
Abstract
Background:
This study investigates breast cancer screening disparities among Mexican immigrant women in rural and urban U.S. communities, focusing on cultural beliefs, healthcare access, and geographical differences.
Methods:
A cross-sectional study of 350 Mexican immigrant women aged 40+ without prior cancer diagnosis was conducted in rural (<2000 population) and urban parts of the U.S. in 2015. Culturally tailored surveys during household visits, clinic appointments, and community meetings assessed cultural beliefs, mammography engagement, and family support. Comparative analyses t-tests and chi-square tests were conducted, with significance set at P < .05.
Results:
Rural women demonstrated higher adherence to spiritualismo (M = 4.31, SD = 1.13) compared to their urban counterparts (M = 3.91, SD = 1.36), marianismo (M = 3.33, SD = 0.45 vs M = 3.21, SD = 0.48), and machismo (M = 3.02, SD = 0.52 vs M = 2.80, SD = 0.61). The rural women also reported higher mammography rates (54.4% vs 45.6%), with 60.4% undergoing four or more mammograms. Despite barriers such as doctor non-recommendation (55.0% rural vs 45.0% urban) and embarrassment (67.9% rural vs 32.1% urban), rural women engaged more in family discussions about cancer screenings (61.7% vs 38.3%) and received more family assistance in finding health information (59.8% vs 40.2%).
Conclusions:
This study elucidates significant rural-urban disparities in cultural adherence and family support among Mexican immigrant women, underscoring the necessity for culturally tailored interventions to enhance breast cancer screening rates and health outcomes.
Keywords
Introduction
Breast cancer disparities among Latinas in the United States (U.S.) remain a critical health concern. Although Hispanic women are 30% less likely to be diagnosed with breast cancer compared to non-Hispanic white women (90.2 cases per 100,000 vs 133.7 cases per 100,000), they are more likely to receive a diagnosis at a later stage, leading to poorer outcomes. 1 From 2014 to 2018, Hispanic women experienced higher mortality rates for certain cancers, such as cervical cancer, underscoring the need for targeted health interventions. Contributing factors include limited healthcare access, transportation challenges, immigration-related complications, and language barriers, particularly in rural areas where 40% of Hispanic women lack regular healthcare access, compared to 24% in urban areas.1,2
The U.S. Hispanic population reached 62.1 million in 2020, comprising 19% of the total U.S. population and making it the nation’s second-largest racial or ethnic group, behind White Americans. 3 This group is defined broadly, including people who trace their roots to Latin America or Spain, and it is notably diverse, encompassing individuals of Mexican, Puerto Rican, Cuban, Salvadoran, and many other origins. Since 1970, when they represented just 5% of the population, Hispanics have become a major demographic force, accounting for about half of the U.S. population growth between 2010 and 2020 alone. The Hispanic population is also growing rapidly in regions where it has traditionally been smaller, such as North and South Dakota, which saw increases of 148% and 75%, respectively, between 2010 and 2020. 3 This demographic shift reflects both natural growth (more births than deaths) and sustained immigration over recent decades.
Given their significant and expanding presence in the U.S., Hispanic women represent a crucial demographic for public health initiatives, particularly for breast cancer prevention and screening programs. However, their diverse cultural backgrounds can influence healthcare behaviors in complex ways. For example, beliefs such as spiritualismo, fatalismo, familismo, and marianismo play a dual role in shaping health behaviors among Latina women.4,5 Spiritualismo refers to a strong belief in spiritual forces or a higher power, which can provide emotional strength and resilience during medical processes like cancer screening. Fatalismo is the belief that life events are predetermined and beyond individual control, potentially discouraging proactive health behaviors like screenings due to a sense of inevitability regarding illness. 5 Conversely, familismo emphasizes strong family bonds and collective support, which can encourage health screenings by providing emotional backing and assistance in navigating the healthcare system. 5 However, marianismo, which reflects traditional gender roles emphasizing modesty, purity, and self-sacrifice among women, can hinder cancer screening participation due to discomfort in discussing personal health information or undergoing medical examinations, particularly with male doctors. 4 These cultural norms present both opportunities and challenges, significantly shaping how Latina women perceive and engage with healthcare services.
This study aims to analyze breast cancer screening disparities among Mexican immigrant women in Illinois by contrasting rural and urban environments. It seeks to identify the interplay of cultural beliefs, socioeconomic status, family dynamics, and geographical location in influencing mammography practices. The objectives are to define the interactive contributions of structural factors and Latino-specific beliefs in the utilization of breast cancer screening and to develop and pilot test a culturally sensitive intervention addressing these barriers. By understanding how these factors interact, we aim to create interventions that are not only structurally supportive but also culturally relevant, ultimately improving screening rates and health outcomes among this distinct population.
Methodology
Study Design
This study employed a cross-sectional design to examine breast cancer screening disparities among Mexican immigrant women residing in both rural and urban areas of Illinois. The primary aim was to explore cultural beliefs, mammography screening engagement, risk perceptions, and reasons for mammography attendance among these populations. Data were collected using a survey with close-ended questions designed to gather comprehensive information on the variables. The study received approval from the Institutional Review Board at the University of Illinois at Urbana-Champaign, and informed consent was obtained from all participants before any data collection began.
Setting
Data collection took place in a variety of settings across Illinois, encompassing both rural and urban environments. Rural areas were specifically defined using data from the U.S. Census Bureau and the United States Department of Agriculture (USDA) as regions with populations fewer than 2000 residents, distinctly separated from urban centers, to capture a diverse range of experiences from different living environments.6,7 Participants were recruited from rural villages, including Onarga, Gilman, DePue, Arcola, and Capron, and towns such as Champaign and Chicago, ensuring accessibility and comfort for the participants while considering potential transportation limitations and language barriers. Data collection methods included household visits, trailer camps, clinics, and community organizations.
Population
The study targeted low socioeconomic Mexican immigrant women aged 40 and above who had not been previously diagnosed with cancer. A total of 350 participants were recruited from both rural and urban areas to examine breast cancer screening disparities. The inclusion criteria focused on women who met the age and socioeconomic conditions and had not been previously diagnosed with cancer. The recruitment strategy shifted from initial plans for random sampling to targeted and snowball sampling methods to effectively reach the intended demographic within budget and time constraints. Engaging multiple individuals from the same households allowed the study to gain a deeper understanding of family dynamics and their influence on health behaviors and beliefs. Community engagement strategies, such as collaborating with local organizations like the Latino Partnership and La Casa Culture in Champaign, Illinois, were employed to build trust and ensure culturally sensitive engagement.
Community Engagement and Cultural Sensitivity
Community engagement was integral to the study’s approach. The research team liaised with local organizations and community leaders to build trust and ensure culturally sensitive engagement. This approach was particularly important given the potential skepticism from participants due to their immigration status or past experiences with authority figures. Collaborations with organizations such as the Latino Partnership and La Casa Culture in Champaign, Illinois, were crucial in facilitating engagement. All data collection was conducted in Spanish to ensure participants’ comfort and accuracy in their responses.
Cultural humility was a guiding principle throughout the study. The research team was trained to approach participants with respect for their cultural backgrounds, understanding the importance of norms such as collectivism, personalism, and harmony. This approach also involved acknowledging the researchers’ own cultural biases and fostering an environment conducive to learning and mutual respect. Graduate research assistants completed training at the University of Illinois Urbana-Champaign focused on human subjects’ protection and an additional 16-h training specific to the research project. This training emphasized aspects of Mexican culture that might affect research participation, cultivated empathy, and ensured respect for the autonomy and voluntary participation of study participants.
Survey Development
A survey with close-ended questions was developed, translated, and back-translated by a proficient Mexican Spanish community organizer to ensure cultural sensitivity and accuracy. Key terms such as spiritualismo, machismo, and marianismo were clearly defined to capture their nuanced cultural meanings: Spiritualismo reflects beliefs about spiritual or religious factors influencing health; machismo addresses attitudes related to traditional masculine norms; and marianismo explores traditional gender roles and expectations of self-sacrifice and modesty.4,5 Pilot testing was conducted with a smaller group of Mexican-born women to refine the questionnaire and update interview protocols. Cognitive testing techniques were employed during the pilot phase to verify the readability and comprehensiveness of the survey instrument.
Measures
The study includes several demographic variables to provide a comprehensive understanding of the sample characteristics. Participants’ ages were recorded to analyze the distribution within the sample and to explore how age may influence breast cancer screening behaviors. Marital status was categorized into groups such as single, married, widowed, or divorced to examine the impact of social support structures on health decisions. Yearly income was captured and rounded to one decimal place, reflecting the economic context of the participants, which could affect access to and utilization of mammography services. The length of stay in the U.S., measured in years, was included to understand how time spent in the country might influence adaptation to healthcare practices and engagement in preventive health behaviors. Education level was recorded to identify any correlation between educational attainment and knowledge or attitudes toward breast cancer screening. Employment status was categorized as employed, unemployed, or retired, recognizing how work conditions, access to health insurance, and availability of time might impact participants’ ability to engage in regular mammography screenings.
Beyond demographics, the study examined several other key variables to understand cultural and psychosocial factors influencing breast cancer screening behaviors. Acculturation stress measured the psychological strain experienced by participants due to cultural adaptation and discrimination; a higher score indicates greater stress, which may negatively impact their willingness to engage in preventive health activities. 4 Familismo assessed the influence of family values and obligations on health decisions; a higher score reflects a stronger emphasis on family involvement and prioritization of family needs over individual health actions. Modesty evaluated participants’ adherence to cultural norms regarding privacy and body exposure, with higher scores indicating greater discomfort with medical examinations and discussing breast health, potentially creating barriers to mammography uptake. Spiritualismo measured beliefs about the impact of spiritual or religious factors on health outcomes; higher levels suggest a stronger tendency to attribute health conditions to spiritual causes, which may affect healthcare-seeking behavior. Social support was assessed to determine the perceived emotional and practical support from family, friends, and community; higher scores indicate stronger perceived support networks, which can encourage preventive health actions. Marianismo explored traditional gender roles and expectations, with higher scores reflecting greater adherence to norms of self-sacrifice, nurturing, and modesty that may discourage women from prioritizing their health. Acculturation gauged the extent of participants’ adaptation to U.S. culture, including language proficiency and social integration, with higher scores indicating a greater level of integration, potentially facilitating better engagement with the healthcare system. Machismo assessed attitudes related to traditional masculine norms, where higher scores indicate stronger endorsement of these norms, which may indirectly affect women’s health decisions. Mammography screening engagement was measured by whether participants had ever undergone a mammography, the number of mammograms in the last four years, and their routine mammography practices. Reasons for mammography attendance or non-attendance captured various personal and social reasons, including perceived need, physician recommendation, cost, embarrassment, fear of pain, lack of insurance, and transportation challenges, influencing whether participants attended screenings. Lastly, risk perceptions assessed participants’ perceived susceptibility to breast cancer compared to others, beliefs about the likelihood of currently having breast cancer, and perceived predisposition to other health conditions, with higher levels indicating greater perceived risk or concern.
Statistical Analysis
Descriptive statistics, including counts, percentages, means, and standard deviations, were calculated for all variables. Statistical analyses were conducted using t-tests and chi-square tests to compare cultural beliefs and mammography practices between rural and urban participants. The t-tests were employed to compare the means of continuous variables, while the chi-square tests examined associations between categorical variables. A P-value of less than .05 was considered statistically significant. This analytical approach ensured the findings were thorough, reliable, and able to address the primary research questions.
In this study, we used row percentages in our tables to present data comparisons between rural and urban groups. Row percentages show the proportion of participants within each response category (eg, “Yes” or “No” for having a mammogram) for rural and urban groups separately. This approach is used in medical and epidemiological research because it allows for a more direct comparison of subgroups, highlighting the differences in characteristics or responses between groups. By focusing on the proportion of responses within each subgroup, row percentages provide a clearer understanding of disparities and can help identify patterns that might be masked when using column percentages. This method is useful in studies examining health behaviors and outcomes across different populations, as it enables targeted analysis and supports the development of focused intervention.
Ethical Considerations
The study adhered to all ethical guidelines set by the Institutional Review Board at the University of Illinois at Urbana-Champaign. Confidentiality was maintained by de-identifying data and ensuring that interview sessions were conducted with the participants’ comfort and privacy in mind. Researchers were trained to handle any emotional distress experienced by participants and to provide support as needed. Participants were informed of their rights, including the right to withdraw from the study at any point without any negative consequences.
Results
The sample consisted of 321 Mexican-born women residing in Illinois, with an average age of 50 years and an average length of stay in the U.S. of 21 years. Most participants were married (58.6%), while 22.4% had attained secondary education, and 75.39% reported an annual income of less than $30,000. About 38.0% of the participants were employed full-time (Table 1). Rural and urban participants were similar in their educational attainment and income levels but varied in other aspects, such as family structure and employment status.
Demographic Characteristics of Mexican-Born Women in Illinois in 2015, N = 321.

The analysis demonstrated that rural Mexican immigrant women (MIWs) demonstrated a stronger adherence to traditional cultural beliefs compared to their urban counterparts. Specifically, rural MIWs reported higher levels of spiritualismo (M = 4.31, SD = 1.13) compared to urban women (M = 3.91, SD = 1.36), as well as higher adherence to marianismo (M = 3.33, SD = 0.45) versus urban women (M = 3.21, SD = 0.48) and machismo (M = 3.02, SD = 0.52 vs M = 2.80, SD = 0.61) (Table 2). Differences in cultural attitudes also extended to perceptions of cancer risk, with 68.9% of rural women disagreeing with the statement, “I do not think I need to worry about ever getting breast cancer,” compared to 31.1% of urban women, indicating heightened awareness or fear of cancer among rural participants (Table 3).
Demographic Characteristics of Urban and Rural Mexican Immigrant Women in Illinois, 2015.

Abbreviations: M, mean; SD, standard deviation; SE, standard error.
Significant P < .01. **Significant P <. 05.
Independent t-Tests of Study Measures for Mexican Immigrant Women (MIWs) Regarding Breast Cancer Screening and Cultural Beliefs Between Rural and Urban Areas of Illinois, 2015.
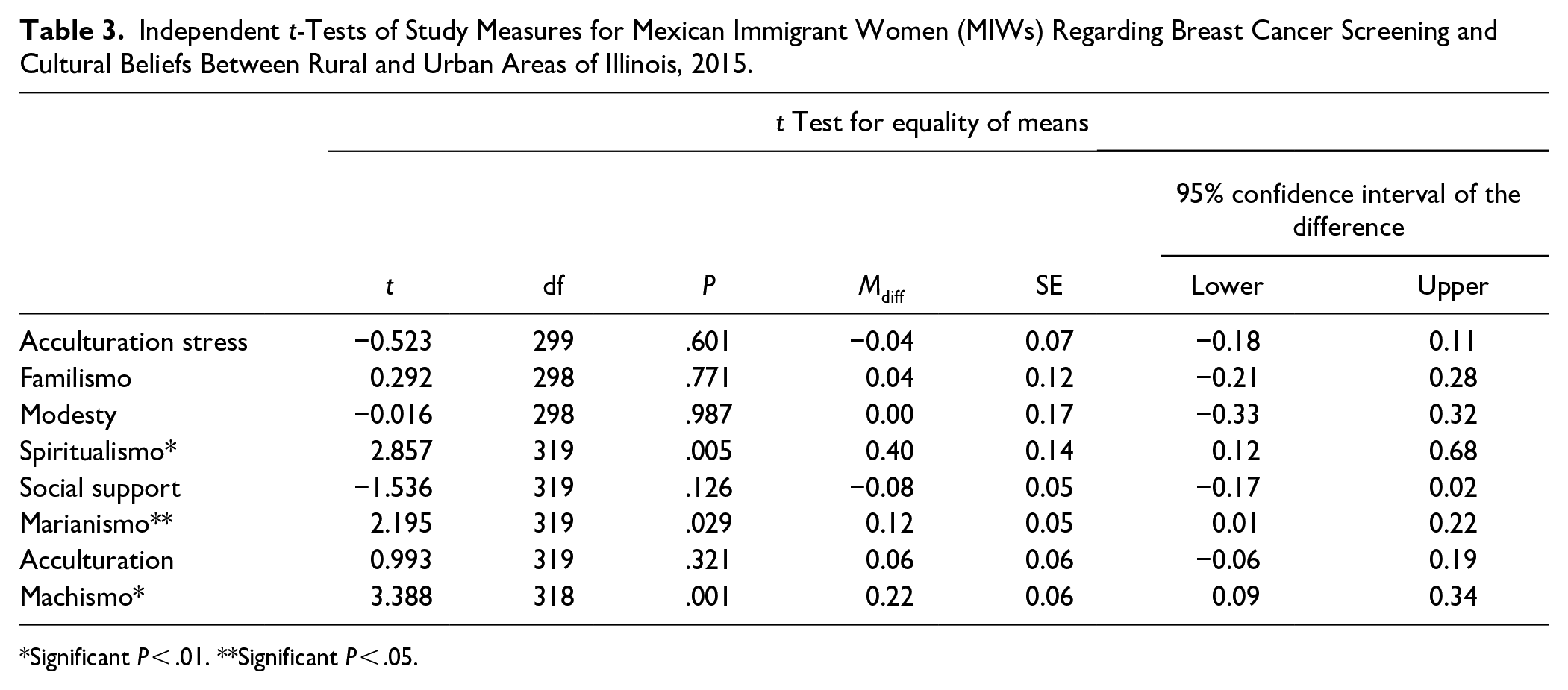
Significant P < .01. **Significant P < .05.
Screening rates for breast cancer were higher among rural MIWs, with 54.4% having had a mammogram compared to 45.6% of urban MIWs (P = .023). Notably, among those who underwent mammograms, rural women were more likely to have had multiple screenings, with 60.4% reporting four or more mammograms, compared to 39.6% of urban women (Table 4). Despite higher screening rates, rural participants faced significant barriers such as a lack of doctor recommendations (55.0% rural vs 45.0% urban, P = .001), procrastination (56.6% rural vs 43.4% urban, P = .010), and embarrassment during exams (67.9% rural vs 32.1% urban, P < .001) (Table 4).
Crosstabulation of Mammography, Cancer Belief, Modesty, Crisis, and Family Support Items Among Illinois Mexican Immigrant Women in 2015(Rural Vs Urban).

P < .05. **P < .01.
Family involvement emerged as a significant factor influencing health behaviors. A greater proportion of rural women reported engaging in family discussions about cancer screenings (61.7% vs 38.3% in urban areas) and receiving family assistance in finding health information (59.8% vs 40.2%), suggesting that while cultural norms may present barriers to screening, strong familial networks can facilitate engagement with healthcare services (P < .001) (Table 4). The primary reasons cited for not participating in mammography screening included a lack of physician recommendation (77.8% in rural areas vs 22.2% in urban areas, P = .001) and procrastination (56.6% rural vs 43.4% urban, P = .010). Additionally, rural participants reported more discomfort with discussing their bodies with doctors (60.7% rural vs 39.3% urban, P = .017) and greater embarrassment during breast exams (67.9% rural vs 32.1% urban, P < .001). Despite these challenges, rural MIWs reported higher family engagement in health-related conversations, indicating that family support could mitigate some of these challenges (P < .001) (Table 4).
Discussion
The study found that rural MIWs reported stronger adherence to traditional cultural beliefs, which appeared to correlate with differences in health behaviors, such as mammography rates and regular screenings. While these cultural factors may help explain some of the disparities in screening behaviors, it is important to recognize that other factors, such as access to healthcare services and socioeconomic status, also play a meaningful role. The rural MIWs who did not participate in mammography cited a lack of doctor recommendations as a major barrier. The rural MIWs reported greater embarrassment related to breast examinations and discussions with doctors, yet they also noted stronger family support in navigating health information. This suggests that while cultural norms around modesty and gender roles might act as barriers to screening, the supportive role of family networks could help to mitigate these barriers to some extent.
The observed interplay between cultural beliefs and screening practices in rural MIWs aligns with the findings of Abraído-Lanza et al 8 who conducted a comprehensive review of the literature on acculturation and health among Latino populations in the United States. Abraído-Lanza et al 8 emphasized the complex relationship between acculturation and health behaviors among Latinas, highlighting that the process of acculturation involves adopting the cultural norms and practices of the host country, which can have both positive and negative effects on health outcomes. Our current study contributes a unique perspective by illustrating these dynamics specifically in rural settings, where traditional beliefs such as spiritualismo, machismo, and marianismo have a more pronounced impact on healthcare decisions among MIWs.
Additionally, our study suggests a potential link between these practices and specific cultural norms, indicating that traditional beliefs may play a meaningful role in shaping health-seeking behaviors. This understanding of cultural factors within rural MIW communities can inform the development of targeted interventions to address healthcare disparities and promote culturally sensitive healthcare practices.
In terms of breast cancer risk perception, the study reveals a noticeable difference between rural and urban MIWs. This aspect is particularly relevant when considering the qualitative emphasis placed by Szalacha et al 9 on the need to understand and leverage cultural beliefs to positively influence screening practices among Mexican-born Latinas. While Szalacha et al 9 highlighted the qualitative aspects, the quantitative approach of the current study brings a complementary perspective, showing how deeply ingrained cultural beliefs can potentially impact risk perception and screening frequency.
The study also sheds light on the barriers to screening, such as doctor nonrecommendation and embarrassment during exams, which are more noticeable in rural areas. This finding resonates with the observations of Ramirez et al 10 regarding discomfort during medical exams among Hispanic women but expands the context to underline the rural-urban divide. The research highlights the importance of a lack of doctor recommendations and embarrassment during medical exams as notable barriers, particularly in rural areas. This observation aligns with Talham et al’s 11 findings on healthcare access and knowledge barriers. Our study’s distinct contribution lies in its focus on how these barriers are magnified in rural settings, emphasizing the need for targeted healthcare strategies.
Recruiting hard-to-reach populations like rural MIWs poses significant challenges, as highlighted by recruitment strategies used in previous research involving community leaders at all stages of research. 12 Engaging community leaders and employing culturally sensitive recruitment methods such as Participatory Learning and Action (PLA) and community partnerships can facilitate ethical research with hard-to-reach populations. For example, involving trusted community members and using culturally appropriate spaces for recruitment can significantly enhance participation and retention. Understanding and accommodating participants’ knowledge and experiences render research more culturally sensitive and relevant, thereby allowing researchers to gain a deeper understanding of the health issues faced by immigrants and other vulnerable populations. This approach was employed by Vahabi et al 13 and Aglipay et al, 14 who used community partnerships to successfully recruit and retain participants.
In the context of rural MIWs, structural barriers such as lack of health insurance, transportation challenges, and limited access to healthcare resources can impede breast cancer screening. 12 These barriers are compounded by cultural contexts, including fatalismo, familismo, and marianismo, which interact with structural contexts to affect screening behavior. The study underscores the importance of understanding the interactive influence of these factors to develop effective interventions. Structural barriers and cultural beliefs must be addressed simultaneously to improve healthcare outcomes. For instance, addressing transportation issues and providing mobile mammography units in rural areas can help overcome access barriers, while culturally tailored education programs can address fatalistic beliefs and emphasize the importance of regular screenings.
The role of family in health decisions emerged as an influential factor, particularly in rural areas. This finding aligns with Documét et al’s 15 research on the influence of social support in cancer screening among Latinas. Sonubi et al 4 further supports this observation by underlining the importance of familial and social networks in healthcare engagement among Latinas. Our study adds to this narrative by demonstrating how family influence is more evident in rural MIWs, impacting both their awareness and engagement in breast cancer screening.
The study emphasizes the need for healthcare policies and practices to consider the diverse needs of MIWs, particularly in underserved rural areas. Healthcare providers must be aware of the cultural beliefs prevalent among rural MIWs. This awareness can guide the development of culturally sensitive approaches to encourage open communication, reduce barriers to screening, and improve breast cancer screening rates.4,5 Policies should also address disparities in healthcare access between rural and urban areas, ensuring the availability of mammography services in rural regions and supporting the training and recruitment of culturally competent healthcare providers. 4 Community initiatives that involve family-oriented strategy-targeted outreach programs, educational campaigns, and mobile mammography units can help promote screening behaviors among underserved populations. 5 The study’s results highlight the importance of tailored healthcare strategies that consider the complex interplay of cultural beliefs, geographical context, and familial support, ultimately striving for equitable health outcomes among MIWs in both rural and urban settings.
Recent healthcare policy changes, including the expansion of Medicaid and the Patient Protection and Affordable Care Act (ACA), have potentially impacted access to healthcare services, particularly preventive screenings such as mammography. 16 These policy changes aimed to extend health insurance coverage to underserved populations, including Mexican immigrant women. 17 As a result, many previously uninsured or underinsured Mexican immigrant women may have gained access to healthcare services, including mammograms. The ACA mandates that health insurance plans cover a range of preventive services without cost-sharing, making mammography screenings more financially accessible. 18 Moreover, these policy changes have encouraged healthcare providers to recommend preventive screenings to eligible patients, potentially addressing the barrier of doctor nonrecommendation identified in the study. 19
Building upon the possible impact of recent healthcare policy changes, the development of culturally tailored interventions to improve breast cancer screening rates among Mexican immigrant women remains essential. 20 These interventions can utilize the benefits of expanded coverage and address disparities effectively. 20 One key aspect is the inclusion of cultural competency training for healthcare providers, ensuring they understand and address the unique cultural beliefs and preferences of Mexican immigrant women. 21 This training focuses on effective communication and building trust with patients from diverse backgrounds.
Limitations
Despite its several strengths, this study’s limitations include its focus on specific areas in Illinois and a relatively small sample size, underscoring the need for more extensive and diverse research. Future studies should explore longitudinal trends to capture the evolving nature of cultural and healthcare factors influencing MIWs’ health behaviors. Additionally, investigating the impact of recent policy changes on these communities’ health practices could provide valuable insights for more inclusive and effective healthcare strategies. A larger and more diverse sample size, potentially including participants from various regions and backgrounds, would offer a more comprehensive understanding of these factors. Moreover, future research should examine the interactive effects of structural barriers and cultural contexts on breast cancer screening practices among MIWs to inform more targeted and effective interventions.
Conclusion
Breast cancer disparities among Latinas, particularly in rural areas and among foreign-born individuals, highlight the critical need for culturally sensitive interventions and accessible healthcare services. Our study reveals that while rural Mexican immigrant women (MIWs) exhibit a higher affinity for traditional beliefs and face significant screening barriers, they also report higher mammography rates and stronger family support. These findings underscore the importance of considering cultural contexts and health access disparities in policy.
Footnotes
Acknowledgements
Financial support was provided by the University of Oklahoma Libraries’ Open Access Fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the University of Illinois Urbana Champaign Center for Advanced Studies (CAS)