
Abstract
Introduction/Objectives:
The cost of medical services is a major barrier to healthcare accessibility for underserved populations in the United States. Community charity medical clinics help address this disparity by providing free or reduced-cost care for the medically underinsured; however, their economic and public health contributions are unknown. The objective of this study was to evaluate the scope of services and monetary impact of 4 community charity medical clinics in North Texas, with one of the largest medically underinsured populations in the United States.
Methods:
A cross-sectional study was conducted using electronic health records from 4 clinics serving adults and children in North Texas. Encounters from June 1 to December 31, 2018 completed by with sufficient documentation to assign a level of service were reviewed. There were 3942 encounters identified and 2148 (54.5%) audited. Centers for Medicare and Medicaid Services Evaluation and Management Standards were used to identify level of service provided for each encounter, and their subsequent value was determined based on CMS fee-for-service schedules at the time service was provided. Common conditions managed during these encounters were identified using ICD-10 codes documented with each encounter.
Results:
The most prevalent diagnoses encountered were hypertension, diabetes, hyperlipidemia, and major depressive disorder. We estimate the total value of services and medications provided for 1 year is between $840 278.30 to $845 737.41.
Conclusions:
The charity clinics in North Texas provide a significant economic impact through a high level of charity care and a broad scope of services for a vulnerable patient population. The results may be used in the development and implementation of future services to meet the needs of the medically underinsured.
Introduction
The United States (US) operates under a complex healthcare system of both public and private insurance with limited regulations and a lack of universal coverage. Because of this, the US has a high prevalence of uninsured or underinsured individuals. In 2018, 23% of the US population reported some degree of inadequate insurance coverage with 12% lacking insurance entirely. 1 As of 2020, Texas had the highest percentage of uninsured individuals (17%) and Dallas County reported 21% of the population was uninsured, which was more than double that of the national average (9%). 2 Furthermore, those who were uninsured reported cost-related delays in getting healthcare (71%) at nearly twice the rate of those who were not underinsured (46%). 3 This disparity in access to care has resulted in worse health outcomes and a greater financial burden on the healthcare system. 4
Charity medical clinics provide free or donation-based care to help patients who are uninsured or unable to pay high costs. In 2010, over 1000 of these clinics provided care in the US for the medically underserved. 5 Over 3.1 million patient encounters occur in these clinics each year, and the majority of patients seen were uninsured, were unable to pay, represented racial or ethnic minority groups, and/or lacked housing. 5 Moreover, 82% utilized volunteer physicians with over 90% supported by individual donations and a yearly mean operating budget of almost $290 000. 5 North Texas is home to several charity clinics, many of which have close partnerships with academic medical centers and serve as training locations for multidisciplinary medical learners to gain service learning experience,6,7 conduct community-based participatory research,8 -10 and provide community responsive care to diverse groups of underpresented patients. For example, medical students at the University of Texas Southwestern Medical School can participate in the Community Action Research Track (CART) program which requires 80 h of service learning over 4 years providing medical and non-medial services to underserved communities. 6 Students have conducted community-based participatory research projects at local homeless shelters and underserved clinics to evaluate knowledge of skin cancer, 11 determine needs of transgender patients, 12 evaluated health literacy levels 13 among many others, along with providing charity care to underserved patients.
Though the services provided likely benefit the community, there is a paucity of data demonstrating how their monetary value impacts the healthcare system. Villa proposed a framework for assessing community benefit in healthcare by focusing on changes in profitability, efficiency, charity care, and bad debt through hospital privatization to justify tax exemption for hospitals. 14 A similar framework for measuring community benefit can be applied to charity clinics as a commonly used component is the provision of free care. In this study, we aim to describe the scope of services and monetary value of 4 North Texas community charity medical clinics to highlight the importance of accessible community healthcare.
Methods
Study Setting and Eligibility
A cross-sectional study was conducted of all patient encounters occurring between June 1, 2018, and December 31, 2018, at the following 4 Dallas community charity clinics: Union Gospel Mission (UGM) Calvert Place; UGM Center of Hope; North Dallas Shared Ministries (NDSM); and Agape Clinic. Patient charts from all clinics were retrospectively identified, extracted, and reviewed through Athenahealth’s electronic health record, AthenaNet. 15 Eligibility criteria included all closed patient encounters with physician assistants and physician visits that occurred during the study period at all clinic sites. Excluded encounters were test patients, nurse visits, and those with missing patient identifiers. A total of 3942 encounters were identified for potential audit and over half (n = 2148; 54.5%) were randomly selected for audit. Seven encounters were removed due to missing documentation for the physical examination. Study size was determined by available resources, and auditor capacity to review and record patient data. Selection bias was mitigated through randomized participant selection utilizing a random number generator.
Data Collection
A group of medical and physician assistant student auditors from a local academic medical center were recruited and trained to collect data from the patient encounters. Students auditors participated in this project in fulfilment of course elective, capstone project, and community-based training program requirements.8 -10 Student auditors were divided into groups based on the clinic site and assigned encounters. Auditors were trained to access and record patient information from AthenaNet according to CMS Evaluation and Management standards. 16
Data collection methods were standardized across clinical sites to minimize observer bias. No patients were contacted directly and no follow-up information was collected from the patients included in the study.
Chart Audit Review Survey
Study auditors reviewed electronic health records of the patients who were seen for an in-person appointment during the specified study period. Data from audited encounters were logged in a survey using the Research Electronic Data Capture (REDCap) survey. 17 The survey included 5 sections: (1) the basics; (2) evaluation of a history of present illness (HPI); (3) evaluation of the exam; (4) evaluation of medical decision making; and (5) evaluation based on time. Survey fields collected data specific to the components of the Centers for Medicare and Medicaid Services (CMS) Evaluation and Management Audit tools. 16
The basics section includes to describe the type of encounter (new or established patient), immunizations (eg, influenza, Tdap, and Pnemmovax), point of care tests (eg, flue text, fecal occult blood, urinalysis, and hemoglobin A1c) provided, and chief complaint. Chief complaints were collected based solely on the designated “chief complaint” section of the patient chart and were then translated into system-based categories (eg, dermatologic, cardiovascular, and musculoskeletal) with the additional categories for “wellness/annual visits” and “other” (eg, lab work and medication refills). The evaluation of HPI section included 4 questions to describe the number of chronic conditions, how many HPI elements were documented, the number of systems evaluated in the review of systems. The evaluation of the exam section included questioned on the level of the exam completed (problem focused, expanded problem focused, detailed, comprehensive) and the number of body area or systems (one body area or system, up to 7 systems, and 8 or more systems). The evaluation of medical decision making section included questions to describe the number of diagnoses or treatment options and a listing of International Classification of Disease, 10th revision (ICD-10) codes, procedure codes, and medications distributed for each encounter. The quantity of medications dispensed was verified, and any medication without a quantity was excluded from the study. These were then categorized based on Food and Drug Administration drug classifications with the following modifications: anti-inflammatory classification was split into 3 separate categories (nonsteroidal anti-inflammatory drugs (NSAIDs), topical corticosteroids, and corticosteroids); cough suppressants and decongestants were included in the cold cures category; and an “other” category was created for medications dispensed fewer than 3 times. 18 This section also included questions to asses the highest level of risk associated with the encounter (minimal, low, moderate, or high) and total for the amount and or complexity of the data reviewed (range 1-9). The evaluation based on time section included 5 questions to describe whether the among of time spent with the patient was documented (yes or no), the documentation described the content of counseling or coordinating care (ues or no) and the time spent during the encounter (range 5-60 min).
Statistical Analysis
Data analysis was conducted using Microsoft Excel and STATA 17.0. 19 Frequencies were reported for chief complaint and medication categories. Prevalence estimates for ICD-10 codes were determined for the most common diagnosis groups, including hypertension (I10, I15, and R03.0), diabetes mellitus (E08-11 and E13), dyslipidemia (E78), and depression (F32-33). Prevalence estimates were determined by consolidating codes for patients with multiple encounters and removing duplicate ICD-10 codes.
The monetary value of medical services was measured based on previous studies that assessed the monetary value of services, level of charity, and scope of care provided.14,20 Procedures and tests were assigned separate values based on CMS reimbursement rates. Vaccines were assigned a range based on the Centers for Disease Control and Prevention (CDC) pricing lists during the time of administration. 21 Pricing from GoodRx and local retailer stores were used to determine the total cost of medications based on quantity dispensed. 22 All monetary values were reported as a 1-year projection from the 7-month study period.
Ethical Approval
This study was approved by the Institutional Review Board at the University of Texas Southwestern Medical Center (#STU-2019-0954). The study was considered exempt based on its used of secondary data that included data recorded by the investigators in such a manner that the identify of the subjects could not readily be ascertained, the investigators did not contact the subjects, and investigators did not make any effort to re-identify subjects after data were collected and de-identified.
Results
There were 3942 patient encounters potentially eligible for the study, and 2148 (54.5%) were randomly selected to be audited to confirm eligibility. Seven encounters were excluded due to missing documentation for the physical examination. The remaining 2141 (54.3%) encounters were then included in the study and analyzed. The average age of patients was 43.3 years (range 1-98). Overall, 64% of patients were female. The most common self-reported races were white (44.8%) and African American or black (19.97%) with 31.33% declining to respond. Most (67.97%) patients identified as Hispanic or Latino. Spanish was the most common language spoken by patients (67.16%). Of the patient encounters with reported federal poverty level (FPL), 79% of patients seen were at or below the FPL. However, data on FPL was missing from 80.6% of patient encounters (Table 1).
Demographic Characteristics of Patients, N = 3918.

Abbreviations: NDSM, North Dallas shared ministries; UGM, Union Gospel Mission.
Of the 2767 chief complaints identified, the most common chief complaint categories were “None” and “Other,” followed by “Dermatologic” and “Cardiovascular” (Table 2). The most frequently occurring documented chief complaints were “Skin problem/rash,” “Hypertension,” and “Diabetes.” The “Other” category largely consisted of “Lab review” (36%), “Medication refill” (15%), and “Follow up (unspecified)” (10.7%; Supplemental Table 1).
Chief Complaint Categories and Top Diagnoses Based on Frequency and Prevalence.
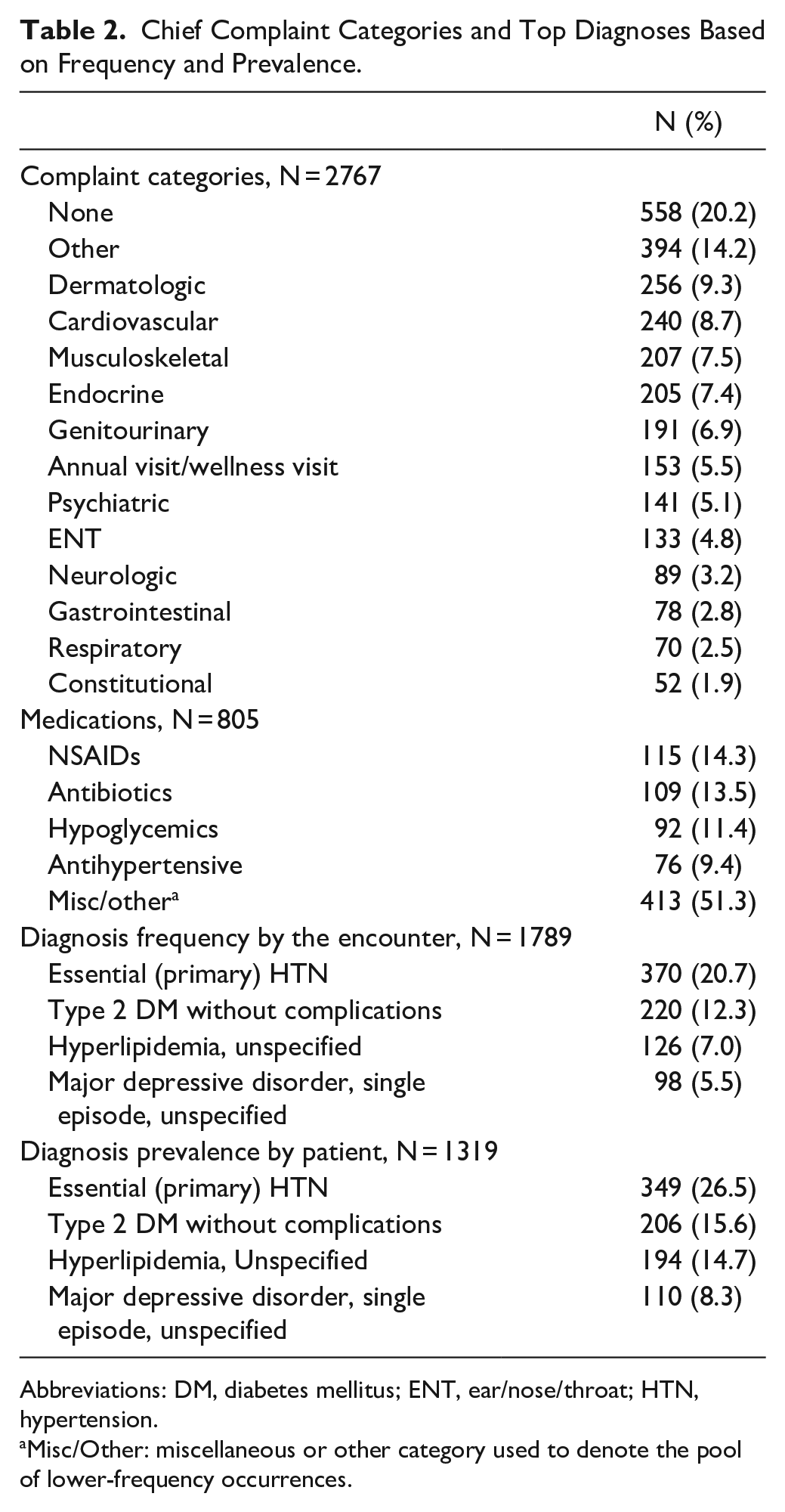
Abbreviations: DM, diabetes mellitus; ENT, ear/nose/throat; HTN, hypertension.
Misc/Other: miscellaneous or other category used to denote the pool of lower-frequency occurrences.
Of 1789 encounters with at least 1 ICD-10 code, a total of 4018 ICD-10 codes and 770 unique codes were found (Supplemental Table 2). The most common ICD-10 codes by encounter were I10 (essential (primary) hypertension; 20.7%), E11.9 (type 2 diabetes mellitus without complications; 12.3%), E78.5 (hyperlipidemia, unspecified; 9.9%), and F32.9 (major depressive disorder, single episode, unspecified; 7.0%; Table 2). There were 26.5% of patients with essential hypertension, 15.6% of patients with type 2 diabetes mellitus, 14.7% of patients with hyperlipidemia, and 8.3% with major depressive disorder (Table 2).
There were 77 encounters with documentation of at least 1 vaccine administration. During these encounters, 94 vaccines were documented primarily including influenza, pneumovax, tetanus, diphtheria, acellular pertussis, and human papillomavirus (Table 3). There were 495 encounters with 654 point-of-care tests identified through the chart audits (Supplemental Table 3). The most common point-of-care tests included finger stick glucose, HgbA1c, and urinalysis (Table 3). There were 7 encounters associated with procedures. There were 533 encounters identified with at least 1 dispensed medication. There were 855 medications verified as dispensed, of which 42 were excluded for missing quantity documentation. The remaining 813 medications were sorted by category and assigned a cost. The most common medications dispensed were NSAIDs, antibiotics, hypoglycemics, and antihypertensives (Table 2).
Level of Service, Vaccines Administered, and Point-of-care Tests Completed.

Abbreviations: Glu, glucose; Hgb A1c, hemoglobin A1c (glycated hemoglobin); HPV, human papillomavirus; Misc/Other, miscellaneous or other category used to denote the pool of lower-frequency occurrences; NDSM, North Dallas Shard Mission.; POC, Point-of-care; TDaP, Tetanus, diptheria, acellular pertussis; UA, urinalysis; UGM, Union Gospel Mission.
Percentages of vaccines administered refers to the proportion of vaccines administered by the charity clinic.
In total, 1473 unique patients were identified with 615 new patient encounters and 1533 established patient encounters. The average level of service for these encounters was 2.69 (1.55 for new patients, 3.15 for established). Based on the distribution of Healthcare Common Procedure Coding System (HCPCS) codes and CMS reimbursement rates, the estimated level of service monetary value provided was $160 661.23 (Supplemental Table 4). The value of vaccines administered, based on the CDC pricing from the time of administration, ranged from $2913.29 to $4906.74 (Supplemental Table 5). The value of the tests and procedures provided according to the current procedural terminology (CPT) and HCPCS codes and CMS reimbursement rates was $5257.20 and $339.08, respectively (Supplemental Table 4). The total cost of medications for these encounters was estimated to be $93 650.15 based on costs reported by GoodRx and local retailers at the time medications were distributed (Supplemental Table 6). The estimated monetary value of all services provided from June 1st to December 31st, 2018 was $262 820.95 to $254 814.40 and the 1-year scaled estimated value was $840 278.30 to $845 737.41 (Table 4).
Level of Charity Based on the Monetary Value of Services.
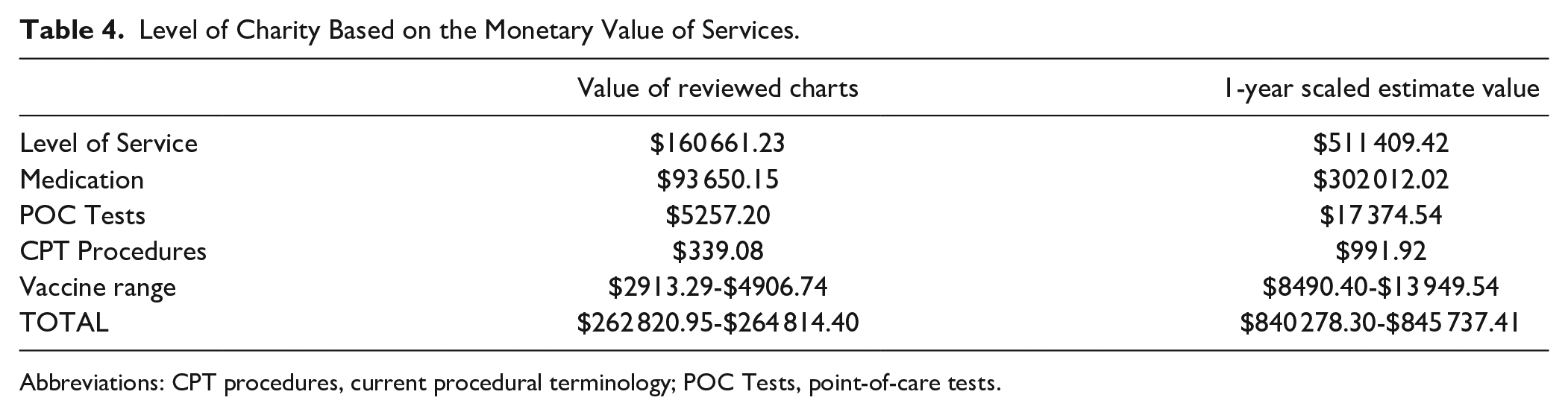
Abbreviations: CPT procedures, current procedural terminology; POC Tests, point-of-care tests.
Discussion
Finding both accessible and affordable healthcare is a significant barrier that many uninsured individuals in the US face and often leads to delayed care, disease progression, and worse health outcomes. 4 As a result, many individuals first present when emergency medical intervention is required, which increases the overall economic burden on the healthcare system compared to if early intervention had occurred. 23 Charity clinics offer a solution to delayed access to care by granting these individuals an alternative option for long-term management of disease. However, the monetary value of such services has yet to be quantified in a meaningful way on the national level or in local communities. In Dallas, community clinics provide services otherwise unattainable to the vulnerable and impoverished population they serve. Through analysis of the services the 4 clinics provide, we estimated the monetary value ranged from $840 278.30 to $845 737.41 over a 1-year period for the healthcare system in 2018. With a 13.28% increase in the consumer price index for medical care cost since 2018 reported by the US Bureau of Labor, this value would be equivalent to $951 867.26 to $958 051.34 in 2023. 24
Our findings demonstrate that the scope of services provided in charity medical clinics is broad. It is estimated these clinics served 4767 unique patients over a 1-year period and hosted 6792 physician and physician-assistant encounters, documenting 770 unique diagnoses. During these encounters, a wide variety of services were available including 11 different tests, 7 unique immunizations, and over 18 categories of medications. The wide scope of services provided by these clinics is also highlighted by the variety of chief complaints and diagnoses documented. Diagnoses were consistent with other community-free clinics across the US. 25 However, the prevalence rate of hypertension (26.5%) and depression (8.3%) were lower than the national average rate for both low-income individuals and the general population.26 -28 The prevalence of hyperlipidemia (14.7%), however, was similar to that of the general population (11.4%) but significantly lower than low-income populations (23.5%). In contrast, the prevalence of type 2 diabetes mellitus (15.6%) was almost identical to that published by He et al 26 for low-income populations. These discrepancies could be attributed to the fact that our patients are specifically being served at a charity clinic, which has dramatic differences in cost and capacity of care compared to public and private facilities. Thus, while charity clinics serve a unique role in providing chronic disease management to underinsured populations, further work needs to be done to refine our understanding of how this specific population may be different from the general population to better meet their healthcare needs.
Furthermore, the findings from this study complement the results identified by Hua et al, 20 which demonstrated the significant monetary value of a student-run podiatry-free medical clinic. While Hua et al 20 identified the significant value of specialty services, this study adds that charity medical clinics also have a substantial impact through providing primary care services. In 2014, 208 charity clinics were collaborating with students to provide care across the U.S., providing outpatient care with similar health conditions to our study population. 29 As many of these clinics are providing reduced-cost care similar to what is presented in this study, the value of such services demonstrates significant cost savings for the public healthcare system as a whole.
Success in managing chronic diseases is largely dependent on medication adherence and is known to significantly decrease hospitalization rates for patients with diabetes, hypertension, hypercholesterolemia, and congestive heart failure. 30 However, among the top reported reasons for medication nonadherence are medication cost, lack of transportation, and health insurance status, all of which disproportionately affect the population in this study. 31 Yet, improving the adherence of patients with diabetes could result in annual savings of over $600 million and represent 700 000 fewer emergency department visits per year, saving a further $4.7 billion. 32 Free clinics provide a unique avenue to address this need by reducing the strain of such obstacles to healthcare that underserved individuals face.
The fragmented care for uninsured patients due to foregoing primary and preventative care services results in a lack of patient-physician relationships and significantly increased emergency department utilization. 33 In 2018, Texas had the highest uninsured rate nationally with Dallas County having one of the highest in the state at 24%. 34 By charity medical clinics providing care to the uninsured population, the financial strain placed on safety-net hospital systems is offset as shown by other free clinic models. 35 Overall, this approach helps improve the health outcomes of the uninsured population and contributes to the overall efficiency and effectiveness of the healthcare system.
Limitations
While this study adds significantly to the discussion on the community impact of charity medical clinics, there were limitations. One limitation of this project is its focus on encounters associated with documentation by either a physician or physician assistant. Many of the participating clinics also rely on nurse visits to conduct services that are not reimbursable based on the level of service, such as providing eyeglasses and hypertension screenings. Our methodology focused on identifying reimbursable services and was not designed to capture these nursing visits, but this may have resulted in understating the monetary value of services provided by these clinics. Additionally, clinic documentation was not consistent between providers or clinic sites. As the participating clinics are charity clinics, their intention for documentation was for medical history purposes and not to bill for services. Therefore, the documented information may underrepresent the quality and value of services provided.
Conclusions
To our knowledge, our unique contribution to the literature is the first cross-sectional study to address the substantial impact of charity medical clinics by assessing their scope of services and monetary value of services provided by health care providers to the communities they serve. This study highlights the importance of charity clinics to urban communities with high numbers of uninsured, underserved, and minoritized populations. Future studies can go beyond this work by estimating and making comparisons to the monetary value of services provided by all health care providers in our area, the state, and nationwide. Moreover, future studies should examine the impact of these services to individuals and families. In conclusion, our results provide evidence for further support for charity medical clinics through partnerships with academic medical centers, local religious and governmental organizations, and philanthropists.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241304143 – Supplemental material for Evaluating the Scope of Services and Monetary Impact of Charity Medical Clinics in North Texas
Supplemental material, sj-docx-1-jpc-10.1177_21501319241304143 for Evaluating the Scope of Services and Monetary Impact of Charity Medical Clinics in North Texas by Logan G. Mills, Barbara Newsom, Abigail Lewis, Alexandra Pottorff, Ashley Wallace Wu, Erika Castro, Kelsi Morgan, Lawrence Wu, Bau P. Tran, Katherine Lake, Mina Guirguis, James M. Wagner, Nora Gimpel and Tiffany B. Kindratt in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank all faculty, staff, managers, and students who have contributed to the student-run free clinics. Additionally, the authors would like to acknowledge Patti Pagels, Emily Worthington, Chiamaka Onuigbo, Cory Smith, Hiep Phan, and Venetia Orcutt for their assistance in the research presented. This project has been made possible through our strong partnership between our academic institution and many community organizations in North Texas.
Anonymized Information
Community Charity clinic sites included Union Gospel Mission (UGM) Calvert Place; UGM Center of Hope; North Dallas Shared Ministries (NDSM); and Agape Clinic. This study was approved by the Institutional Review Board at UT Southwestern Medical Center (#STU-2019-0954).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. The University of Texas System has an agreement with Sage to publish gold access articles free of charge through 2025.
Data Availability
Data will be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.