
Abstract
This study used a cross-sectional survey design to explore the levels and manifestations of weight stigma experienced by individuals during the COVID-19 pandemic and how it compared to pre-pandemic levels and understanding how stigmatizing experiences have affected health behaviors and healthcare utilization. Adults ages 18–55 completed surveys that assessed weight stigma and discrimination using quantitative and open-ended responses. Participants (N = 88) reported neutral attitudes on measures of weight stigma and moderate weight bias internalization. Weight-based discrimination and interpersonal stigma were lower during the pandemic compared to pre-pandemic. Many participants reported experiencing weight stigma from healthcare providers during the pandemic. Over half of higher-weight respondents reported a negative effect of exposure to COVID-19 news and social media “quarantine-15” mentions on feelings about their weight. The high prevalence of weight-related stigma experienced in healthcare settings may lead to healthcare avoidance and should be a target for improved intervention and policy efforts.
Introduction
Weight stigma, or social devaluation and marginalization of people who are perceived to have excess weight, has been well established as a prevalent national and global public health problem (Andreyeva et al., 2008; Brewis et al., 2018; Rubino et al., 2020; Spahlholz et al., 2016). It is pervasive in a variety of settings, including healthcare, media, schools, workplaces, families, and general community settings, and can cause discriminatory practices and negative attitudes about people in larger bodies (Pearl, 2018; Puhl and Heuer, 2009, 2010; Rubino et al., 2020). The experience and internalization of weight stigma is associated with poor physical and mental health outcomes, likely mediated by stress responses (Emmer et al., 2020; Tomiyama, 2014; Warnick et al., 2022; Wu and Berry, 2018), and significantly increases risk of mortality, independent of BMI (Sutin et al., 2015).
Intersecting with the association between weight stigma and poor health outcomes is the continued finding that weight bias remains prevalent in healthcare, which in turn influences the care provided to patients and healthcare utilization of those who experience bias. For example, patients who report experiencing weight stigma from a provider report lower trust and satisfaction, compounded with feelings of shame, which can lead to avoidance or delay of healthcare appointments (Findling et al., 2020; Phelan et al., 2015). Importantly, weight stigma-related healthcare avoidance has been linked to poor management of chronic health conditions and worse health outcomes (Pearl and Schulte, 2021). Therefore, given the need for healthcare access during a worldwide pandemic, addressing weight bias in healthcare is a critical priority.
Beyond healthcare settings, the COVID-19 pandemic, a worldwide public health crisis that resulted in illness and excess mortality due to the SARS-CoV-2 coronavirus, introduced new conditions that may have amplified weight stigma among the public (Townsend et al., 2020). Weight stigmatizing COVID-19-related social media and news content proliferated in the early years of the pandemic, often linking weight status to COVID-19 infection risk and outcomes, with a high frequency of memes and warnings about quarantine weight gain (de Macêdo et al., 2022; Flint, 2020; Pearl, 2020). This messaging may have increased interpersonal weight stigma, including negative comments about weight from friends, family, or healthcare providers (Bhasker and Greve, 2020; Lessard and Puhl, 2021), even while exposure to in-person weight-related stigmatizing situations was reduced due to quarantines and social distancing (Fung et al., 2021). Pre-pandemic encounters with weight stigma also may have influenced the COVID-related experiences of people in larger bodies, particularly as the simplistic use of BMI as a surrogate for estimating COVID-19 risk furthered the idea of body size as a measure of health (Gutin, 2021), with some media sources citing people in larger bodies as a drain on limited resources, increasing dehumanization and fear (Carbone-Moane and Guise, 2021). In the United Kingdom, the pandemic strategy released by the National Health Service (NHS) was criticized for being particularly stigmatizing (The Lancet Diabetes & Endocrinology, 2020), with a press release that stated, “lose weight to beat COVID-19 and protect the NHS.” In the United States, the social media discourse around COVID-19 and weight became particularly biased and harmful during times of important pandemic-related government announcements (Pollack et al., 2023).
Another stigmatizing theme during the height of the pandemic was the so-called “quarantine-15,” or potential weight gain resulting from isolation (de Macêdo et al., 2022). Social media posts regarding the “quarantine-15” or “fattening the curve” may have contributed to stigma toward those who were already perceived as having excess weight (Pearl, 2020), with evidence that up to half of these messages endorsed weight stigmatizing attitudes and messages, while perpetuating oversimplified beliefs about the controllability of body size through diet and exercise (Lucibello et al., 2021).. These messages were also linked to increased depression and worsened wellbeing (Jones et al., 2022) and compounded existing negative mental and physical effects of the pandemic on individuals with disordered eating symptomatology (Cooper et al., 2022; Devoe et al., 2023; Schlegl et al., 2020; Termorshuizen et al., 2020). Higher weight children experiencing stigma had significantly higher levels of stress, depression, and COVID-19 infection fears than their counterparts (Chen et al., 2021; Puhl et al., 2020). Thus, researchers have noted that it is imperative to understand how weight stigma was experienced by individuals during the pandemic and its resulting effects on health and health behaviors (Pearl and Schulte, 2021; Puhl et al., 2020).
Evidence on whether weight stigma increased during the pandemic compared to pre-pandemic is mixed, and it remains unclear how experiences varied by different subgroups of people and types of stigmatizing pandemic situations (de Macêdo et al., 2022; Jones et al., 2022; Pearl and Schulte, 2021). Therefore, the objective of this study was to use a cross-sectional observational design to better understand the manifestations of weight stigma that individuals experienced during the COVID-19 pandemic in relation to pre-pandemic levels of weight stigma, including weight-based discrimination in healthcare and other settings; the effects of news and social media related to weight, COVID-19, and quarantine on weight stigma; and perceptions of the relationship between weight stigma and health behaviors. Specifically, we (1) describe the average levels of explicit attitudes about weight and levels of weight bias internalization among a convenience sample of adults, and evaluate if they differ by weight status (with obesity vs without), and (2) evaluate the association between experiences of weight-based discrimination, interpersonal sources of stigma, and exposure to stigmatizing situations pre-pandemic and during the pandemic, in addition to the moderating effect of weight status on these relationships. The primary hypotheses were that experiences of weight-based discrimination, interpersonal sources of stigma, and exposure to stigmatizing situations would increase during the pandemic compared to pre-pandemic, and that individuals with obesity would report greater increases than those without obesity. Additional exploratory analyses evaluated the frequency of participants who reported specific discriminating situations during the pandemic, in the sample overall and among those with obesity.
Methods
Study design and recruitment
A convenience sample of adults were recruited to complete an online survey in the summer of 2021, during the COVID-19 pandemic. The cross-sectional survey was created to assess the impact of the COVID-19 pandemic on participants’ experiences of weight stigma and discrimination, and how these experiences have affected participants’ health behaviors and healthcare utilization. In addition to quantitative items, the survey included open-ended items to uncover nuances in adults’ experiences and perceptions of weight stigma that could not be captured by closed items. Participants were recruited through social media (Facebook group posts, including posts to the authors’ social media groups such as local neighborhood/community groups, young adult groups, and parents’ groups), and email listservs for university students and employees. Recruitment materials consisted of a brief paragraph explaining the goal of the cross-sectional survey with a link to the REDCap (Research Electronic Data Capture) survey. When accessing the link, individuals were first presented with the online informed consent form. Individuals who provided consent then received a set of eligibility questions. Eligibility criteria included being 18–55 years old, able to read and write English, and living in the United States. Individuals who were eligible then proceeded to the survey questions. All survey responses were completed between June and September 2021. No incentives were provided for participation in the survey.
Measures
Quantitative measures included in the survey assessed multiple aspects of experiences of weight stigma and weight-based discrimination, as well as weight bias internalization.
Demographic information
Participants answered standard demographic questions, including age range, race, ethnicity, gender, and current weight and height. Weight and height were used to calculate body mass index (BMI; kg/m2). BMI was used to create weight status categories, in which participants were dichotomized between obesity (BMI ⩾30) and non-obesity (BMI <30).
Explicit attitudes (pre-pandemic)
The Beliefs about Obese Persons Scale (BAOP; Allison et al., 1991) is an eight-item Likert scale that assesses explicit attitudes regarding the characteristics of people in large bodies, as well as the causes of obesity (example item: “obesity is usually caused by overeating.”). Items are rated from 1 = strongly disagree to 6 = strongly agree and summed to reach a total score with a range of 8–48. A higher score is indicative of the belief that obesity is not under individual control. Participants were asked to respond to the BAOP items retrospectively, based on their beliefs prior to the beginning of the COVID-19 pandemic (before March 2020). The BAOP scale demonstrated good internal consistency in this sample (Cronbach’s α = 0.86).
Weight bias internalization (pre-pandemic)
The Modified Weight Bias Internalization Scale (WBIS-M; Pearl and Puhl, 2014) is a validated measure of weight bias internalization adapted from a prior version (Durso and Latner, 2008) to apply to men and women across the spectrum of body weight. Example items include “I hate myself for my weight.” Items are rated from 1 = strongly disagree to 7 = strongly agree and summed to reach a total score with a range of 7–77. The WBIS-M was assessed retrospectively, with participants responding regarding beliefs prior to the beginning of the COVID-19 pandemic (before March 2020). The WBIS-M demonstrated excellent internal consistency in this sample (Cronbach’s α = 0.91).
Experiences of discrimination (pre- and during pandemic)
The six-item experience of weight-based discrimination scale (Farrow and Tarrant, 2009) was included to evaluate the extent to which individuals felt personally victimized by weight-based discrimination. Example items include “I feel like I am personally a victim of society because of my weight,” and “I have personally been a victim of weight-related harassment.” Items are rated on a Likert scale from 1 = totally disagree to 7 = agree very much and averaged for the final score. Participants responded to these items twice, reporting experiences of discrimination that occurred prior to the COVID-19 pandemic (“. . .how you felt prior to COVID-19”) and reporting experiences of weight-based discrimination since March 2020 (“. . .how you have felt during the COVID-19 pandemic, since March of 2020.”). This scale demonstrated excellent internal consistency in this sample for both time points (Cronbach’s α = 0.95 and 0.93 for pre- and during pandemic, respectively).
Interpersonal sources of stigma (pre- and during pandemic)
Interpersonal sources of weight stigma were assessed with a measure that provided a list of 12 types of people (i.e. family members, healthcare providers, employers, strangers on social media, etc.) and participants were asked to rate the frequency of weight-based discrimination or stigma from each type on a Likert scale from 0 = never to 3 = multiple times (Puhl and Brownell, 2006). The 12 people types were grouped into 7 source types: family, spouse (acquired family), friends, educators, work, healthcare, and community. Each source type rated as “multiple times” as given a score of 1, and the 7 source scores were combined for a total composite score ranging from 0 to 7. Participants completed this matrix twice, reporting instances of stigma attributable to each source prior to the COVID-19 pandemic and since March 2020. This scale demonstrated excellent internal consistency in this sample for pre-pandemic (Cronbach’s α = 0.92) and good internal consistency for during the pandemic (Cronbach’s α = 0.86).
Exposure to stigmatizing situations (pre- and during pandemic)
A modified 10-item version of the Stigmatizing Situations Inventory (SSI; Vartanian, 2015) was included to assess types of experiences that participants have had with weight stigma prior to and during the COVID-19 pandemic. Items included “being stared at in public,” and “having a doctor recommend a diet, even if you did not come in to discuss weight loss.” Participants rated items on a Likert scale from 1 = once in your life to 9 = daily and the 10 items were averaged for a final score ranging from 1 to 9. This scale demonstrated excellent internal consistency in this sample for both time points (Cronbach’s α = 0.92 and 0.94 for pre- and during pandemic, respectively).
Weight-related stigmatization and discrimination from healthcare and media (during pandemic)
Items assessed perceived stigmatization and discrimination from healthcare providers, if utilization of healthcare resources during the COVID-19 pandemic was affected by weight-related stigmatization, and if exposure to news stories and social media regarding body weight, COVID-19, and the “quarantine-15” affected their experience of stigmatization and discrimination. Example items include “Have you delayed or canceled any healthcare appointments since March 2020 due to concerns about weight-based discrimination?,” “Has your exposure to news stories about body weight and COVID-19 affected your experience of weight stigma or discrimination?,” and “Have ‘quarantine-15’ posts affected how you feel about your body or your weight?,” with response options of “Yes” or “No.” Responses of “Yes” to each of the items assessing experiences of weight-based discrimination in healthcare and the media triggered open-ended questions that asked the participant to describe how their experiences have affected them (e.g. “Please describe how [social media] posts about the ‘quarantine-15’ have affected how you feel about your body or your weight.”). These open-ended items were included in the survey to give participants an opportunity to describe how their experiences of weight-based discrimination, weight stigma internalization, and exposure to weight-related news media have affected how they feel about their bodies and their weight and to give participants a chance to share information that was not possible in the quantitative items. One final item assessed the extent to which participants felt like weight stigmatization or discrimination during COVID-19 affected their eating behaviors (1 = not at all, to 5 = very much). The internal consistency of the items that everyone received was α = 0.70 (adequate given the binary response options).
Other measures
Additional questions assessed participants’ history of eating disorder diagnoses and the relationship between the experience of weight stigma and behaviors related to preventing COVID-19 infection: “Do you feel like your experiences of weight internalization or discrimination during the COVID-19 pandemic have affected the actions you have undertaken to prevent becoming infected with COVID-19? (Scale 1 = not at all, to 5 = very much).” Participants were also asked about other types of stigma that they have experienced (e.g. pertaining to race, gender, sexual orientation, etc.) and how that has affected their feelings about their body size.
Data analysis
Descriptive statistics were calculated for demographic variables and to describe the sample in terms of their pre-pandemic explicit attitudes toward obesity (BAOP) and weight bias internalization (WBIS). Independent samples t-tests were used to determine if explicit attitudes and weight bias internalization varied by weight status (BMI below 30 and 30 and above).
For the primary aims, paired t-tests were used to evaluate differences in experience of discrimination, interpersonal sources of stigma, and exposure to stigmatizing situations pre-pandemic compared to during the pandemic. To determine if any differences existed between respondents with BMI below 30 and 30 and above, independent samples t-tests evaluated differences in these following variables both prior to COVID-19 and during COVID-19. Additionally, to determine if BMI category was associated with changes in scores on experience of discrimination, interpersonal sources of stigma, and exposure to stigmatizing situations during COVID-19 (as compared to prior to COVID-19), separate linear regression models regressed BMI category on the during COVID-19 value, controlling for the prior to COVID-19 value.
For items assessing experiences of weight-related discrimination in healthcare and the media, frequencies were used to report the percent of all participants who endorsed each item, in addition to the percent of participants with BMI ⩾30 who endorsed each item. Furthermore, many participants who endorsed experiencing weight-related stigma or discrimination provided detailed accounts in the open-ended questions; thus, a selection of illustrative quotations are included below to provide contextual insight into participants’ experiences with weight stigma.
Results
Sample characteristics
The survey was active for 6 weeks and a total of 88 participants completed the survey and were included in the analysis. Demographic information of survey participants is displayed in Table 1. Participants were predominantly non-Hispanic white females, most had a college degree, 57% were between the ages of 25 and 44, and had an average BMI of 32.3 (SD = 9.6). A total of eight participants (11%) had either a current or past eating disorder diagnosis. All participants (N = 88) completed all primary items (i.e. items without additional branching).
Demographics of participants (N = 88).
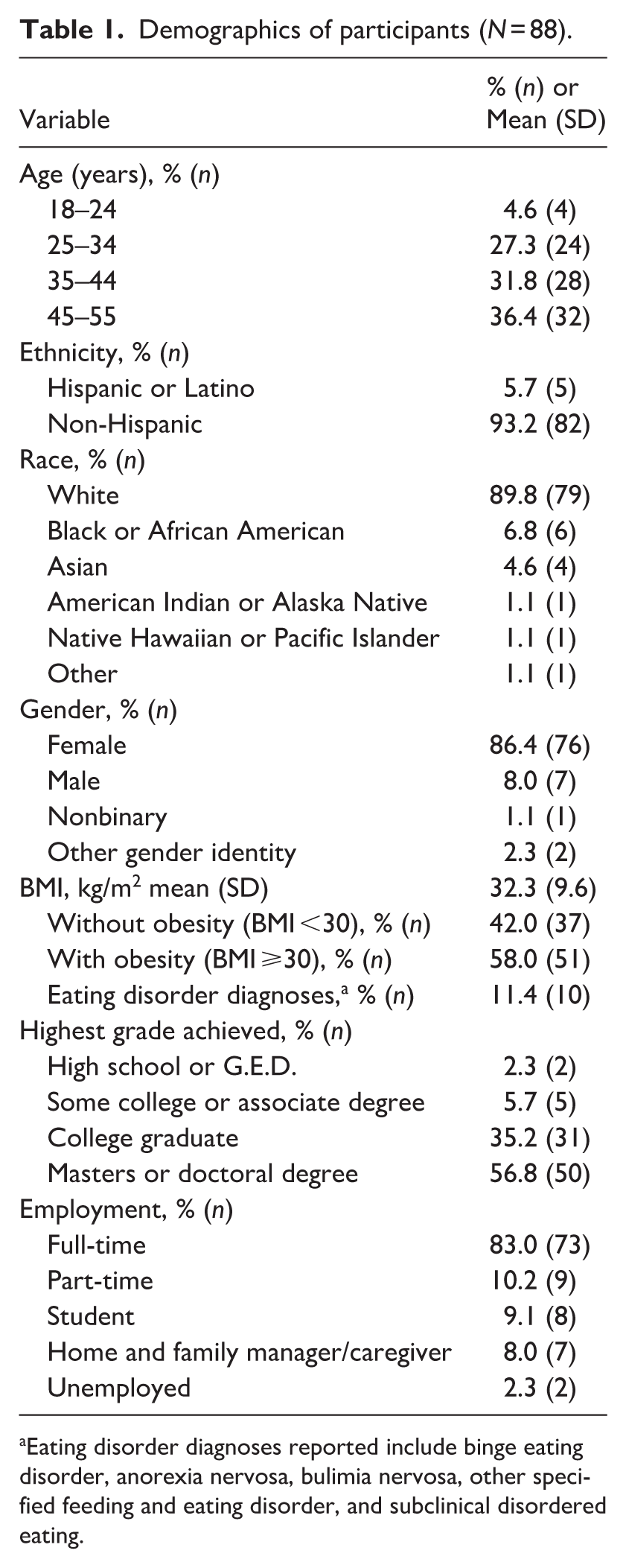
Eating disorder diagnoses reported include binge eating disorder, anorexia nervosa, bulimia nervosa, other specified feeding and eating disorder, and subclinical disordered eating.
Explicit attitudes
Results of weight bias measures included in the survey are presented in Table 2. The BAOP average scores demonstrate neutral attitudes of explicit weight stigma among participants in the sample. The BAOP scores did not differ significantly by BMI category.
Weight bias, reported retrospectively as prior to and during the COVID-19 pandemic, stratified by weight status.
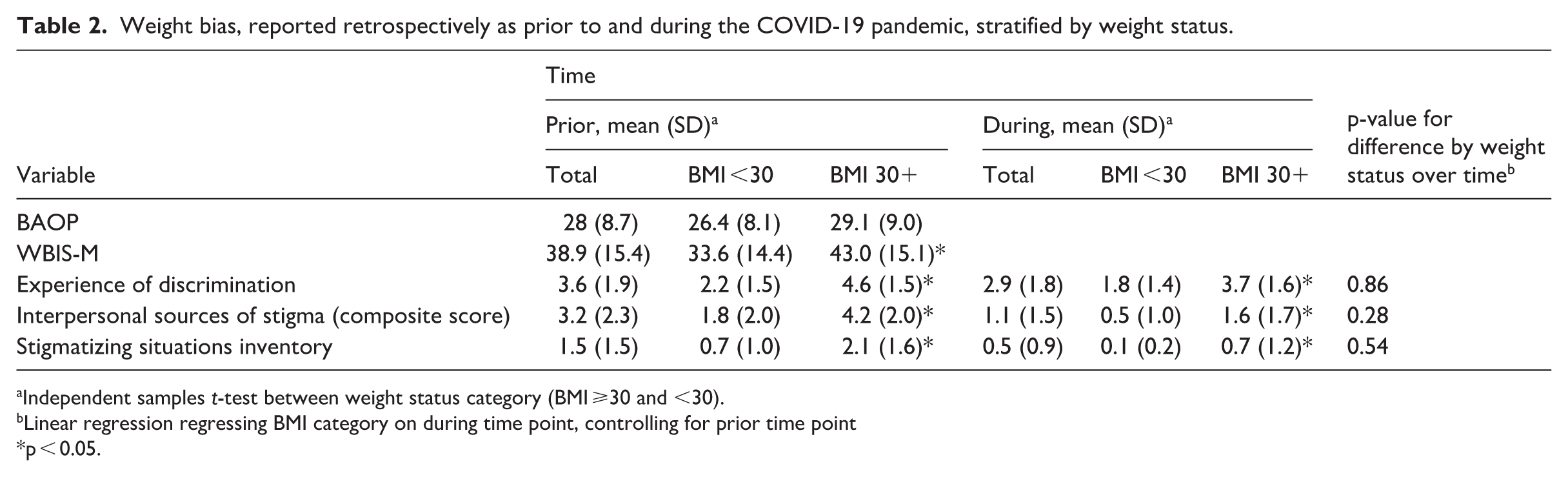
Independent samples t-test between weight status category (BMI ⩾30 and <30).
Linear regression regressing BMI category on during time point, controlling for prior time point
p < 0.05.
Weight bias internalization
The WBIS-M average score demonstrates a moderate level of weight bias internalization among participants in the sample. Mean WBIS-M scores differed significantly by BMI category, with higher internalized bias in the group with a BMI of 30 or greater (p < 0.05).
Experiences of weight-based discrimination, interpersonal sources of stigma, and exposure to stigmatizing situations prior to and during COVID-19
For the total sample, the experience of weight-based discrimination was higher prior to than during the COVID-19 pandemic. When stratified by BMI, the experience of discrimination was higher prior to the pandemic in both groups but was significantly higher in the BMI 30+ group at both time points (p < 0.05). Similarly, the interpersonal sources of stigma composite score and SSI followed a similar pattern, with higher scores prior to the pandemic for the total sample as well as both BMI categories, but significantly higher scores among the BMI 30+ group at both time points (p’s < 0.05). There were no differences in change from prior to during the pandemic by weight status in these variables.
Weight-related stigmatization and discrimination from healthcare and media
Table 3 presents the percentage of respondents who endorsed experiencing weight-based discrimination from healthcare and media during the COVID-19 pandemic. Almost a third of the sample endorsed experiencing weight stigma or weight-based discrimination from healthcare providers during the pandemic. Among those that endorsed experiencing discrimination from healthcare providers, 22% canceled a healthcare appointment due to concerns about weight stigma, with 10% endorsing canceling COVID-19 related appointments due to weight stigma concerns. The percentage of respondents who experienced stigma and endorsed healthcare avoidance was markedly higher among those with a BMI 30+. Among those, 44% experienced weight stigma from providers, 31% delayed or canceled an appointment, and 15% canceled a COVID-19 related appointment due to weight stigma concerns. Weight stigma was also present in telehealth, experienced by nine individuals in this sample, eight of which were in the BMI 30+ category. Below are examples of direct quotations from participants describing how their experience(s) of stigmatization from healthcare providers has affected them:
“[HCPs] focus on my weight and divert conversation about other health concerns.”
“I know I’ll always need to push more than I should if a provider won’t think beyond my weight.”
“they have made me want to avoid healthcare in general”
Percent of participants who endorsed experiencing discrimination in healthcare and the media since March 2020.
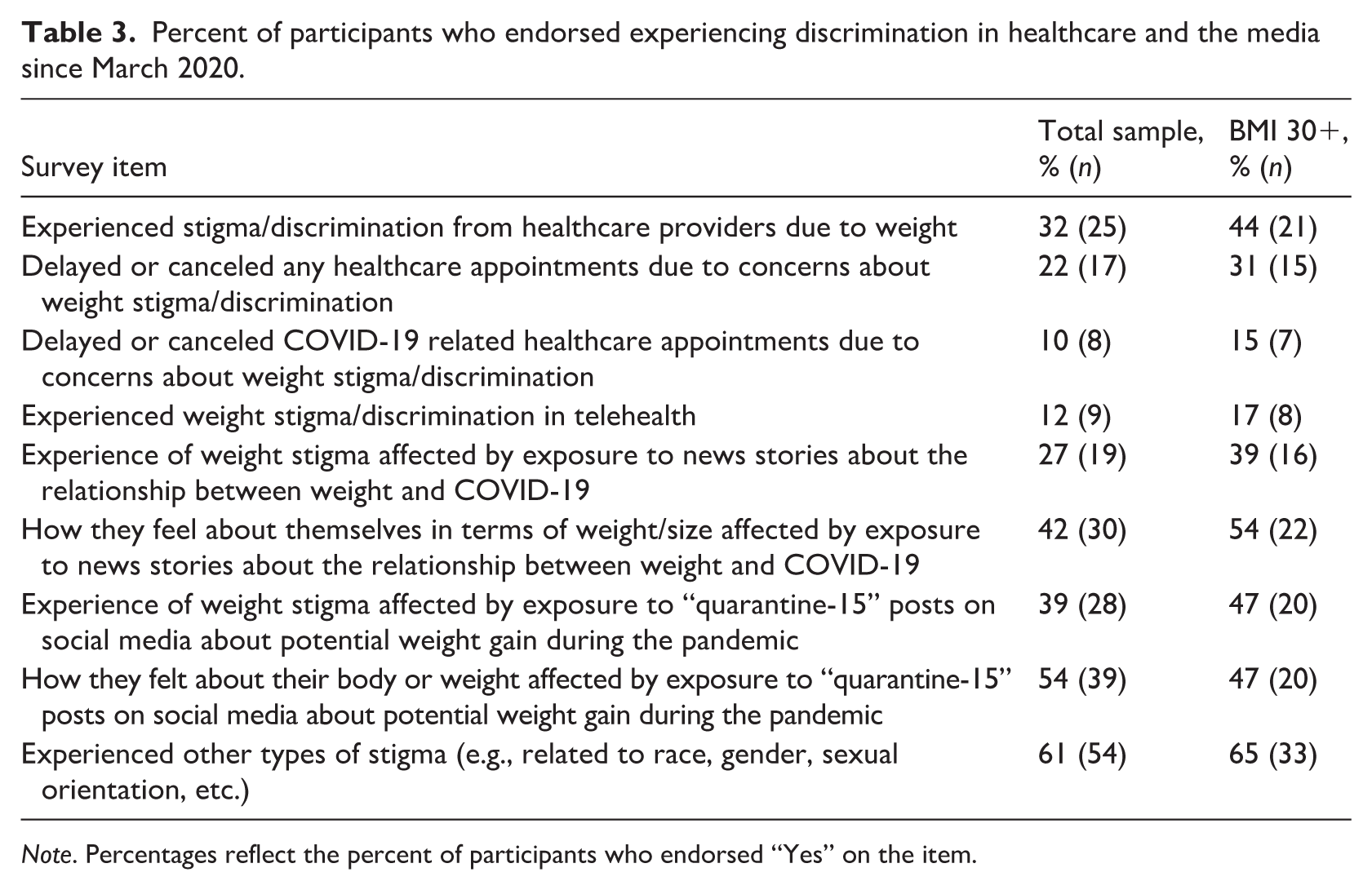
Note. Percentages reflect the percent of participants who endorsed “Yes” on the item.
Thirty-nine percent of respondents with a BMI of 30+ said that exposure to news stories about the relationship between weight and COVID-19 affected their experience of weight stigma, and 54% said that those stories affected how they feel about their weight or body size. Almost 40% of the total sample, and 47% of those with a BMI of 30 or higher, said that exposure to “quarantine-15” social media posts affected their experience of weight stigma. Over half (54%) of the total sample said that exposure to “quarantine-15” social media posts affected how they felt about their body or their weight, while only 47% of respondents with a BMI 30+ agreed. Below are examples of direct quotations from participants describing how exposure to news, social media, and the “quarantine-15” affected their experience of weight stigma:
“constant media about weight and covid or people overweight. . .more likely to die or have bad cases made me very fearful about getting the virus and then when I did get sick, I was very worried I was not going to be able to pull through.”
“I believe [the quarantine-15] implies that overweight people are that way because of their sedentary and quarantine-like lifestyle, and that it is a choice.”
“Similarly to the “freshman-15” it creates a toxic environment where people are constantly comparing weights and weight gain/loss.”
Effect of weight-based discrimination on health behaviors
Twenty-three percent of respondents reported that experiences of weight-based stigma or discrimination during the COVID-19 pandemic affected their eating behaviors, 31% reported that it affected their activity behaviors, and 18% reported that it affected the actions they took to prevent COVID-19 infection.
Discussion
The purpose of this cross-sectional observational study was to learn more about adults’ experiences of weight stigma and internalization during the COVID-19 pandemic, and if they perceived any changes in stigma and internalization due to healthcare providers, news, social media, or friends and family during the pandemic. This descriptive study is one of the first to explore the experiences of both pre-pandemic and pandemic-related weight bias and stigmatization in healthcare, social media, and the community. The sample overall reported neutral personal weight bias attitudes (i.e. neither positive or negative) and reported moderate levels of weight bias internalization over their lifetime. Contrary to our hypotheses, weight-based discrimination and interpersonal stigma were lower during the pandemic compared to pre-pandemic. As expected, participants with a BMI of 30+ experienced significantly higher weight-based stigma and discrimination at all time points.
Results of this study revealed a high prevalence of weight stigma (around 10%–30%) experienced in healthcare settings and participants’ endorsement of responsive healthcare avoidance. The negative impact of stigmatizing healthcare on people in larger bodies has been well established prior to this global public health emergency (Alberga et al., 2019; Phelan et al., 2015). Specifically, the consequences of delaying or canceling healthcare appointments compound the negative impacts of weight stigma itself (Phelan et al., 2015), which is salient during a global pandemic in which access to healthcare is pivotal to obtain COVID-19 vaccines, education, and treatment. While healthcare providers may not readily identify a connection between weight stigma and virus prevention, it is notable that several participants explicitly endorsed canceling COVID-19 related appointments due to weight stigma concerns. This highlights a strong need to prioritize weight stigma education and interventions among providers.
For both the total sample and higher-weight respondents, an unexpected trend emerged of decreased weight stigma and reduced exposure to stigmatizing situations during the COVID-19 pandemic. This contrasts with the prior reviews that suggested that the pandemic and COVID-19-related social media messaging may have exacerbated weight bias and stigma, though they noted that results have been mixed (de Macêdo et al., 2022; Pearl and Schulte, 2021). While the causal effects of pandemics on weight stigma and related concerns are difficult to establish, the results of one study that assessed young adults’ weight concerns at regular intervals beginning in 2017 through 2021 found a significant increase in female young adults’ weight-related concerns at the beginning of the COVID-19 pandemic (Haas et al., 2024). However, weight-related concern is a different construct than experiences of weight bias, and it could be reasonable to expect overall lower experiences of bias and stigma during the pandemic due to changes in daily life throughout the pandemic, including isolation, quarantine, and social distancing measures. Without time series surveys assessing weight stigma that began prior to COVID-19 and continued during and after, it will unfortunately not be possible to firmly evaluate changes in weight stigma due to the pandemic.
Open-ended responses provided additional depth to understand adults’ experiences of weight stigma during the pandemic. In place of treating patients for their primary concerns, participants emphasized that they perceived their provider as focusing on weight as a cause of their reported medical problems. Another common theme regarding healthcare access was that some participants experienced ambivalence and avoidance of healthcare during the pandemic, and these breakdowns in communication are likely to result in reductions in overall quality of care for larger patients, further contributing to size disparities in outcomes from COVID-19 as well as from other acute and chronic conditions. Some respondents also noted that news and social media related to COVID-19 have had profound effects on participants’ body image and experiences of weight stigma. Themes in the responses included increased body and weight shame and fear of severe COVID-19 disease and death. “Quarantine-15” posts on social media prompted reactions that ranged from feeling more socially accepted due to the ubiquity of pandemic weight gain to feeling increasingly shamed and stigmatized.
Long-term implications from the convergence of experiencing discrimination and existing during a global pandemic are yet unknown, especially given the mixed findings that some may have experienced lower discrimination and stigma due to social distancing and quarantine efforts, while others may have experienced more depending on their exposure to media, HCPs, and other situations in their life. Amid mounting evidence that weight stigma is correlated with decreased health-promoting behaviors like healthy eating and movement (Zhu et al., 2022), one of the salient findings is that healthcare avoidance remains a pressing concern. Responsive healthcare avoidance and the negative health effects of weight stigma itself will likely compound these effects for people in marginalized bodies.
While the survey was not designed to analyze the effect of multiple marginalized identities on participants’ experiences of weight stigma during the pandemic, it is notable that over half of the total sample endorsed experiencing other stigmas, including those related to race, ethnicity, and gender. Evidence for the cumulative effects of holding multiple marginalized identities is emerging, and future research should analyze the effects of the intersection of different stigmas (Denise, 2012; Himmelstein et al., 2017).
Strengths and limitations
The primary limitation of this cross-sectional study is the retrospective nature of the design. While this design cannot answer causal questions about the effect of a pandemic on weight stigma, it nonetheless provides insight into the perceptions and experiences of adults during this time. Notably, given that pandemics cannot be predicted, a prospective design to study changes from before a pandemic to during a pandemic is not possible. Thus, this retrospective design, while limited, can provide insight on perceptions and experiences that would not have otherwise been collected. Additionally, the evaluation of multiple comparisons increases the potential for an inflated Type 1 error, though notably the analyses were primarily descriptive and intended to identify patterns to inform future research rather than determine causal relationships. Nonetheless, these findings should be interpreted with caution.
A second limitation is the retrospective recall of some of the measures that evaluated lifetime exposure to weight stigma, which were compared to levels of stigma experienced in the relatively short period from March 2020 to summer of 2021. Third, mental health outcomes were not measured, though there is evidence that exposure to perceived negative representations of higher weight people in the media were associated with increases in psychological distress among higher weight people during the pandemic (Sutin et al., 2020). Fourth, the recruitment methods resulted in a convenience sample of adults that was small and lacked diversity, consisting primarily of non-Hispanic white highly educated and employed females, which may have introduced selection bias and limits the generalizability of the results to larger populations of adults. Finally, no incentive was provided to complete the survey, meaning that the results are biased toward adults who likely already had an interest in weight stigma or have a general interest in contributing to scientific efforts. While this biases the sample and the results should be interpreted with caution, it is notable that general experiences of weight bias were rated fairly neutral, and overall the sample did not appear to be experiencing greater levels of weight stigma relative to the general population.
Conclusions, recommendations for future research, and policy implications
These results contribute depth to our understanding of how the COVID-19 pandemic and its associated restrictions, along with related news and media, have affected peoples’ experiences of weight stigma, though results should be interpreted with caution given the study limitations. Weight-based stigma and discrimination was experienced at lower levels during the pandemic versus prior to it, possibly due to isolation measures that limited exposure to stigma. However, healthcare providers were a prominent and problematic source of stigma during the pandemic, resulting in significant endorsement of healthcare avoidance (both COVID-19 related and not). Many participants also felt stigmatized by exposure to news stories about weight and COVID-19 and by “quarantine-15-type” social media posts. Interventions and policies to reduce weight stigma remain limited (Puhl, 2022), despite clear evidence of its negative health effects and the uncommon social acceptability of that bias (Puhl and Heuer, 2009). This study contributes to the weight stigma literature by highlighting how messaging during a global crisis can exacerbate discrimination and undermine truth in medicine and public health, which steers people away from necessary care and is detrimental to population-level risk reduction during a global pandemic. These insights highlight the need for sustained efforts to reduce weight bias in clinical practice and public health policy, such that lessons from the pandemic can ensure preparedness for the future. To reduce the burden of weight stigma and its negative health effects and improve access to non-stigmatizing healthcare, research and interventions at the individual and policy level will be imperative.
Footnotes
Acknowledgements
The use of REDCap for this research was supported by a grant from the Clinical and Translational Science Award program of the Division of Research Resources at NIH (UL1TR002489).
Ethical considerations
The survey was completely anonymous, thus, the Institutional Review Board at The University of North Carolina at Chapel Hill determined the study to be exempt from federal human subjects regulations and all study protocols were approved on 4/26/2021 (#21-0340).
Consent to participate
Respondents provided online informed consent by checking “yes” or “no” to the question “Do you consent to participate?” before starting the surveys. The survey was completely anonymous, and as such, was determined by the UNC Chapel Hill IRB to be exempt from federal human subjects research regulations.
Consent for publication
As noted above, this anonymous study was determined to be exempt from federal human subjects research regulations. The data, and this paper, include no identifying information, images, or videos.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, BN, upon reasonable request.*