
Abstract
Introduction
Community-based student-run free clinics (SRCs) can advance health on a community level by reaching populations not served by other organizations and serving as an access point to the healthcare system. However, little is known about the scope of community-engaged efforts undertaken by SRCs, including interorganizational partnerships and relationship-building activities. The primary objective of this study was to characterize the community collaborations of an interprofessional SRC located in a high-poverty area.
Methods
Qualitative data was collected through semi-structured interviews with key stakeholders, which included student volunteers holding leadership roles, representatives of community-based organizations, and current and former members of the community advisory board.
Results
Key informant interviews with student and community leaders offered insight into local community outreach activities and the community advisory board. Findings revealed opportunities to impact community health through more intentional collaboration and relationship-building.
Conclusions
This exploratory study adds to literature suggesting that community-based SRCs can address service gaps in medically underserved communities while advancing community health through intentional community engagement.
Keywords
Introduction
There is substantial evidence that addressing societal inequities is necessary to improve health outcomes. Community engagement is defined by the Centers for Disease Control and Prevention (CDC) as “the process of working collaboratively with groups of people who are affiliated by geographic proximity, special interest, or similar situations with respect to issues affecting their well-being.” 1 The goals of community engagement include building trust, enlisting new resources and allies, creating better communication, and improving overall health outcomes as successful projects evolve into lasting collaborations.2,3 A meta-analysis of community engagement interventions showed their positive impact on a range of health outcomes. 4 Among the interventions that can advance health on a community level, community-based student-run free clinics (SRCs) engaged in authentic community collaborations may contribute to improved health outcomes in high-poverty neighborhoods.
Student-run free clinics are important sites for service-learning, as they have been shown to shape health professional students’ understanding of uneven access to health care and resultant disparities.5,6 However, SRCs are often helmed by health professional students who may not elicit community perspectives to guide programs and services. Encouragingly, newer SRCs are being developed in response to community needs assessments and community-identified priorities,7,8 but there remains a notable gap in the literature with respect to characterizing how SRCs collaborate with their local communities. This is an important area of inquiry given the limited services volunteer-led clinics can provide. A comprehensive study of SRC characteristics showed that more than 95% of SRCs had a location other than a medical school or hospital, 9 which suggests these clinics rely heavily on community partnerships. However, only one study to date has focused on how interorganizational partnerships increase the ability of free clinics to address socioeconomic factors. 10
The Phillips Neighborhood Clinic (PNC), located in the Phillips community of South Minneapolis, is the largest interprofessional student-led organization at the University of Minnesota, with more than 400 students from 13 professional programs volunteering each year. The health professionals who supervise the students come from multiple healthcare organizations in the surrounding communities. The clinic is managed by a student board and 2 co-chairs and overseen by a medical director. The clinic provides free primary, specialty, and acute care; pharmacy and laboratory services; health education; insurance enrollment; and referrals to external organizations. Founded in 2003, the clinic operated as a satellite clinic of the University of Minnesota’s Community University Health Care Center, a federally qualified health center, until 2006. In early 2007, the clinic transitioned to a joint partnership between the University of Minnesota Physicians and University of Minnesota Medical School. This joint partnership funds 5% of the medical director’s salary, provides an electronic health record and the technology to support it (laptops and internet access) and consultation for specialized administrative support such as risk management, infection prevention, and contract negotiation. The PNC moved to its current location in the church basement of St. Paul’s Evangelical Lutheran Church in 2014.
Community engagement has been an important component of the PNC since its inception. The physician who founded the PNC anchored his efforts in a community needs assessment of unstably housed individuals in the Phillips community. The early years of the clinic were bolstered by a partnership with a federally qualified health center, alongside persistent challenges with finding a sustainable clinic site and consistent sources of funding. In light of these challenges, the clinic closed in December 2006 while transitioning to a new organizational structure. Reopening 6 months later, the PNC reestablished its presence in the neighborhood by expanding outreach efforts through partnerships with community organizations. All student volunteers now participate in community outreach activities with 7 to 10 partner organizations as part of their volunteer role, spending at least 6 hours per academic semester at various community sites. The clinic also created a community advisory board (CAB) in 2012 to engage key stakeholders and help guide operational decision-making. Anecdotal feedback suggested that student and community interest in the CAB has waxed and waned over the years, largely owing to rapid turnover of student volunteers.
The Phillips community, which spans 3 zip codes and was subdivided into 4 smaller neighborhoods between 2002 and 2005, has the second highest poverty rate in Minneapolis (48%) in part due to a legacy of residential segregation and environmental racism. 11 The East Phillips neighborhood, the lowest-income neighborhood in Minneapolis, was declared a “federal residential arsenic superfund site” in 2000. 12 People of color and indigenous people make up almost four-fifths of the population of the Phillips community, which is significantly higher than the city’s overall demographic distribution. 11 The patient population served by the PNC is demographically similar to the Phillips community, although nearly three-quarters of the 900 to 1000 patients seen in 2016 and 2017 reported an address outside of the 3 zip codes comprising the Phillips community (Table 1). Prior surveys of patients have asked how they found out about the clinic, and the majority stated it was through an internet search. The PNC is one of the first to show up when searching online for a free clinic in the area.
Self-Reported Zip Code of PNC Patients. +
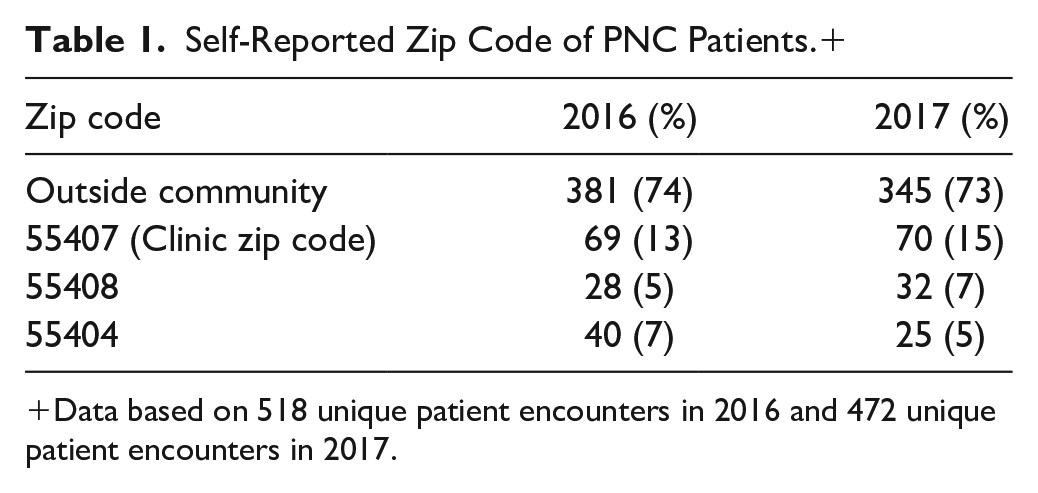
Data based on 518 unique patient encounters in 2016 and 472 unique patient encounters in 2017.
The PNC has a mission statement that includes “supporting community partnerships and promoting overall health and well-being in the communities [served].” The purpose of this qualitative study was to characterize the PNC’s community collaborations, understand neighborhood organizations’ perceptions of the role of the PNC in the community and its impact, and gather recommendations for community collaborations that would advance community health. This study was intended to address a gap in the literature by characterizing how one SRC sought to engage meaningfully with its local community.
Methods
Study Design
To characterize PNC’s approach to community collaboration, an exploratory, descriptive, qualitative study with key informants was conducted. Considering the diverse areas of expertise of key informants, individual semi-structured interviews were chosen to explore their perspectives in depth. Interviews were conducted in person or via telephone between March and June 2018. Each interview took approximately 30 to 45 minutes. All informants were given an information sheet, which explained the goals of the project and provided the informant with written assurance of confidentiality. All interviewees consented to being audiotaped and their interviews transcribed. The Institutional Review Board (IRB) of the University of Minnesota exempted this project from full review.
Participants
The authors identified initial key informants, and additional interviewees were identified with a snowball sampling technique. Inclusion criteria for PNC student informants were holding a current or past co-chair position or holding a current leadership position related to community outreach or engagement. Inclusion criteria for community informants were holding a role in a health or nonprofit organization in the Phillips community that afforded them knowledge of community assets and needs, or serving as a current or former member of the CAB.
Analysis
Interview responses were de-identified and transcribed within a week of the interview. The authors independently read quotes and identified and coded content patterns. Coding was iterative, beginning with an initial list of inductive codes drawn from the data-rich transcripts. As analysis progressed, quotes were compared with others similarly coded and codes were categorized into themes. Themes were identified if supported by at least 2 quotes. Analysis was conducted without the use of data analysis software.
Results
A total of 22 key informants were interviewed within the time frame of the study. Student informants were affiliated with pharmacy (7), public health (2), and medicine (1) graduate degree programs at the University of Minnesota. Community key informants were affiliated with community-based organizations (5) and healthcare delivery organizations (5). Two community informants were current or former members of the CAB. While one goal of key informant interviews was to gather perceptions of the PNC’s community impact, it was found that “impact” was an unfamiliar concept to most informants. Impact was clarified during the interview as the net effect of activities or actions on the surrounding community, including longer-term changes. The entirety of informants’ interview transcripts afforded insight into a new way of framing their responses. This approach aligns with inductive thematic analysis, 13 in which the data itself is used to derive the structure of analysis. From this process, the following 3 themes emerged with multiple subthemes: (1) perceptions of community outreach; (2) perceptions of the CAB; and (3) recommendations for advancing health on a community level.
Perceptions of Community Outreach
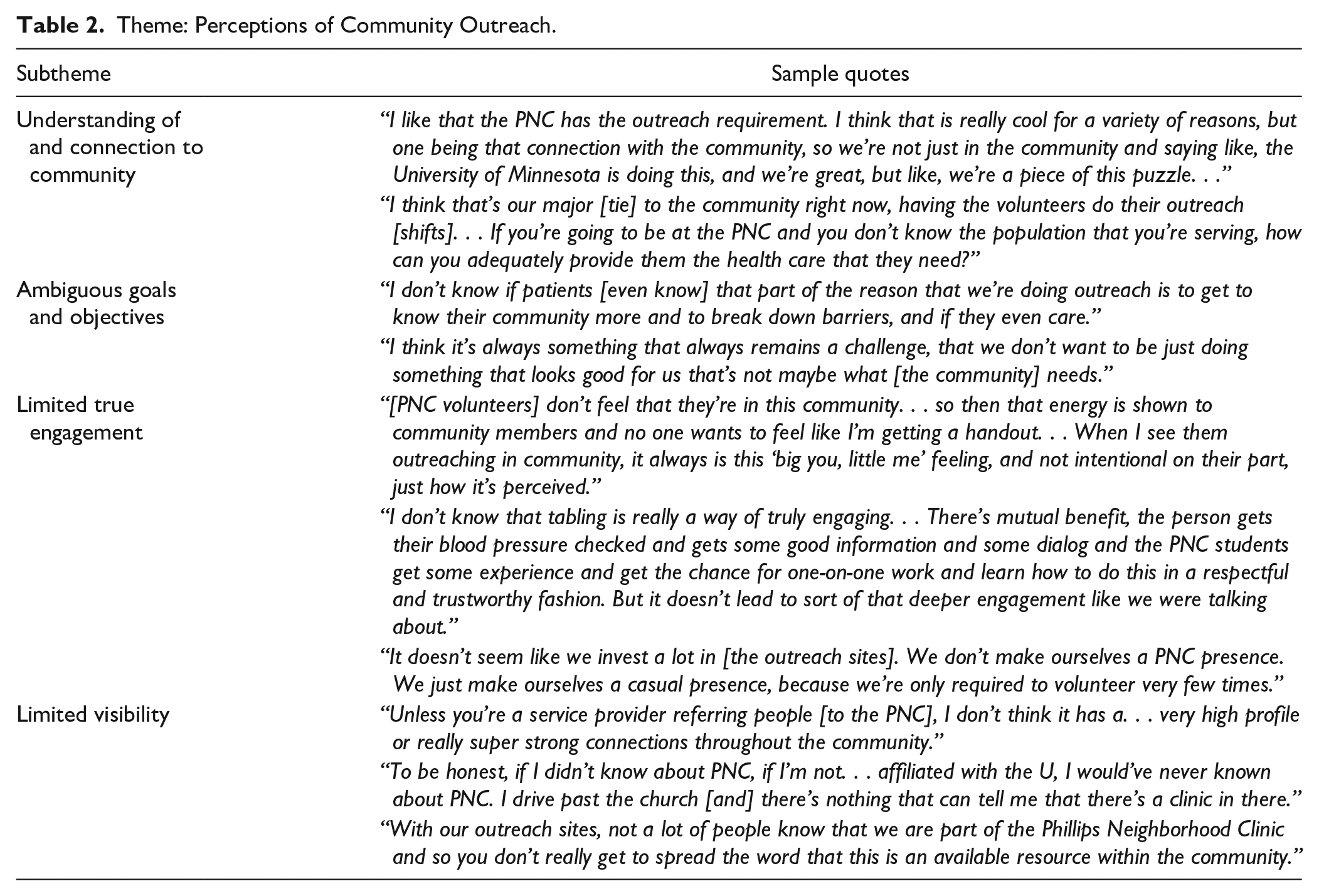
Informants’ perceptions of the community outreach activities were categorized into 5 subthemes as shown with representative quotes in Table 2. Many student interviewees emphasized that community outreach activities allow students to become familiar with the neighborhood and context of care for patients seen at the clinic. However, both student and community informants noted persistent challenges with ensuring outreach activities promote authentic community engagement and establish the clinic’s presence in the neighborhood.
Theme: Perceptions of Community Outreach.
Perceptions of the Community Advisory Board
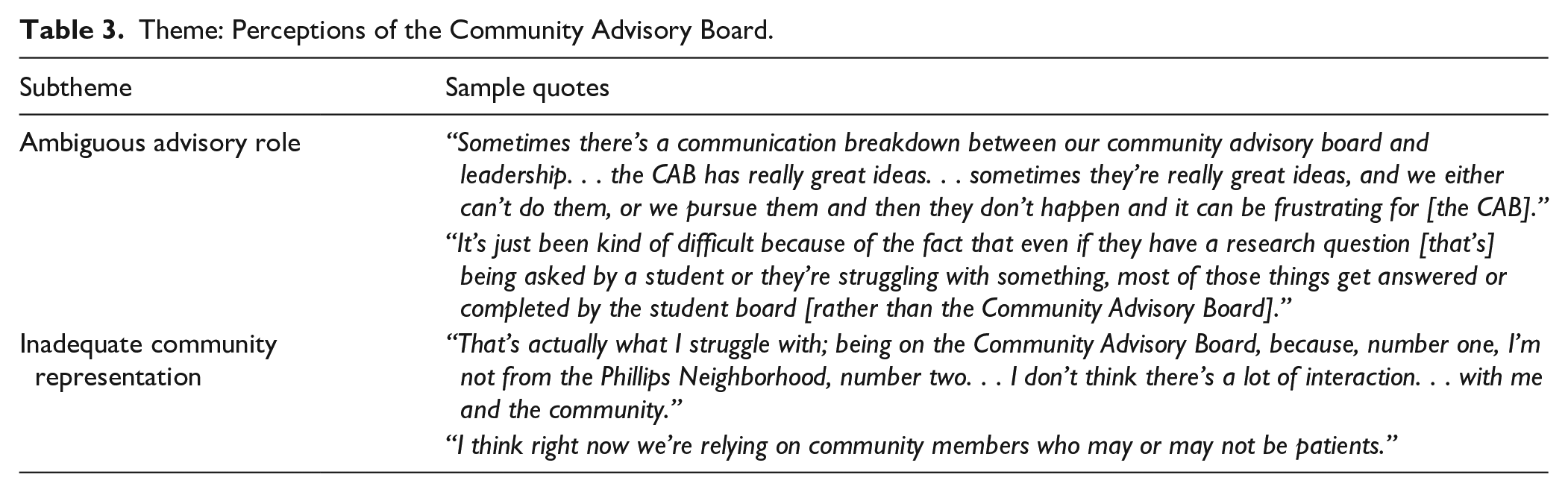
Two subthemes emerged from the informants’ perceptions of the CAB with representative comments shown in Table 3. Student informants talked mainly about the challenges faced in building a CAB with a meaningful advisory role and that was representative of both patients and the community. One informant who had served in the highest tier of student leadership said, “The CAB has always been like a dream that we’ve been working toward.” Community informants with current or past experience serving on the CAB echoed these challenges. Many student informants said they were unsure of who comprised the CAB or mentioned members who were no longer active. One student informant was unaware of the CAB altogether.
Theme: Perceptions of the Community Advisory Board.
Recommendations for Advancing Community Health
All key informants were eager to share recommendations for fulfilling the clinic’s mission of supporting community partnerships and promoting health on a community level. Within these recommendations were 6 subthemes, which are shown with representative quotes in Table 4. Many community informants emphasized the importance of maintaining a clearly defined and feasible scope. One community informant commented, “I’m not sure [the community] looks at the PNC and [says], oh, we want them to run a garden, or we want them to run exercise programs. . . I need some place to really focus on to get health care and when I go there, I want to be treated with respect. And so I think that if the PNC can do that well, then you’re meeting a huge need in the community.”
Theme: Recommendations for Community Collaborations That Advance Community Health.

Discussion
Student-run free clinics often operate in well-known neighborhood locations such as churches, community centers, and primary health clinics, and are therefore well-positioned to meaningfully engage with the communities they serve. However, SRCs are frequently founded and managed by health professional students, who may be unfamiliar with the history of a community and not equipped with strategic planning tools that focus on health from the community perspective. Students may therefore implement programs or services that primarily benefit learners and do not address community-identified needs. Emerging models in medical education, such as structural competency, may address how symptoms, clinical problems, diseases, and attitudes toward patients, populations, and health systems are influenced by “upstream” social determinants of health. 14
The extent to which SRCs collaborate with their local communities has not been described in the literature, although this does not imply SRCs are not involved in their communities. Existing studies describe SRCs engaging in community outreach to advertise services and reach populations not served by other organizations.15,16 Many SRCs likely rely on both formal and informal community partnerships as extensions of their limited services. In addition, there may be variability in whether a clinic’s “community” is defined as the neighborhood where it is located or as the patients who utilize its services. The PNC, for example, primarily serves patients whose zip codes come from outside of the Phillips community. Despite these considerations, a strategic approach to community collaboration appears to be lacking. The CDC framework suggests community engagement should be understood as a continuum with outreach as an initial touchpoint and shared leadership as the final stage of involvement (Figure 1). 1

Community engagement continuum (CDC, 2011).
We sought to characterize the PNC’s community collaborations, understand neighborhood organizations’ perceptions of the role of the PNC in the community and its impact, and gather recommendations for community-engaged efforts. This investigation revealed that the PNC’s community collaborations have fallen short of moving the relationship with the community further down a continuum of engagement. Many informants were unsure or doubtful that outreach activities were meeting a direct need in the community, increasing the clinic’s visibility, or contributing to broader change efforts. Informants also expressed concern about requiring volunteers to participate in community outreach, noting that it was often viewed as a task to be completed, rather than a learning opportunity. The recommendations shared by key informants in this study are echoed in previous SRC literature on community engagement, notably improving data collection and reporting, developing robust evaluation mechanisms, and strengthening community partnerships.17,18
Previous literature has also emphasized that having patients or community members actively involved in SRCs helps ensure that patient perspectives are not overlooked. 19 These findings highlight the need for a clearly defined role for the CAB in decision-making for the clinic, while ensuring that the CAB represents both patients who come to the clinic and the neighborhood in which the clinic is embedded. The challenges expressed by PNC informants related to the CAB are echoed in literature about creating advisory structures for clinical research activities.20,21 Successful practices of CABs in other settings include authentic power-sharing, mutually beneficial partnerships, and bidirectional learning.22-24 The CAB of Widener University’s Chester Community Physical Therapy Clinic is comprised of former patients who relay information to community peers who may need services in the future. 25
Since this study, the student leading the CAB reorganized and improved its engagement with the PNC. The student recruited 15 people who live, work or volunteer in the neighborhood with attention to a diversity of gender, ethnicity and language. Seven meetings were held in person or virtually in 2019-2020 with attendance from 3 to 9 participants. Participants were given prepaid transit cards and a monetary honorarium at the end of the year for those who attended one or more meetings. With their help the clinic improved its website, helped create patient-centered informational resources, and established a community partnership which allowed the PNC to start a food shelf.
This study has several limitations. Key informant interviews may prevent the divulgation of less acceptable information, as participants are acting as representatives of their organizations. However, we found that key informants spoke freely and noted when their perspective differed from that of their organization. Because this study was exploratory and qualitative in nature, another limitation is generalizability. There was considerable heterogeneity in community informants’ knowledge of the PNC, which may limit conclusions that can be drawn from differences in individual perspectives. Future investigations may consider eliciting the perspectives of patients who live in the neighborhood where the PNC is located, as well as determining whether the findings from this study hold true for other community-based SRCs.
To our knowledge, this is the first investigation focused on characterizing the community collaborations of a community-based SRC. This study contributes to a gap in knowledge related to the scope of community-engaged efforts undertaken by SRCs, including interorganizational partnerships and relationship-building activities. Findings from this exploratory study add to literature suggesting SRCs are important sites for health care in high-poverty areas and can advance health on a community level through intentional community engagement. Future research could identify ways to operationalize these study findings as best practices for SRCs interested in developing meaningful community collaborations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.