophysiology, assessment tools were excluded post-hoc during revision process to focus on clinically relevant treatment data). Data items included primary outcomes: metabolic syndrome risk factors, diagnosis, and treatment. The focus of the review was narrowed to metabolic syndrome treatment to accommodate the 50-citation limit for this journal. Studies only describing the definitions and studies focused on a specific risk factor without assessing treatment were subsequently excluded (n = 22, Table 1; Figure 1). Although there was no age cut off for studies’ inclusion, the final draft focused on adult metabolic syndrome, excepting a few pediatric studies that focus on projecting future adult metabolic syndrome. A narrative synthesis approach was used to compare effects with various measures reported, including odds ratios, hazard ratios, and risk ratios. This review was not registered, nor was it a protocol published previously. This study was not funded.
Studies of Risk Factors Associated With Metabolic Syndrome.
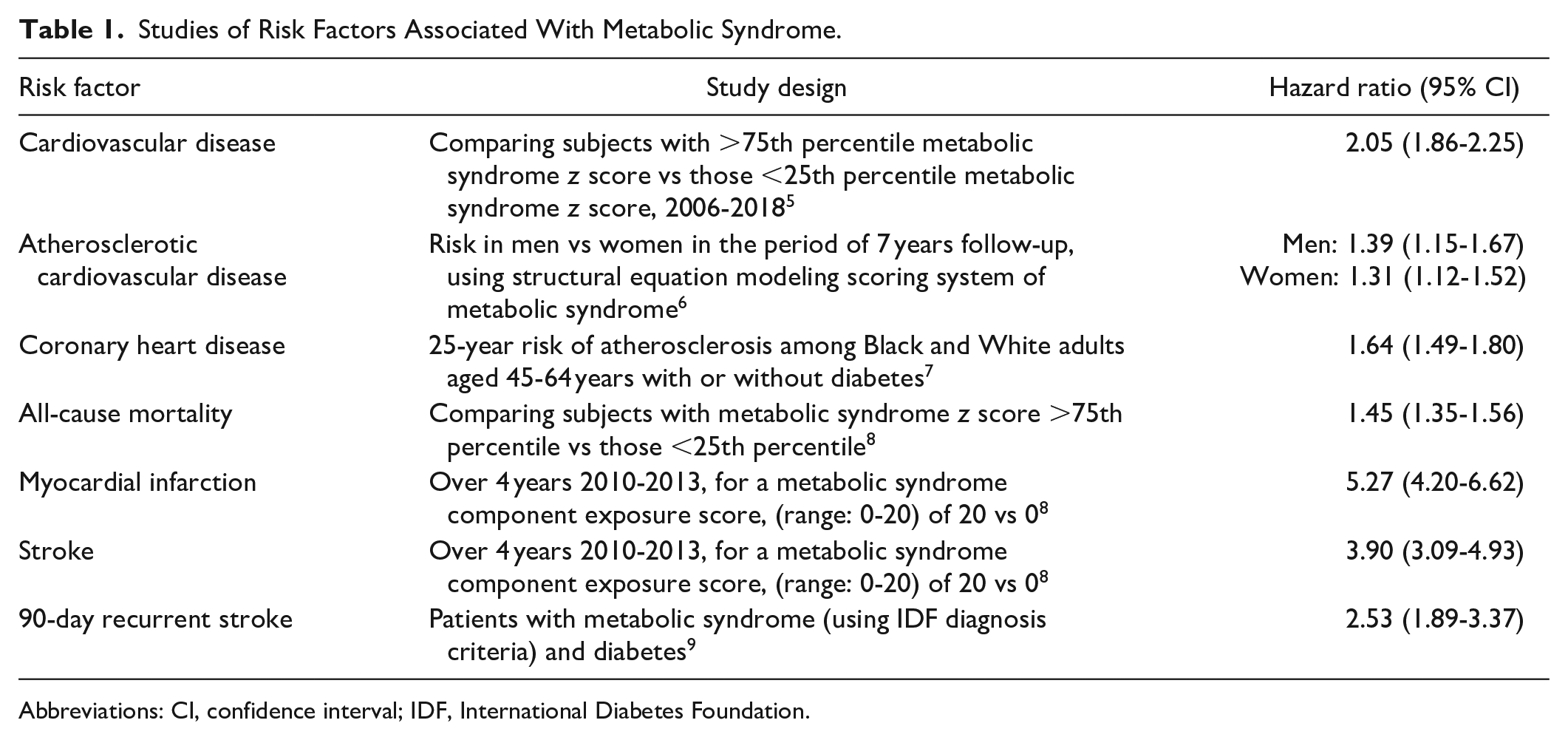
Abbreviations: CI, confidence interval; IDF, International Diabetes Foundation.

PRISMA flow diagram.
Results
Defining Metabolic Syndrome
The 5 main components of metabolic syndrome are abdominal/central obesity, high blood pressure, impaired glucose metabolism (high blood sugar), and triglyceride dysfunction (elevated levels of triglycerides, low levels of high-density lipoprotein cholesterol [HDL-C]), with or without renal dysfunction. A person is diagnosed with metabolic syndrome if they have 3 of these 5 components, depending on which definition is used. 3
The Importance of Treating Metabolic Syndrome
There remains a lack of evidence to show improved patient related outcomes with treatment of the syndrome as a whole. However, there is substantial evidence to report on both disease related outcomes and patient related outcomes for treatment of the syndrome’s individual components. The primary clinical outcome with the biggest impact is ASCVD risk reduction. (Table 2).
Comparison of Interventions for Metabolic Syndrome, by Component Diagnoses.

Abbreviations: SR, sustained release; Subq, subcutaneous; T2DM, Type 2 diabetes mellitus; Tx, treatment; Vs, versus; w/, with; WL, weight loss; w/o, without.
Metabolic Syndrome Scoping Review References.

Participants unless otherwise specified.
if available.
Treatment of Metabolic Syndrome
A combination of pharmacologic options; a plant-based, whole foods diet; and exercise can decrease the severity of metabolic syndrome components, hence, reducing the risk of morbidity and mortality associated with metabolic syndrome.
Therapeutic lifestyle changes
In children, a weight-maintenance approach during growth with a focus on healthy habits is generally preferred as opposed to weight loss as a goal. Address the 5210 model (5 daily fruits/vegetables, <2 h screen time, 1 h exercise, and 0 sodas) at well-child checks, and ask whether the child’s parents encourage regular family movement activities. 22 The 5210 model has been validated and shown to increase children’s fruit and vegetable intake from 18% to 23% (P < .001) over 4 years. 22
In adults, enacting changes toward a healthier lifestyle and a weight loss of 5% to 10% of initial body weight are generally recommended to treat metabolic syndrome. Lifestyle changes including moderate/vigorous physical activity are necessary for treating metabolic syndrome and its components and are more effective than metformin or placebo, but the question of how to effect these changes remains complex and the subject of public health research.23 -26
In the primary care setting, behavioral weight loss interventions in groups such as the US National Diabetes Prevention Program have been shown to be superior to self-directed weight loss for patients with metabolic syndrome. 27 Quarterly primary care visits for lifestyle counselling for patients with 2 or more metabolic syndrome components over 2 years showed at least a 5% weight loss for about 21% of patients. 28 Items such as weight goals, weight history, and risk factors of metabolic syndrome may be useful topics for lifestyle discussion. Telehealth weight loss interventions are beginning to be explored for patients with metabolic syndrome as well. 29
Any sustained behavior change that involves increased physical activity may be helpful to treat metabolic syndrome. Exercise programs ranging from moderate continuous and high-intensity interval training to yoga and Tai Chi can improve metabolic profiles and reduce metabolic syndrome severity.30 -33
Adherence to specific diets, such as the Mediterranean-type diet, Dietary Approaches to Stop Hypertension (DASH) diet, and diets low in processed and inflammatory foods and high in lean fish and colorful vegetables, also can improve metabolic profiles and reduce the risk of metabolic syndrome.34 -44 The Mediterranean diet has been shown to lower overall and cardiovascular mortality for patients with metabolic syndrome. 45
Pharmacotherapy
There are multiple pharmacologic options with evidence of improving metabolic syndrome components.
Only 27% of people who followed diet and exercise alone were able to lose 5% of body weight. However, semaglutide (number needed to treat [NNT] = 2) and liraglutide (NNT = 4) can help people lose at least 10% body weight loss in conjunction with diet and exercise and help achieve HbA1C <7%.15,19 Phentermine combined with topiramate (NNT = 2) supports 5% weight loss and decreasing HbA1C. 21 Naltrexone combined with bupropion demonstrates 5% weight loss (NNT = 4) when compared with placebo. 16 Metabolic syndrome remission was shown with dapagliflozin plus metformin as compared with metformin alone (NNT = 5). 14 In addition, appropriate use of statins, antihypertensives (eg, angiotensin-converting enzyme inhibitors [ACEIs]), medications for lowering glucose (eg, glucagon-like peptide-1 receptor agonists [GLP1s], metformin, sodium-glucose cotransporter-2 inhibitors) can treat components of metabolic syndrome, including diabetes, hypertension, dyslipidemia, and complications of metabolic syndrome such as fatty liver disease. 17
Weight loss options according to the most recent United States Preventive Service Task Force (USPSTF) systematic review 46 include GLP1s (eg, liraglutide and semaglutide), combination naltrexone and bupropion, orlistat, and combination phentermine and topiramate. GLP1s have directly been shown to decrease the severity of metabolic syndrome itself, primarily through weight loss.15,19,21,47 Taking liraglutide for 13 months also has been shown to be associated with lower risk of incident diabetes. 20
Surgical options have been shown to be more effective for weight loss than medical management in certain patients. 18 (Table 2) Bariatric surgeries can be recommended in patients with body mass index (BMI) >35 kg/m2 or those with a BMI >30 kg/m2 and a weight-related comorbidity. 48
Conclusion
Fifteen years after a landmark review of metabolic syndrome, 49 there is still a lack of evidence to show improved patient-related outcomes with treatment of the metabolic syndrome as opposed to its respective components (Table 3). Metabolic syndrome is still an independent risk factor for many poor health outcomes including all-cause mortality, MI, stroke, CVD, CKD, CHD, heart failure, NAFLD, T2DM, cervical cancer, colorectal cancer, and esophageal cancer. Patients should be counselled on these risks as incentive to commit to treatment of metabolic syndrome. 50 Many studies recommend prevention and treatment for metabolic syndrome components through a combination of medication, surgery, and behavioral interventions including diet and exercise. Treating individual components of metabolic syndrome can reduce overall ASCVD risk, prevent diabetes and its complications, and facilitate significant weight loss. More research is needed to compare treatment of metabolic syndrome as a whole versus the sum of its parts and to further system-level changes that facilitate and incentivize healthier lifestyles for families.
Footnotes
Authors’ Note
This manuscript has not been published in another journal and is not under consideration by another journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data
Contact the authors for data used for analyses.