
Abstract
Background:
Obesity is a significant public health issue in Saudi Arabia. Rising obesity rates increase the risk of weight bias and stigma, even among healthcare workers.
Objectives:
This study assesses weight stigma in healthcare workers, with findings intended to inform strategies for creating a more supportive healthcare environment for patients with obesity.
Methods:
This cross-sectional study was conducted in a university hospital in the Eastern Province of Saudi Arabia. Healthcare workers completed self-administered questionnaires, including the Attitudes toward Obese Persons Scale (ATOP) and the Beliefs about Obese Persons Scale (BAOP), which assess levels of positive attitudes and beliefs about obesity, respectively. Data were analyzed using SPSS.
Results:
The study included 266 healthcare workers (HCWs), mean age 33.21 years, with 54.5% female. The ATOP mean score was 64.4, and BAOP mean score was 18.3, indicating moderate negative attitudes and beliefs toward obesity. Significant differences in ATOP scores were found based on age, patient interactions, and years of experience.
Discussion
Our study aligns with international findings, revealing significant weight stigma among healthcare workers in Saudi Arabia. Such stigma can negatively impact patient care, leading to biased treatment and poorer health outcomes. Societal norms and personal biases contribute to this stigma, despite misconceptions regarding its supposed motivational effects. Addressing this requires comprehensive training and education for healthcare providers. Policymakers should include weight bias education into medical curricula and establish anti-discrimination policies to promote inclusivity and respect.
Conclusions:
Our study highlights obesity stigma among Saudi healthcare workers and the need for targeted interventions. Creating a supportive, nonjudgmental environment can enhance patient-provider relationships and improve healthcare outcomes for individuals with obesity.
Introduction
Obesity has steadily emerged as a significant public health concern in Saudi Arabia, with an adult overweight and obesity prevalence of more than 60%. 1 As obesity becomes more prevalent, societal attitudes toward individuals with obesity often become more negative, leading to increased stigmatization. 2 While healthcare workers are at the frontline of addressing the complications associated with obesity, yet they are not immune to the negative attitudes and beliefs associated with weight bias.3,4 Weight bias or stigma is the negative attitudes and beliefs held toward individuals due to their weight or body size. 3 Although the recognition of the negative effects associated with weight stigma has existed for decades,4 -6 it is noteworthy that a broader acknowledgment of these impacts has only emerged relatively recently.7,8 Counter to intuition, healthcare workers, including physicians and nurses, have been found to harbor implicit and explicit obesity stigmas, a phenomenon observed not only in Saudi Arabia but also in various countries, where studies indicate that weight stigma in medical settings can lead to differences in healthcare delivery, exacerbating obesity-related health outcomes and reducing patient-provider trust.9 -12 A recent meta-analysis reviewed strategies and interventions from various countries aimed at reducing obesity stigma in healthcare settings, highlighting diverse approaches and reinforcing the universal relevance of addressing weight bias. 13 In Saudi Arabia, similar to reports from international studies, weight stigma often arises from cultural beliefs that individuals with obesity frequently overeat, binge eat, or lack the motivation to implement lifestyle changes, reflecting a societal view of obesity as a personal responsibility rather than a complex health issue. 12 Additionally, the rise of social media has amplified these perceptions, as influencers often promote ideals of a “perfect” lifestyle and body image, further shaping public views on obesity and potentially reinforcing stigma. 14 Given the scarcity of research on obesity stigma in Saudi Arabia, this study aims to assess weight bias among healthcare workers in a teaching hospital in the Eastern Province. By understanding the prevalence and determinants of obesity stigma, healthcare organizations can develop targeted interventions to promote a supportive and inclusive environment for patients with obesity.
Methods
This cross-sectional study was conducted in a university hospital in the Eastern Province of Saudi Arabia. Participants included all healthcare workers and faculty staff employed at the university hospital and its affiliated primary care clinics. The sample comprised both Saudi nationals and expatriate healthcare professionals, allowing for the exploration of weight stigma across diverse cultural backgrounds within the healthcare workforce. Using convenience sampling by an online sample size calculator, the sample size was calculated to be 266 with a 95% confidence level. Data was collected using self-administered structured questionnaires distributed via staff email and through in-person visits to their offices. The questionnaire included demographic information such as age, gender, marital status, education level, job title, number of patients with obesity interacting with per week, years of experience, department (internal medicine, emergency, and pediatrics), years of experience, weight, height, and 2 scales: the Attitudes toward Obese Persons Scale (ATOP) and the Beliefs about Obese Persons Scale (BAOP). 15 BMI was calculated using self-reported height and weight. The ATOP is a 20-item Likert scale assessing attitudes toward individuals with obesity, with higher scores (0–120) reflecting more positive attitudes; 13 of the items are negatively worded and require reverse scoring. Similarly, the BAOP is an 8-item scale evaluating beliefs about the control individuals have over obesity, with 6 negative items that are reverse scored. Higher BAOP scores indicate stronger beliefs that obesity is less within personal control. The ATOP and BAOP scales were chosen for their strong validation in assessing attitudes and beliefs regarding obesity, making them widely recognized tools in weight stigma research. These scales are also effective for evaluating healthcare professionals’ perceptions, as they address both attitudes toward individuals with obesity and beliefs about the causes of obesity. Additionally, the response options are designed so that the “best” answer is not immediately predictable, which encourages honest responses and enhances reliability. Other scales were considered, but ATOP and BAOP were selected due to their reliability, relevance, and simplicity, which are crucial for capturing insights on a sensitive topic within our healthcare setting. Most scales assessing weight stigma are relatively old and do not use people-first language, which could perpetuate stigma. At the time these scales were developed, it was more common to use non-person-centered language; however, many organizations have recently adopted people-first language when discussing obesity. 8 The questionnaires were submitted to the Institutional Review Board (IRB) for ethical approval with IRB number 2022-01-412 and informed written consent was taken from all the participants in the study.
Data analysis was conducted using Statistical Package for the Social Sciences software (IBM SPSS statistics for Windows, Version 25, IBM Corporation, Armonk, NY,USA) with descriptive statistics used to summarize demographic information and scale scores. Significance was determined at P < .05.
Results
The questionnaire was distributed to all staff (1207) and the total number of participants was 266 HCWs with a response rate of 22.0 %. The mean age was 33.2(SD = ±9.4; median = 31.0), ranging from 22 to 64 years.
Table 1 shows that 54.5% of the participant HCWs were females, 60.2% were bachelor holders and around one fifth (21.0%) were board certified.
Distribution of HCWs According to Their Socioeconomic and Job Characteristics.
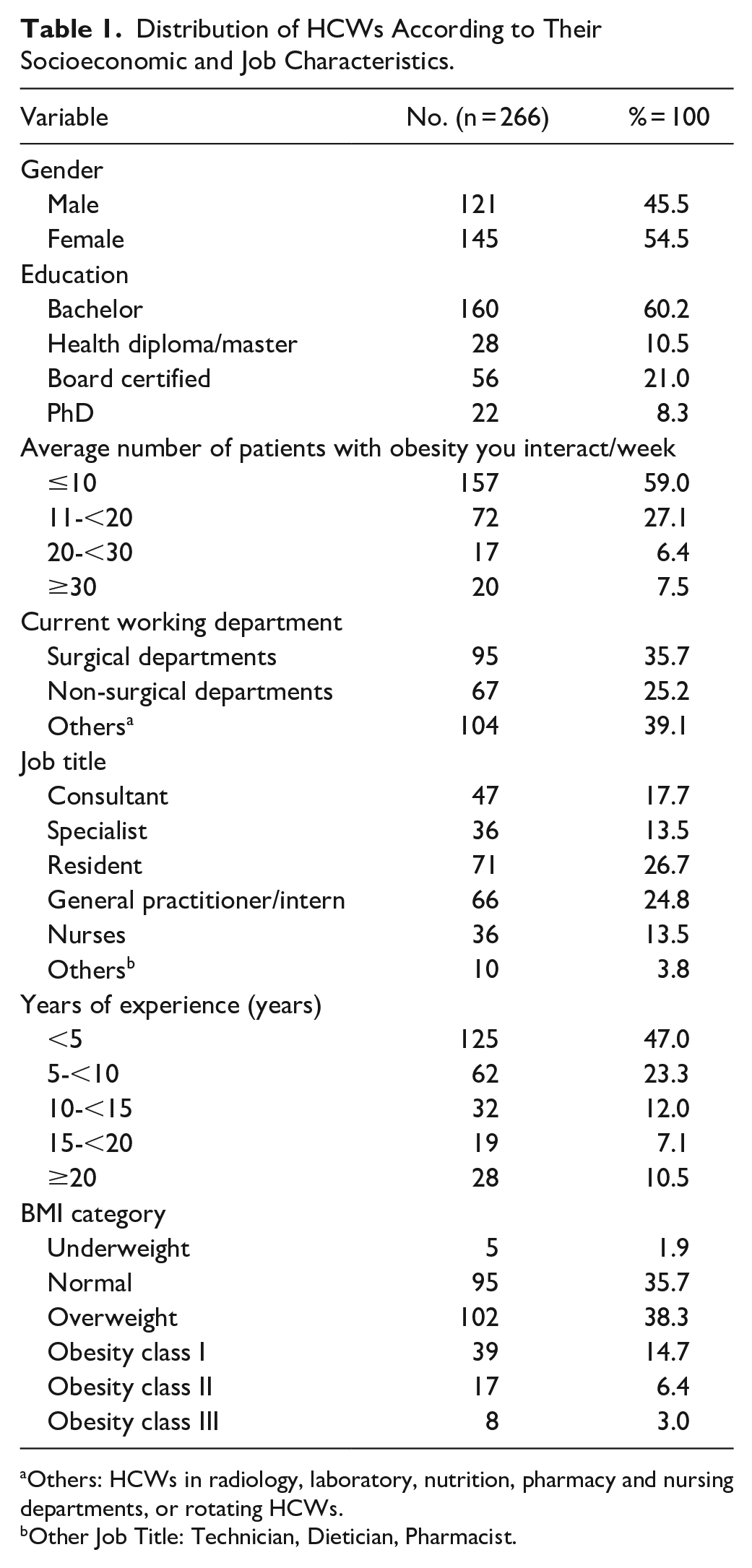
Others: HCWs in radiology, laboratory, nutrition, pharmacy and nursing departments, or rotating HCWs.
Other Job Title: Technician, Dietician, Pharmacist.
Highest percentage of HCWs (59.0%) interacted with an average number of ≤10 patients with obesity, meanwhile only 7.5% of HCWs interacted with ≥30 patients with obesity per week.
Regarding the working experience, nearly half of the HCWs (47.0%) had a working experience of less than 5 years, while those having a working experience of more than 20 years were only 10.5% of the respondent HCWs. Table 1
The average height of HCWs in cm was 165.16 (SD = ±10.8; median = 165.0) ranging from 105 to 186 cm, and the average weight in kg was 74.65 kg (SD = ±19.4; median = 72.0) ranging from 43 to 200 kg. Calculated mean BMI was 27.08 (SD = ±5.7; median = 26.5) ranging from 17.7 to 58.4, with the highest percentage was the overweight (38.3%)
Table 2 shows the distribution of respondent HCWs according to each item response on ATOP 20. As displayed in Table 2, a minority of HCWs strongly agree that “Obese people are as happy as non-obese people” (9.4%), “obese people are not dissatisfied with themselves” (8.4%), “obese people are just as self-confident as other people” (7.9%), and “obese people are just as attractive as non-obese people” (4.9%).
Distribution of HCWs According to Their Responses to ATOP 20.
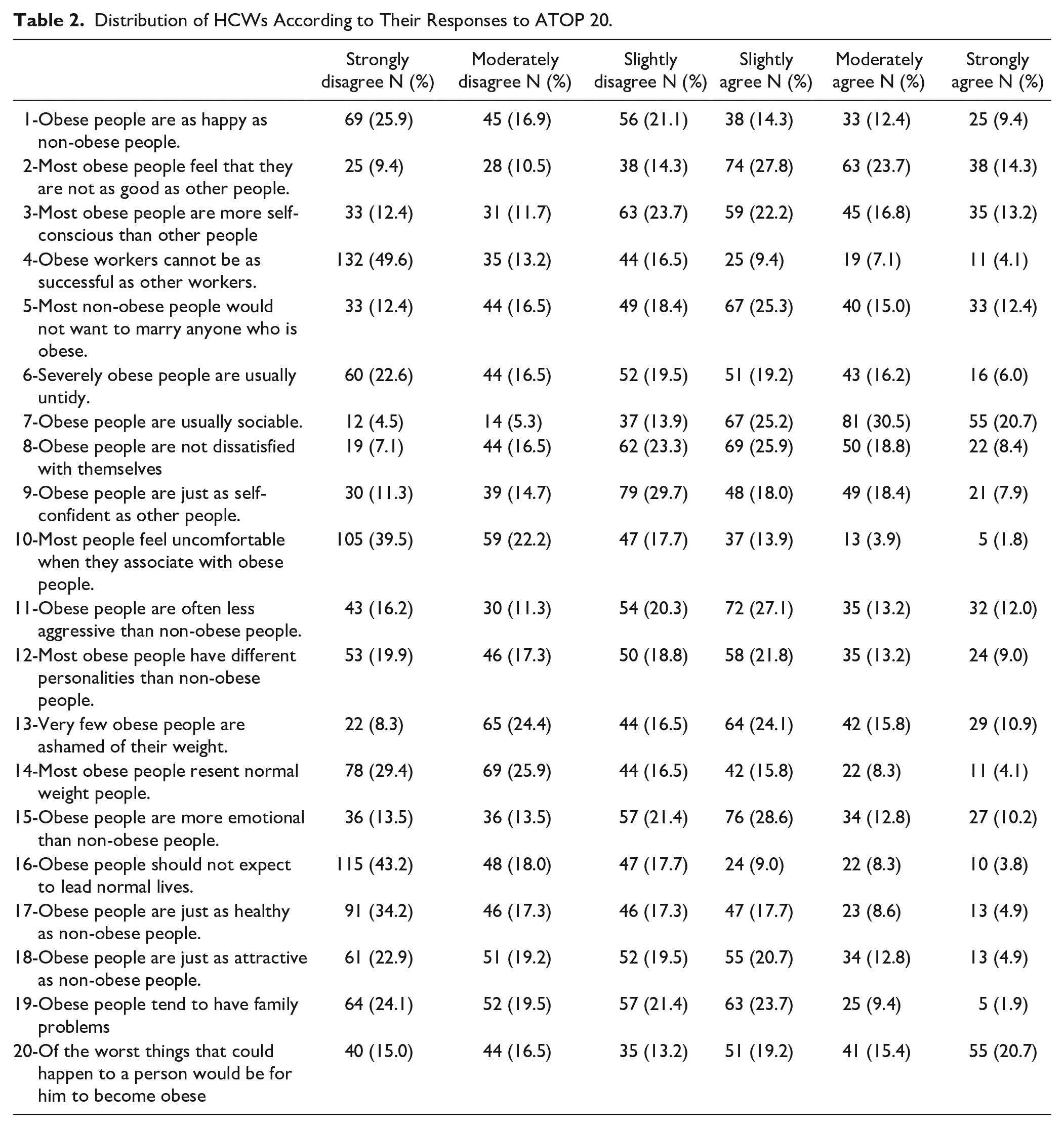
On the contrary, a minority of respondent HCWs strongly agree that “most people feel uncomfortable when they associate with obese people” (4.8%), “most obese people have different personalities than non-obese people” (9.0%), meanwhile those who strongly agree that “of the worst things that could happen to a person would be for him to become obese” represented the fifth (20.0%). The collective mean score for ATOP 20 was 64.4(SD = ±15.1; median = 63) ranging from 23 to 113.
Regarding Beliefs About Obese Persons Scale (BAOP 8), Table 3 shows HCWs responses to each item where 1 quarter of them (25.2%) strongly agree that “most obese people eat more than non-obese people,” “the majority of obese people have poor eating habits that lead to their obesity” (nearly one third 31.3%), and that “people can be addicted to food, just as others are addicted to drugs, and these people usually become obese” (27.1%). The collective mean score for BAOP 8 was 18.3 (SD = ±6.7; median = 18) ranging from 2 to 38.
Distribution of HCWs According to their Responses to BAOP 8.

Differences in ATOP 20 and BAOP 8 in relation to different participants characteristics are shown in Table 4 where no statistically significant differences were observed for BAOP 8 in relation to age, gender, educational level, average number of patients with obesity seen weekly, current working department, job title, years of experience, or category of BMI. However, ATOP 20 scores showed statistically significant differences in relation to age, average number of patients with obesity interacted per week and years of experience. A significant negligible linear correlation is observed (R = .199), HCWs who interact with ≥30 patients with obesity per week had higher ATOP 20 mean score than others (70.55 ± 20.43; P = .027), and those with ≥20 years of experience had a significant higher ATOP 20 mean score than other HCWs (72.67 ± 16.79; P = .012).
Differences in ATOP 20 and BAOP 8 in Relation to Different Participants Characteristics.

Differences regarding ATOP 20 were tested using t test and ANOVA, Meanwhile Mann-Whitney and Kruskal-Wallis tests were used for BAOP 8.
P value significant <.05.
Discussion
Prevalence of Obesity Stigma and Influencing Factors
The findings of our study align with international research, highlighting the widespread existence of weight stigma among healthcare workers in Saudi Arabia. The ATOP mean of 64.4 and the BAOP mean of 18.3 suggest moderate negative attitudes and beliefs toward people with obesity. These results are similar to those reported in studies from other regions, such as Gujral’s evaluation of nurses’ attitudes in hospitals, with comparable ATOP (67.1) and BAOP (18.0) scores. 16 Conversely, studies such as Oliver’s weight sensitivity training among undergraduate nursing students demonstrated more positive attitudes with higher ATOP scores of (74.3) coupled with relatively lower BAOP scores (18.3), suggesting negative beliefs about the controllability of obesity. 17 Additionally, Luig et al’s 18 study on family medicine residents reported ATOP (73.2) and BAOP scores (19.9).
Despite evidence of obesity’s complexity, healthcare professionals may still hold biases due to factors like cultural beliefs, educational gaps, and occupational stress. In Saudi Arabia, obesity is often seen as a preventable condition linked to lifestyle choices, reinforcing the perception that it is personal responsibility. This view creates barriers to empathetic care for individuals with obesity. Furthermore, limited emphasis on obesity education in medical curricula, especially regarding its biological and environmental determinants, may lead to oversimplification of obesity among healthcare workers. Because of the belief that stigmatization of people with obesity will motivate them to lose weight, along with work-related stressors such as high patient volumes and time constraints, it is easier for healthcare providers to adopt stigmatizing attitudes toward individuals with obesity. However, empirical evidence demonstrates that this belief is a societal misconception.4,19,20
In our study, 42.8% of participants disagreed or strongly disagreed that people with obesity can be as happy as those without, and 38% agreed or strongly agreed that many individuals with obesity feel inferior to others. While these responses could initially be seen as implicit bias, they may also suggest a level of empathy and awareness among healthcare providers regarding the social and psychological burdens faced by individuals with obesity. Rather than direct stigma, these perceptions might indicate that healthcare professionals recognize some of the challenges people with obesity encounter in a society that often stigmatizes their condition. This insight reinforces the need for healthcare providers to approach weight management with sensitivity, ensuring their understanding of the complex social and emotional factors associated with obesity enhances rather than hinders patient care.
Impact on Patient Care
The presence of obesity stigma among healthcare workers can have detrimental effects on patient care and outcomes. 21 Stigmatizing attitudes may lead to biased treatment decisions, poorer communication, and decreased patient adherence to medical recommendations. 4 Patients experiencing weight stigma are also less likely to seek healthcare services, leading to delayed diagnoses and exacerbation of health conditions.22 -24 Additionally it can also lead to psychological disorders causing more negative effects toward health or treatment adherence.25,26 This issue is particularly concerning when stigma originates in teaching institutions, potentially passing on biases to future healthcare professionals.
Training and Education
Addressing obesity stigma requires comprehensive training and education initiatives targeted at healthcare providers and students. 13 Interventions such as weight sensitivity training, counter-conditioning techniques, and brief interventions have shown promise in reducing weight bias among healthcare workers and students. 27 Several training programs and online hubs have recently emerged aimed at address weight stigma amongst HCPs.28,29 These programs aim to increase awareness of weight bias, challenge negative stereotypes, and promote empathetic and patient-centered care. Notably, data from other countries, indicate that educational initiatives have effectively reduced weight bias among healthcare professionals. 13 In Saudi Arabia, implementing similar educational frameworks could be particularly beneficial, given the cultural beliefs surrounding obesity as a preventable condition tied to personal responsibility. By integrating successful elements from international models into local training programs, Saudi healthcare institutions can foster a more empathetic approach to care. Furthermore, our data indicate that employees with more experience exhibit less stigma, suggesting that experience may contribute to increased empathy or a greater capacity to engage with a diverse patient population. This trend highlights the importance of developing training initiatives that not only focus on the theoretical aspects of obesity stigma but also encourage healthcare providers to spend more time interacting with patients. By fostering empathy and understanding through experiential learning and continuous engagement, training programs can further enhance the ability of healthcare workers to provide sensitive care to individuals with obesity. To create a more comprehensive and supportive approach to reducing stigma, these programs can be adopted by healthcare institutions, community health organizations, and policymakers.
Policy Implications
Policymakers and healthcare institutions play a crucial role in implementing policies and guidelines aimed at combating obesity stigma. To lessen its impact, weight stigma must be acknowledged and addressed. Eliminating weight stigma is cruical, not only from promoting respect and mental well-being standpoint, but to advance the prevention and where relevant, treatment of obesity. 7 Efforts should focus on integrating weight bias education into medical curricula, establishing anti-discrimination policies within healthcare settings, and fostering a culture of inclusivity and respect for individuals of all body sizes.
Limitations of the Study
The study has several limitations. The relatively small sample size as it was only done in 1 institute and doesn’t necessary reflect the whole targeted staff. Therefore, further studies in different institutes with a larger sample size are required. The study is also limited by the inherent constraints of an online cross-sectional survey which makes it challenging to establish associations between variables. Additionally, there may be self-report bias in that respondents might present socially desirable answers. Furthermore, the scales used in this study do not employ people-first language, which could inadvertently perpetuate stigma among healthcare workers if not clearly contextualized when administering the questionnaire. Future research using qualitative interviews could offer deeper insights and additional information.
Conclusion
Our study highlights the presence of obesity stigma among healthcare workers in Saudi Arabia and emphasizes the need for targeted interventions to address this issue. Healthcare facilities in Saudi Arabia can take proactive steps to reduce weight bias by implementing comprehensive training programs that focus on sensitivity and empathy, alongside fostering a culture of inclusivity. National policy initiatives can also play a crucial role; for example, establishing guidelines for best practices in weight management and integrating weight bias education into medical curricula can help shape the attitudes of future healthcare providers. Future studies in this field should focus on evaluating the effectiveness of these interventions and exploring additional strategies to foster a supportive and nonjudgmental healthcare environment. Longitudinal studies could investigate whether interventions aimed at reducing bias have a long-term effect on healthcare workers’ attitudes toward patients with obesity. By improving patient-provider relationships, enhancing healthcare access and delivery, and ultimately promoting better health outcomes for individuals with obesity, we can make a significant impact on patient care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Ethics Committee of Fondazione IRCCS Istituto Neurologico Carlo Besta approved the study.