
Abstract
Introduction and Objectives:
Structured physical activity (PA) programs help to prevent and manage chronic diseases, yet systematic approaches to identify and enroll patients in these programs are lacking. Exercise is Medicine Greenville (EIMG) is a novel clinic-to-community model that identifies patients with chronic diseases in primary care settings and connects them to a structured, evidence-informed, community-based PA program. This study assessed influences on PA program enrollment using a mixed methods design.
Methods:
Data were collected from 12 clinics over 18 months. Electronic health record data were used to quantitively compare the characteristics of referred patients who did versus did not enroll. Semi-structured interviews were conducted with a subset of non-enrollees to elucidate barriers and facilitators to enrollment.
Results:
Of the 217 referred patients who were eligible, 84 (38.7%) enrolled in the PA program. A greater percentage of enrollees had a history of high cholesterol (73.8%) relative to non-enrollees (57.9%, χ2 (1, N = 217) = 5.66, P = .02). Twenty-six patients completed qualitative interviews. Three themes emerged from interviews: (1) positive referral experiences with opportunity for enhanced information sharing and improved flow; (2) strong patient motivation, perceived capability, and social support; and (3) external barriers, such as cost and time, that prevented enrollment.
Conclusions:
Findings can guide improvements to the EIMG model, thus increasing its positive impact on individual- and community-level health. Findings can also inform efforts to build similar clinic-to-community PA models at other health systems.
Keywords
Introduction
Regular physical activity (PA) helps to prevent and manage many chronic diseases.1,2 PA reduces risk of developing cardiovascular disease, 1 metabolic disease, 3 osteoporosis, 4 and multiple types of cancers, 5 and it reduces symptoms and slows disease progression among those with existing chronic diseases,1,2 The benefits of PA also extend beyond individual-level health, as regular PA is associated with reduced healthcare spending and costs. 6
Structured PA programs are effective in increasing PA among individuals with chronic diseases. 7 However, there have been persistent challenges in establishing sustainable PA resources within community settings, and in effectively connecting patients to these programs. 8 In 2007, the American College of Sports Medicine launched the Exercise is Medicine (EIM) initiative in part to help address these problems. 9 EIM aims to make PA assessment and promotion a standard part of disease prevention and treatment, and to connect patients with suboptimal PA seen in clinical settings with appropriate community-based PA resources. 10
Multiple healthcare systems and other institutions (eg, universities) have incorporated pieces of the EIM model, such as PA assessment and prescription, into their services.11,12 However, fewer systems have implemented comprehensive pathways that involve assessing PA and referring patients to a standardized PA program, with an infrastructure to support doing so. One example of a comprehensive PA assessment and referral pathway is the Exercise is Medicine Greenville (EIMG) program at Prisma Health, in partnership with the University of South Carolina School of Medicine Greenville and the YMCA of Greenville, in upstate South Carolina (SC).9,13 When patients with relevant chronic conditions (eg, hypertension, obesity, and diabetes) and/or low PA are seen at participating clinics within the Prisma Health system, their primary care providers can refer them to a network of community PA facilities (6 local YMCAs and 1 medical fitness center) offering a standardized, evidence-informed PA program. Past research has shown that completion of the 12-week community PA program confers health benefits and that the program is well received by participants. 13 Patient engagement through the EIMG model thus has significant potential to improve the health of patients living in the Greenville, SC region.
Since EIMG started in 2016, nearly 2000 patients have been referred to the community-based PA programs. While many referred patients enroll in the PA program, others do not. Prior studies have looked at reasons why patients drop out from similar provider-referred PA programs, but much less is known about why patients do or do not start these programs in the first place.14 -16 This knowledge gap hinders efforts to build clinic-to-community PA models that effectively engage as many patients as possible, as it is unclear which factors most strongly influence whether patients want to and feel able to participate. Further, most of the few studies that have examined patient participation (or lack thereof) in physician-referred PA programs have focused on static sociodemographic predictors; only a handful have applied a broader lens to examine multi-level, multi-factorial influences on enrollment decisions.14,15,17 -20 Cumulatively, this work suggests that men and younger individuals are less likely to enroll in physician-referred PA programs, and that factors like work obligations, motivation, environmental characteristics, and social dynamics influence enrollment decisions.14,15,17 -20 Patients’ interpersonal experiences with their healthcare providers can also influence health behaviors and referral uptake, yet these factors have rarely been considered in prior work. 18
Although these findings shed light on potential reasons why EIMG-referred patients do not enroll in the PA program, the literature is quite limited, necessitating additional study of comprehensive influences on decision making around enrollment in physician-referred PA programs. Additionally, prior work has been conducted almost exclusively in the context of exercise referral schemes outside of the United States (US).14,15 Although these schemes bear similarities to EIMG, there are also important differences in model components, such as the type of PA resources that patients are referred to (eg, degree of structure) and how the healthcare systems operate (eg, payer structure). It is thus unclear how well prior findings translate to US-based settings.
In summary, innovative clinic-to-community PA models like EIMG have great potential to increase PA among patients with chronic diseases, thereby improving health outcomes. However, much remains to be learned about why patients referred to community-based PA programs through such models ultimately do or do not enroll. Clarifying factors that most strongly impact enrollment decisions among EIMG patients can: (1) inform refinements to the EIMG program at Prisma Health to optimize enrollment, and (2) inform future efforts to build effective clinic-to-community PA models at other US-based health systems.
This mixed-method study aimed to comprehensively assess influences on EIMG patient enrollment in the community-based PA program. Aim 1 was to quantitatively evaluate whether sociodemographic characteristics, patient health characteristics, health care utilization characteristics, or neighborhood characteristics differed among referred patients who did versus did not enroll using electronic health record (EHR) data. Aim 2 was to further understand reasons why patients did not enroll in the PA program through qualitative interviews with a subset of patients who were referred to the PA program but did not enroll.
Methods
Overview of the Study and Enrollment Process
Data were collected as part of a broader study that assessed the implementation of the EIMG program at 12 primary care clinics (n = 5 family medicine, n = 7 internal medicine) over an 18-month period (March 15, 2021 to September 15, 2022). This paper reports on factors impacting patient enrollment in the PA program. Findings on other outcomes of interest for the parent study (eg, reach, cost) have yet to be published. Study procedures were approved by the Prisma Health Institutional Review Board.
Enrollment in the PA program involves 3 steps (see Supplemental File 1). First, patients complete a short assessment of their current PA behavior (answer 2 questions that will equate to number of min/week of PA) and, if appropriate, receive an EIMG referral from their healthcare provider during a clinic visit (step 1). This involves the provider speaking with the patient about the PA program and completing an EHR referral process to officially refer the patient to the program. An EIMG Care Coordinator (ie, nurse navigator) follows up within 3 business days (but no more than 3 contacts) to answer questions about the program, verify eligibility, and facilitate enrollment at 1 of the 7 community PA program locations (step 2). Last, interested patients meet with an EIMG Facility Coordinator, who is a staff member at one of the designated PA program locations, for an orientation visit to start the PA program (step 3). Patients may also apply for financial assistance (ie, scholarships covering up to 90% of program costs) through the participating YMCA programs. If they do, they may speak with additional PA center staff and complete additional electronic forms with support from the staff.
Study Participants and Eligibility
Patients are eligible to receive an EIMG referral if they are attending a clinic where EIMG is activated (ie, where providers have been trained on the program and can submit referrals), are ≥18 years old, and are physically inactive (<150 min of moderate-to-vigorous PA per week) and/or have overweight/obesity, hypertension, hyperlipidemia, diabetes, or other risks of PA-associated chronic diseases. Patients are excluded from enrolling in the PA program if they are diagnosed with a condition listed in Supplemental File 2 or do not have complete referral documentation. Inclusion in this specific study further required patients to have received an EIMG referral at 1 of the 12 clinics included in the parent study between March 15, 2021 and September 15, 2022. This timeline was chosen as the program was re-opened across the system after a COVID-19 shutdown.
Procedures
Quantitative data (study aim 1)
Data were extracted from the EHR for all patients who received an EIMG referral at one of the target clinics during the study period. Based on prior literature,14,15,17 -20 the following variables were extracted: sociodemographic characteristics (age, sex, race/ethnicity, marital status), patient health characteristics (body mass index; history of obesity, physical inactivity, hypertension, and high cholesterol; Charlson comorbidity index), health care utilization characteristics (type of health insurance and number of visits to a Prisma Health provider since 10/01/2020), and environmental characteristics of each patient’s zip code (population aged 16 years and older, median and mean household income, unemployment rate, percentage of families in poverty). Distance from each patients’ home address to the nearest community PA facility was also assessed as an environmental characteristic.
Qualitative data (study aim 2)
All referred patients who were eligible but did not enroll in the PA program were mailed a letter informing them of the opportunity to participate in a study focused on their EIMG referral and decision-making experience. Patients were contacted by phone within 6 weeks of the letters and invited to participate in an individual, semi-structured interview. Three contact attempts by phone and/or text message were made. A phone interview was scheduled with interested patients. Prior to the interview, patients were emailed a study information sheet and consent form. A research assistant obtained verbal informed consent from participants at the start of the interview.
A semi-structured interview guide, based on the COM-B (capability, opportunity, motivation, and behavior) behavior change theory 21 guided interviews (see Supplemental File 3). The COM-B model was selected as a theoretical framework for the interviews given that it assesses diverse, multi-level influences on health-related behaviors and has been previously used to understand engagement in PA programs. 17 The interview guide focused on: (1) patient experiences across the referral/enrollment process; (2) capabilities (physical and psychological), opportunities (social and physical), and motivation (automatic and reflexive) of patients to participate in the PA program; and (3) other potential factors influencing their enrollment decision. Interviews were audio recorded and transcribed verbatim, with all identifying information removed. Patients received a $15 gift card for completing the interview.
Data Analysis
Sociodemographic, patient health, health care utilization, and neighborhood characteristics were characterized using percentages (categorical variables) or mean and standard deviation (continuous variables). Characteristics were compared by enrollment status using chi-square (categorical variables) and Student t-tests (continuous variables). Fisher’s Exact tests rather than chi-square were used for race/ethnicity comparisons due to small cell size in the “Other” category. The significance level was set at α = .05. For the qualitative analyses, thematic deductive coding was used to analyze the individual interview data. Two coders created a codebook using a subset of interviews and the COM-B model. Codebook agreement was tested by the coders using another subset of 4 interviews. Any discrepancies were discussed by the two coders and the first author until consensus was reached; the codebook was subsequently modified as needed to enhance clarity. All transcripts were then uploaded to Dedoose (version 9.2.4) and the remaining transcripts were individually coded. After coding, three research team members analyzed the coding to identify themes. Any discrepancies were resolved through consensus. A power analysis was not conducted due to the naturalistic study design.
Results
Figure 1 displays the CONSORT diagram. As shown in Figure 1a, 335 patients were referred to the PA program and 217 (217/335, 64.8%) were eligible; of those who were eligible, 84 (84/217, 38.7%) enrolled. Table 1 presents descriptive characteristics for the full sample. Supplemental File 4 presents statistical comparisons between patients deemed eligible and ineligible for the PA program. These comparisons were not a primary study focus since eligibility was primarily determined by referral fidelity (eg, appropriate referral or not) rather than patient-level factors.
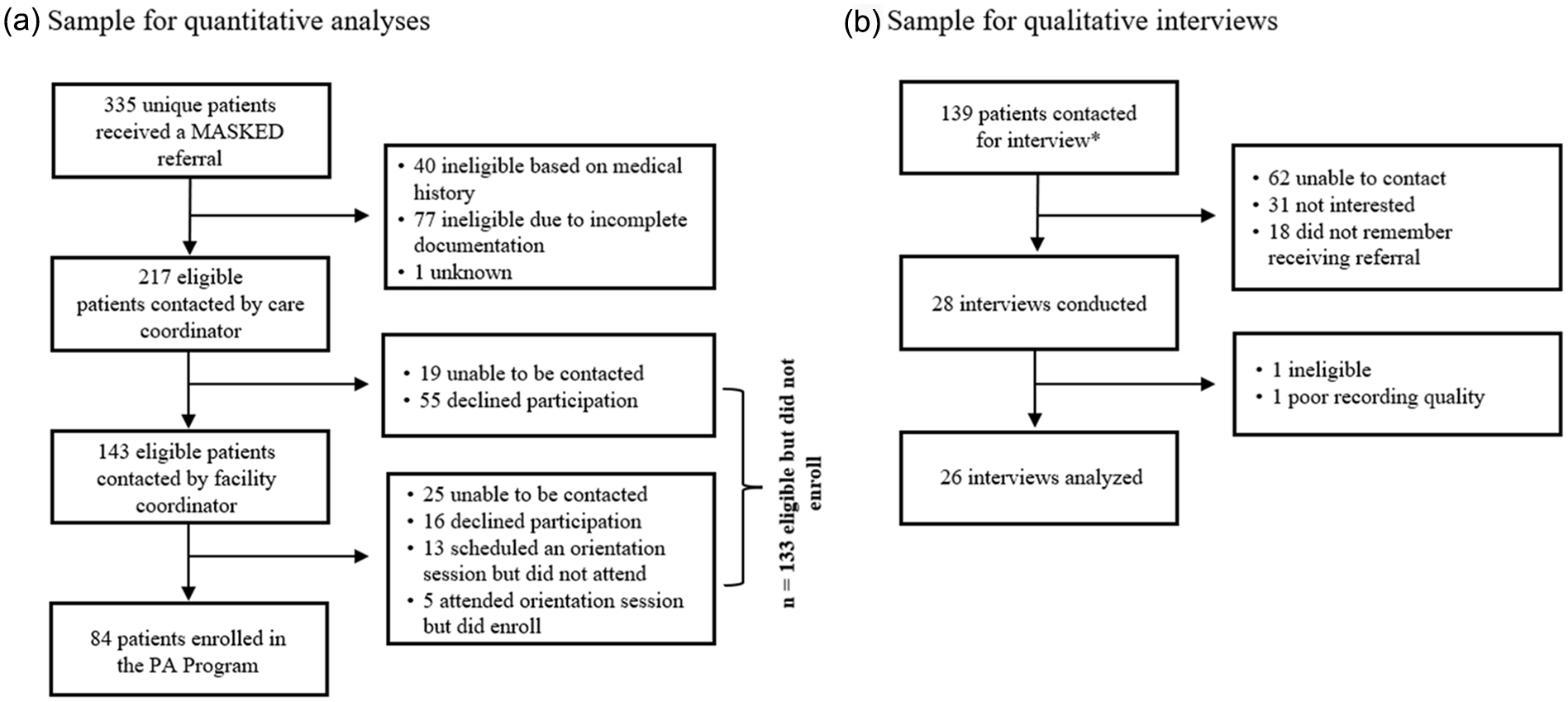
CONSORT diagrams. (a) Shows the CONSORT diagram for the sample of patients included in the quantitative comparisons with electronic health record (EHR) data. (b) Shows the CONSORT diagram for the sample of patients included in the qualitative interviews.
Total Sample Patient Characteristics.

Missingness by variable: Body mass index (n = 2); Marital status (n = 4); CCI (n = 22); all environmental characteristics (n = 1).
Source, US Census data from patient zip code in 2000.
Quantitative Results (Study Aim 1)
Aim 1 sought to quantitatively compare PA program enrollees and non-enrollees on sociodemographic characteristics, patient health characteristics, health care utilization characteristics, and neighborhood characteristics using data from the EHR. Table 2 presents descriptive characteristics for all eligible patients (n = 217), as well as statistical comparisons between eligible patients who did (n = 84) and did not (n = 133) enroll in the PA program. As shown, a greater percentage of enrolled patients had a history of high cholesterol (73.8%) compared to patients who did not enroll (57.9%), χ2 (1, N = 217) = 5.66, p = .02. No other statistically significant differences between patient groups were observed. However, comparisons for distance from each patient’s home to the nearest EIMG PA facility and for type of insurance coverage were trend level (p’s of .08 and .09, respectively).
Characteristics by Enrollment Status Among Patients Who Were Eligible.

Missingness by variable: BMI (n = 2); Marital status (n = 4); CCI (n = 22); all environmental characteristics (n = 1).
Source, US Census data from patient zip code in 2000.
Qualitative Results (Study Aim 2)
Aim 2 sought to enhance and deepen understanding of reasons why patients did not enroll in the PA program through qualitative interviews. As shown in Figure 1b, 139 patients were initially contacted for interviews. Upon later review, 6 of these individuals were determined to be ineligible for the study (eg, EIMG referral not placed from 1 of the 12 pre-identified clinics). As a result, although 28 interviews were completed, 1 was excluded due to ineligibility and another was unable to be analyzed due to poor recording quality, leaving 26 interviews for analysis. Twenty-three (88.5%) interviewed patients were female. Interviewed patients came from 8 of the 12 referring clinics (see Supplemental File 5). The mean interview duration was 22.2 min (SD = 8.0).
Three major themes emerged from the interviews: (1) positive referral experiences with opportunity for enhanced initial information sharing and improved flow; (2) strong patient motivation, perceived capability, and social support; and (3) external barriers preventing enrollment. Details are provided below. Supplemental File 6 provides example quotes.
Theme 1: Positive referral experience with opportunity for enhanced information sharing and flow
For context, all referrals were placed by patients’ primary care physician. The process was usually initiated by the provider, although a few patients inquired about EIMG after seeing a poster or brochure in the clinic.
Most patients reported having positive interpersonal interactions across the referral phases. Beginning with their experience in the clinic (step 1), most patients reported having a good relationship with the referring provider and felt that the provider listened to their concerns, was informative, and problem-solving oriented. When asked about the motivation that they received from their provider to enroll in the PA program, most felt encouraged but not pressured; no patients reported that the interaction with their provider negatively affected their motivation level. Patients reported high amounts of trust in their provider’s advice, stating that their providers had their best interest at heart and were knowledgeable about appropriate recommendations for improving their health. A few patients shared that they took their provider’s advice into consideration, but also liked to research the recommendations themselves. Overall, patients appreciated the referral, felt that their provider cared, liked the general tone of the interaction, and were happy to receive another strategy to improve their health.
Patients who proceeded to step 2 and 3 in the enrollment process reported similarly positive interactions in these later phases. Most patients reported having a positive interaction with the EIMG Care Coordinator during the follow-up call (step 2). While some individuals felt extremely encouraged to enroll in the program specifically due to their interaction with the EIMG Care Coordinator, the majority felt the interaction itself did not directly affect their motivation levels, but rather was an effective way to learn more details about the program (eg, location, times, and cost) and how to enroll. Similarly, those who decided to attend the PA program orientation (step 3), but ultimately did not enroll, felt that the facility staff were informative, reassuring, encouraging, and helpful. Thus, the interpersonal interactions throughout the enrollment process were overall positive and not a barrier to enrolling.
With regard to the type and amount of information shared at each phase, patients had more mixed experiences, particularly during the initial encounter. The type of information received from the provider in-clinic (step 1) varied but included information about the health benefits of EIMG and details of the PA program (eg, locations, cost, and class times). For the amount of information received, most patients felt the information provided was brief and high-level; very few reported receiving comprehensive, in-depth information on EIMG by their primary care provider. Some patients were satisfied with this limited amount of information, but others thought it was not detailed enough and needed more information for them to make an enrollment decision. Similar themes were observed for perceptions of the information received during the follow-up call (step 2). Most patients felt that the program details were well explained and were generally satisfied with the quality of information received from the EIMG Care Coordinator, while a few patients wanted more details. Those who attended an orientation (step 3) reported being satisfied with the amount and quality of information received at that phase in the process.
Patients were divided when discussing the continuity of the overall referral process. Approximately half reported that the process went smoothly and as planned; the rest stated that they experienced systemic issues (eg, long wait time for follow-up, missing forms that they needed to sign) that slowed down the referral process. After the referral was placed, most patients reported receiving follow-up calls from the EIMG Care Coordinator, while 3 reported no follow up communication or needing to inquire further themselves. The patients who went to the initial PA program orientation, but ultimately did not enroll, felt that the enrollment process was smooth, easy to understand, and required them to do little.
When asked about suggestions for ways to improve the referral process, patients shared that they wanted more information about the PA program from their provider in the clinic and suggested that the information be made available both via hard copy and electronically. Patients also recommended more frequent follow-up by the referral coordinator after missed contacts, using different modes of communication (ie, email, text message, or messaging in the patient portal rather than just phone communication), and having clinics confirm that patients were connected with the EIMG Care Coordinator after the referral was placed.
Theme 2: Strong patient motivation, perceived capability, and social opportunity
Nearly all patients reported being excited about and interested in the PA program. When asked why they received an EIMG referral, most patients felt that it was for weight loss, either alone or in conjunction with management of a chronic condition (eg, diabetes, hypertension, musculoskeletal pain). A few patients specifically mentioned that they felt they received the referral as an alternative to anti-obesity medication or metabolic and bariatric surgery. Several patients reported that they felt the program was a way to become active and exercise more frequently, making no mention of health or weight. Most patients stated they were very motivated to increase their PA levels and to join the program, citing anticipated benefits that aligned with their perceived reasons for referral, such as losing weight, improving their overall health, and gaining encouragement and knowledge from the PA program staff.
Most patients also reported feeling comfortable exercising, both physically and psychologically. However, some brought up concerns, such as anxiety about exercising around others or, conversely, not feeling safe exercising alone due to their health issues. While many patients reported having some physical limitations (eg, musculoskeletal pain, weakness, and fatigue), almost none felt that these limitations would have prevented them from joining the program with the proper exercise modifications.
Regarding social considerations, patients perceived several benefits of the small group format of the PA program, including a positive group dynamic to increase motivation and comradery. Disadvantages of the small group format were also noted, including lack of individualized attention and goal setting. About half of patients noted that they had not told any family or friends about the referral. Most patients who had shared about the program felt that their family and friends were supportive and encouraging of them joining. A few patients felt that a stronger support system might have helped them overcome barriers preventing them from joining (eg, finances and transportation).
Thus, for the vast majority of patients, motivation and perceived physical and psychological ability to perform PA and participate in the program were high. Social opportunity (ie, cues and norms that can encourage or discourage behavior) was more varied, although most patients had positive views of social aspects of the program itself and reported at least some encouragement from family or friends if they had told them about the program.
Theme 3. External barriers preventing enrollment
Although most individuals were interested in enrolling in the PA program and felt motivated and capable, a majority cited external barriers that ultimately prevented them from joining. About half reported that the cost of the PA program and/or the lack of insurance coverage was the main reason they did not join. Several individuals stated that they did not have discretionary funds to pay for the program even with financial assistance, while others were unaware of this resource or they had assumed it would not be sufficient, without reaching out to apply for financial aid. Other patients reported that the PA program session times, their work schedules, and other responsibilities prevented them from joining. Balancing their personal and professional schedules with the timing of the program sessions was a challenge for many individuals; even for patients who did not report time as being the primary reason for not enrolling, it was still mentioned as a consideration. Although lack of transportation to the PA facility was not reported as a major barrier, approximately half of the patients mentioned that the location of the PA facility was too far and played a role in their decision to not enroll. Although all PA facilities were following the US Centers for Disease Control and Prevention guidelines of operating safely during the COVID-19 pandemic (when facilities were reopened March 2021), 3 patients still cited concerns around fear of contracting COVID-19 as their main reason for not joining.
When asked for ways to reduce barriers to enrolling in the PA program, patients recommended lowering the program cost, having more PA facilities to increase the likelihood one would be more convenient, and adding more session times to accommodate personal and work schedules. When asked for overall feedback, most individuals reported that their overall experience receiving the EIMG referral was good, and they thought it was a great program.
Discussion
EIMG is a unique clinic-to-community model that aims to connect eligible patients seen in clinical settings with an evidence-informed, community-based PA program. This study sought to understand factors that impact whether patients who are referred to the PA program enroll to both improve the EIMG model itself and to inform efforts to create similar, effective clinic-to-community linkages in other US healthcare systems. Influences on enrollment decisions were assessed using both quantitative (Aim 1) and qualitative (Aim 2) approaches. Results for Aim 1 revealed few differences between patients on variables from the EHR. This highlights the difficulty of predicting who will enroll in a community-based program based on these more static factors. Findings from the follow-up interviews (Aim 2) suggested that logistical factors, such as finances, time, and location, presented the greatest barriers to enrollment. Concrete ways that the enrollment process could be bolstered to potentially increase engagement were also identified.
Enrollment status was unrelated to most sociodemographic, patient health, health care utilization, and neighborhood variables assessed in this study. This pattern of findings diverges from prior literature on exercise referral schemes, which generally found that females and older individuals were more likely to follow through on provider referrals to community-based PA resources.14,20 It is possible that specific features of the EIMG model helped engage a higher proportion of males and younger individuals than seen in some prior programs with diverse referral pathways and PA resources. For example, the fact that patients’ received an in-person referral from their regular provider may have encouraged patients to enroll. 15 Referral to a structured PA program at a known facility (eg, the YMCA), rather than referral to a less known PA resource like behavioral counseling, may also have made the PA program more appealing to a broad audience. Since both the eligible and enrolled samples were predominantly female and middle- to older-aged, it is also possible that this study’s more homogenous (and limited) sample impacted findings.
The one significant difference that was detected between enrollees and non-enrollees in the quantitative comparisons was for history of hyperlipidemia. Prior research has found inconsistent evidence as to the impact of medical history on enrollment in provider-referred, community-based PA programs.14,19 Our findings add to this mixed body of literature. In addition, while differences between enrollees and non-enrollees on distance to the nearest PA facility and type of insurance coverage did not reach statistical significance, these comparisons were trend level and potentially of a clinically meaningful magnitude; on average, non-enrollees lived about 4 times as far from the nearest EIMG PA facility, and only 31% of non-enrollees (vs 45% of enrollees) had commercial insurance. Given that these differences were not pronounced enough to reach statistical significance, these findings must be interpreted cautiously. However, these observations lend credence to the qualitative findings, discussed below, and should be further investigated in future studies with larger samples.
While EHR data provided limited insights into factors associated with enrollment, qualitative interview data highlighted several reasons why patients did not enroll. Key among these were finances, time or scheduling constraints, and location considerations. These top barriers closely align with findings from several prior studies on enrollment in physician-referred PA programs.15,17,18 It is interesting that cost was cited as a major barrier to enrollment, despite existence of a robust financial assistance program (up to 90% of the program cost waived and/or enrollment for as little as $25 for the entire 12-week PA program, which included full YMCA membership and child care at some locations). Interview data indicated that several patients were not fully aware of or did not fully understand the available financial aid options; this likely contributed to cost being cited as a barrier. The frequency at which cost was cited as a concern despite the availability of financial aid also highlights the importance of patient perceptions in understanding barriers. While a fee of $25 (or more in some cases) may seem workable for one person, it may feel untenable for the next, especially when factoring in additional costs of participation such as transportation. Similarly, as indicated in a number of quotes (see Supplemental File 6), what is seen as a workable distance to the PA facility for one person may differ from what is workable for the next. These differences in what is “workable” may also help to explain why the quantitative comparisons for distance to the nearest PA facility and type of health insurance coverage (one indicator of income) fell short of statistical significance despite being raised as common concerns in the interviews.
Consistent with prior literature, interviews also highlighted the value of a positive interpersonal experience with one’s provider15,18 and the perceived ease of the enrollment process. 18 Interestingly, while some prior literature points to motivation as an influence on enrollment,17,18 most interviewed patients in this study stated that they felt motivated to join the program, despite not ultimately doing so. It is possible that both were true: patients felt highly motivated and still did not join due to other reasons. As illustrated in select quotes (see Supplemental File 6), some patients reported initial high motivation that dampened when they realized complexities involved with participating (eg, fitting PA sessions into their schedule). It is also possible that motivation had a more subtle influence on enrollment (eg, participants felt motivated in some regards and less in others), or that motivation was lower than recalled.
Overall, these results point to several potential ways to enhance uptake of PA programs within clinic-to-community referral pathways. First, following patient suggestions, it may be helpful to share detailed information with patients about the PA program at the point of referral. Given the many constraints on providers’ time, there may be creative ways to achieve this. For example, interviewees suggested creating a short video that gives more information about the program that patients could access or that could be sent through the EHR patient portal, having a peer who had completed the program available for Q&As (akin to a patient navigator or peer support model 22 ), or simply having detailed written materials available at the visit or on a website. Other relatively straightforward modifications to the enrollment process could also enhance engagement. These include having the EIMG Care Coordinator follow-up by text message or email in addition to phone, and encouraging providers to follow-up about the referral at subsequent visits to guard against patients getting lost in the enrollment process. Some of these suggestions are already being implemented at Prisma Health in response to these study findings, including the ability to now obtain patient signatures through MyChart if they were not obtained in clinic, reducing the need for the patient to return to clinic and reducing the delay in patient referral to the PA facility.
Aligned with previous suggestions, it may be important for referring providers to know and clearly communicate financial aid resources to patients from the onset to avoid patients erroneously assuming they will not be able to afford the program. EIMG has also recently (post-study) streamlined the financial aid application process. While there are limits to what any one program can provide, it may also be worth exploring scenarios under which full program costs could be covered, and whether the locations and times can be expanded while maintaining program viability. Overall, one take-home message from the data is that providers should continue to refer patients to the program, as even those who did not enroll viewed the referral positively and felt cared for. While research on providers’ decision-making processes around referrals is needed, data also caution against using more static characteristics like those captured in the EHR to try to predict who will ultimately enroll or who should be offered a referral.
Strengths of this study include the mixed-methods design, racially diverse sample, and use of the COM-B model to design the interview guide and interpret the interview data. Limitations should also be acknowledged. For the quantitative analyses, the team was limited to data available in the EHR, which narrowed the potential variables that could be assessed (eg, individual income was unavailable) and resulted in some missing data. The precision of variables within the EHR is also unknown. For example, it is possible that not all existing health conditions were entered into the EHR, and some race and ethnicity data may have been entered based on judgements by the care team or clinic staff rather than self-identified by the individual. 23 For the qualitative analyses, the delay between the time of referral and time of interview, which was due to research funding timelines, may have resulted in recall bias. There could also be systematic bias in who agreed to be interviewed; those who felt most positively about the program have may been more likely to complete an interview. Findings may thus not reflect the experiences of all referred patients. Relatedly, only a portion of potentially eligible patients seen in the clinics were referred to EIMG during the study period; some referred patients were ultimately deemed ineligible; and nearly half of the patients who ultimately agreed to be interviewed were from 1 referring clinic. Multiple factors likely impact who a provider decides to refer (eg, apparent motivation, assumptions about ability to participate, whether the provider has time that day). As referrals are a necessary first step, further research is needed to assess EIMG’s “reach” and optimize providers’ role in connecting patients with the program.
In summary, few differences existed between patients who did and did not enroll in the PA program based on more static characteristics available through the EHR. While most patients reported positive experiences with providers, logistical reasons—namely, cost, time constraints, and location—were the main reasons patients provided for not enrolling. Suggestions for program improvement focused on addressing these barriers, as well as giving more detailed information at the point of referral and modifying the enrollment process to streamline and strengthen the flow. Given the prevalence and burden of chronic diseases in the US, these findings can inform improvements to the EIMG infrastructure and guide the development or refinement of clinic-to-community PA pathways in other healthcare systems.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241306710 – Supplemental material for Factors Influencing Patient Enrollment in a Community-based Physical Activity Program After Healthcare Provider Referral: A Mixed Methods Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241306710 for Factors Influencing Patient Enrollment in a Community-based Physical Activity Program After Healthcare Provider Referral: A Mixed Methods Study by Leah M. Schumacher, Jennifer L. Trilk, Lia K. McNulty, Kelly R. Ylitalo, Stephanie Eskuri, John M. Brooks, Paul A. Estabrooks, Meenu Jindal and Mark Stoutenberg in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to acknowledge Frankie Bennett for his help with the Institutional Review Board submission and the coordination of payment to patients completing the interviews. We would also like to acknowledge Ksenia Power and Samantha Waltrich for their help conducting and analyzing the patient interviews, respectively.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Stoutenberg is a paid consultant by the American College of Sports Medicine for his work with the Exercise is Medicine initiative. All other authors declare that they have no potential or actual conflicts of interest related to this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Duke Endowment [#7058-SP]. LMS received a Loan Repayment Award from the National Heart, Lung, and Blood Institute (L30HL154167). KRY is supported by the National Institute on Aging under the National Institutes of Health under Award Number K01AG058754. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Prisma Health IRB (Reference #:1980721-3).
Consent to Participate
Informed consent was obtained from all individuals who participated in qualitative interviews. Only de-identified data were accessed for quantitative analyses; the IRB determined that informed consent was not required for this aspect of the study.
Consent for Publication
Not applicable
Data Availability Statement
This study was not formally registered. The analysis plan was not formally pre-registered. De-identified data from this study are not available in a public archive. De-identified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author. Analytic code used to conduct the analyses presented in this study are not available in a public archive. They may be available by emailing the corresponding author. Materials used to conduct the study are available in supplemental materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.