
Abstract
Introduction/Objectives:
We aimed to investigate the effect of family structure on depression program outcomes for adolescents enrolled in a depression-focused, primary care-based collaborative care program.
Methods:
This was a retrospective study of primary care patients ages 12 to 18 years seen at a Midwestern academic center with data obtained by medical record review. We used logistic regression models to assess the effect of family structure on program graduation and achievement of a single Patient Health Questionnaire 9–Modified for Adolescents (PHQ-9M) score <5 at any time while enrolled.
Results:
Adolescents were divided into 2 groups, Both Parents in Household (n = 179) and Parents Not Together (n = 161). The Both Parents in Household group had higher rates of graduation (38.0% vs 23.6%, P = .005) and achieving single PHQ-9M scores <5 (64.1% vs 46.2%, P = .002) than the Parents Not Together group.
Discussion:
Youth residing with both parents had higher rates of successful outcomes in a depression-focused collaborative care program.
Introduction
Families in which parents live in separate households due to divorce or separation are common. In 2015, 27% of United States children had a parent outside of their household. 1 The impact of parental living arrangements on adolescents’ mental health is poorly understood.
Previous studies investigating child and adolescent mental health in relation to parental living arrangement have shown mixed results. One study found that children 10 to 18 years of age in joint custody arrangements had similar rates of psychological symptoms compared to those in intact two-parent families, whereas children in sole parental care demonstrated higher rates of psychological symptoms than those in joint custody. 2 Two studies showed that the risk for major depression in young adulthood has been associated with family disruption, especially when divorce occurs in early childhood.3,4 Children in single-parent families also have higher rates of depressive symptoms, potentially related to financial stressors and other demands of single-parent households5,6 and lower socioeconomic status for single parent households. 7 Lastly, children who experienced parental divorce/separation were at increased risk of starting to drink alcohol at all ages, 8 which may also impact adolescent mental health.
Despite evidence for increased mental health risks in youth from families with separated or single parents, the impact of split family structure on treatment outcomes for children with depression, anxiety and alcohol use is not known. This is an important area for emerging investigation, given the high lifetime prevalence (10-15%) of adolescent depression 9 and the increasing use of integrated medical and behavioral health care approaches for extending evidence-based care to this population. 10 By understanding risk factors for poor outcomes and low depression remission rates, such as vulnerabilities in family structure, additional services may be designed and mobilized for this at-risk population, incorporating new strategies into integrated care programs serving youth with a diverse range of family structures.
This study sought to evaluate the effect of parent relationship and family structure on depression outcomes for adolescents enrolled in a collaborative care program. We hypothesized that adolescents in intact two-parent families would show greater likelihood of improvement in the collaborative care program as measured by achievement of a single Patient Health Questionnaire 9–Modified for Adolescents (PHQ-9M) score <5 and program graduation rate. This hypothesis emerged from observations in clinical practice in which split families may have differing opinions on what type of care is needed, or whether it is needed at all. Additionally, split families may require greater coordination and need assistance with making and attending appointments, leading to greater vulnerabilities in the delivery of care.
Methods
This study was a retrospective review of clinical records from adolescent patients at our institution who enrolled in a collaborative care program known as EMERALD (Early Management and Evidence-Based Recognition of Adolescents Living with Depression). 11 The present analyses are based on a convenience sample of 340 adolescents (273 female, 67 male) who enrolled in the EMERALD program between 2011 and 2018 with a mean age of 15.6 ± 1.6 years (range 12.1–18.8 years). The study was approved by the Mayo Clinic Institutional Review Board. In accordance with Minnesota Statute 144.335, only adolescents whose parents (or themselves) had provided research authorization to review their child’s medical records for general research studies were included in this study.12,13
The EMERALD Program, 11 which opened in July 2011, is designed to treat adolescents with depression in the primary care setting using a collaborative care model located in Rochester, MN, USA. The EMERALD care team consists of primary care providers (PCPs), child and adolescent psychiatrists (CAPs), and behavioral health care coordinators (BHCCs), who are registered nurses trained specifically for the program. After identifying concerns for depressive symptoms, the PCP makes a referral to EMERALD. The BHCC then meets with patient and parent to obtain history and baseline clinical rating scales. The BHCC communicates by telephone with the patient, initially weekly and then less frequently as the patient’s condition improves to review progress, side effects, and response to treatment, and to set and monitor behavioral activation and other self-care goals. The BHCC also communicates regularly with the patient’s parent(s) and the patient’s therapist to obtain their observations. The BHCC and CAP meet weekly for systematic case review. They use clinical history and outcome measures to review the diagnosis and initial recommendations for care, and over time they track progress and recommend changes to the care plan, which are implemented by the PCP. Face-to-face consultation with the CAP is available for patients whose diagnoses or comorbidities are unclear, or who do not respond to initial treatment. Psychotherapy may be provided by therapists within the institution, or by therapists in the community separate from EMERALD.
All adolescents between the ages of 12 and 18 years treated in our institution’s primary care clinics who have a PHQ-9M score of 10 or greater and have a depressive disorder diagnosis (major depressive disorder [MDD], persistent depressive disorder, adjustment disorder, or unspecified depressive disorder) are eligible to participate in EMERALD. Initially, the program was designed to serve adolescents ages 13 to 18, but in December 2012, it was expanded to include 12-year-old patients. Exclusion criteria for EMERALD include a diagnosis of bipolar disorder, severe cognitive disability, primary psychotic disorder, or substance use disorder requiring primary chemical dependency treatment, as these typically require specialty services beyond what the collaborative care program offers. Consistent with its purpose of addressing depressive symptoms in real-world primary care settings, adolescents with other comorbidities may enroll, including those with anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), learning disorders, and externalizing disorders.
“Graduation” from EMERALD requires PHQ-9M scores less than 5 in 3 consecutive months. Upon graduation, a relapse prevention plan is generated for the patient. Patients who do not respond to BHCC contacts for 2 consecutive months are considered lost to follow-up. Patients also may withdraw from the program by informing program staff that they no longer want to participate. Patients who need a higher level of subspecialty care while enrolled in EMERALD were paused from the program until completion of a higher level of care. Adolescents who remain in EMERALD for more than 12 months without meeting graduation criteria typically are referred to specialty adolescent psychiatry care. Patients’ care could also be transitioned to specialty providers at an earlier stage if recommended by the care team based on clinical need.
As an outcome of depressive symptom severity, our study used the Patient Health Questionnaire Modified for Teens (PHQ-9M).14,15 The adolescent version is similar to the adult scale, but with modified, developmentally-appropriate language. It consists of 9 items and is scored on a Likert-type scale from 0 (“not at all”) to 3 (“nearly every day”). A score cutoff of 5 indicates mild depression, 10 moderate to severe depression, and 15 severe depression.
Screening for substance abuse was completed using the Car, Relax, Alone, Forget, Family/Friends, and Trouble (CRAFFT), 16 a validated substance use screening tool for adolescents aged 12 to 21 years. It consists of 2 parts: A and B. If patient answers no to all questions in Part A then they are asked only 1 question in Part B, which inquires about being in a car with someone under the influence of the alcohol. If they answer “yes” to questions in Part A, then 6 questions in Part B are asked.
The Spence Children’s Anxiety Scale–Child (SCAS-C) 17 is a validated self-report questionnaire to screen for symptoms of anxiety in children and adolescents. It consists of 38 items with each item rated on a 4-point Likert-type scale ranging from 0 (never) to 3 (always). The Spence Children’s Anxiety Scale–Parent (SCAS-P) is a validated 38-item parent-report measure of anxiety symptoms for children and adolescents.18 -23 Each item is rated on a 4-point Likert-type scale ranging from 0 (never) to 3 (always).
The Mood Disorder Questionnaire, Adolescent Version (MDQ-A) 24 is a validated self-report questionnaire with 13 binary, “yes/no” questions screening for bipolar disorders derived from DSM-IV criteria. The Vanderbilt Diagnostic Parent Rating Scale (VADPRS) 25 was used to assess for attention-deficit/hyperactivity disorder. This instrument is used to assess inattention (9 items), hyperactivity/impulsivity (9 items) and 3 comorbidities (oppositional defiant disorder, conduct disorder, anxiety, and depression). The VADPRS uses a Likert-type scale with each item rated from “never” to “always.”
Our primary program-related outcome was a dichotomous variable of whether patients completed the EMERALD program (requiring PHQ-9M scores <5 in 3 consecutive months). As a secondary outcome of symptomatic improvement, we examined whether patients achieved a single PHQ-9M score <5 at any point during EMERALD participation, indicating any improvement, even if not sustained. The study team reviewed each patient’s EMERALD care coordination notes for details related to family structure and composition. The primary independent variable, family structure, was operationalized as a dichotomous variable. Patients were classified into Both Parents in Household or Parents Not Together groups based on descriptions of the family living arrangements given by the patient and parent and recorded in the clinical record. If a patient reported that they lived with 1 parent only, were co-parented and oscillated between 2 different households, or resided with another guardian such as a grandparent, foster parent, or another adult, they were classified as Parents Not Together. The categories of single parent and split custody has been utilized in previous studies evaluating impact of family structure on psychological symptoms,2 -7 and “other guardians” represented a unique caregiving arrangement not previously studied. Additional demographic variables such as age at EMERALD enrollment, gender, race, and ethnicity were also extracted.
Clinical characteristics at the time of enrollment were extracted from the BHCC EMERALD enrollment note and the CAP supervisory review note. These included primary diagnosis (as determined by the CAP), prior antidepressant medication use, timing of antidepressant initiation (dichotomized to ≥3 months or <3 months prior to enrollment), prior psychotherapy, and scores for the PHQ-9M, MDQ-A, SCAS, VADPRS, and CRAFFT. Variables related to participation in EMERALD included number of days enrolled, number of attempted contacts by staff, and number of successful contacts.
Individual socioeconomic status (SES) was measured using the validated HOUsing-based SocioEconomic Status (HOUSES) Index. 26 We collected the most current addresses of study participants which were matched to real property data of individual housing units from the county assessor’s office to formulate the HOUSES Index. Principle components factor analysis identified 4 real property variables (housing value, square footage of the housing unit, number of bedrooms, and number of bathrooms) that were then formulated into a standardized HOUSES Index. Higher HOUSES Index scores (z scores) correspond to higher SES. 26 Since the original validation of HOUSES Index, it has shown to predict a broad range of health outcomes in children and adults, including acute and chronic health outcomes, behavioral health, and mortality.27 -30
Statistical analysis
Baseline demographic and clinical characteristics were compared between Both Parents in Household and Parents Not Together groups using Fisher’s exact tests for categorical variables and independent samples t-tests for continuous variables. For the primary aim, we conducted logistic regression, with family structure (Both Parents in Household vs Parents Not Together) as the primary independent variable (predictor) and EMERALD graduation as the dependent (outcome) variable. In this model, we adjusted for SES (HOUSES Index z-score) and 3 clinical variables of interest. These included 1 selected a priori for potential impact on outcome (enrollment PHQ-9M score) as well as 2 clinical variables empirically found to differ between Both Parents in Household and Parents Not Together groups (enrollment CRAFFT score, prior antidepressant use). These variables were all entered together for the analysis. The discrimination of this model was measured using the c-statistic. For the secondary aim, we conducted a separate logistic regression, with family structure as the independent variable and achievement of a single PHQ-9M score <5 as the dependent variable, again with SES (HOUSES Index z-score) enrollment PHQ-9M score, enrollment CRAFFT score, and prior antidepressant use as covariates. For these models, we assessed for an interaction between socioeconomic status and family structure; however, no significant interactions were found (P values > .5).
Subgroups of the Parents Not Together group were compared to Both Parents in Household with univariate analysis for the outcomes of single PHQ-9M score < 5 and EMERALD graduation. This analysis was adjusted for multiple comparisons using the false-discovery rate method.
No imputation was done for missing data in Table 2. Patients missing data were excluded from that respective analysis (ie, those missing MDQ-A scores were excluded from the comparison of MDQ-A scores between groups). All analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Demographic characteristics are presented in Table 1. There were 179 adolescents (144 female, 35 male) classified in the Both Parents in Household group, and 161 adolescents (129 female, 32 male) in the Parents Not Together group. There was a significant difference in race distribution between groups (P = .002), with the Both Parents in Household group having a higher proportion of White adolescents (84.9%) than the Parents Not Together group (72.1%). However, the groups did not differ significantly in ethnicity (P = .096). Adolescents in the Parents Not Together group had a higher mean number of siblings (P = .005) and lower SES (mean HOUSES z-score: −1.0 ± 2.7 vs 1.7 ± 3.8; P < .001) than those with Both Parents in Household.
Demographic Characteristics of Both Parents in Household and Parents Not Together Groups.
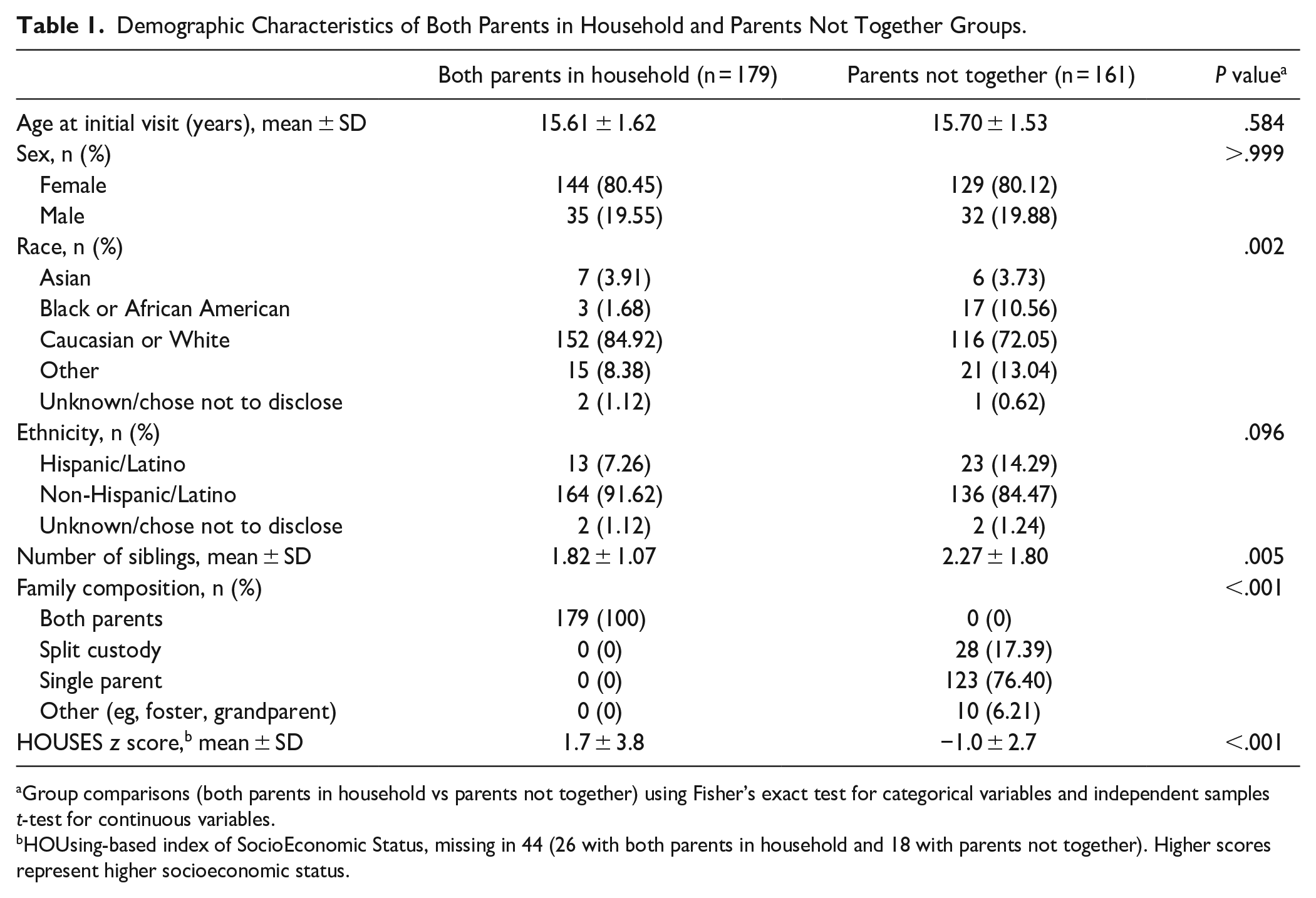
Group comparisons (both parents in household vs parents not together) using Fisher’s exact test for categorical variables and independent samples t-test for continuous variables.
HOUsing-based index of SocioEconomic Status, missing in 44 (26 with both parents in household and 18 with parents not together). Higher scores represent higher socioeconomic status.
Clinical characteristics of the 2 groups at the time of enrollment are presented in Table 2. The groups did differ in distribution of primary diagnosis (P < .001), notable for a higher proportion of Parents Not Together patients having an MDD diagnosis (80.8%) than Both Parents in Household patients (73.2%), and a higher proportion of Both Parents in Household patients having a primary anxiety diagnosis (11.7%) than patients in the Parents Not Together group (0.6%). A greater proportion of patients in the Both Parents in Household group had prior antidepressant medication use (53.1%) than in the Parents Not Together group (33.5%; P < .001). However, among those who had prior antidepressant use, groups did not differ in the proportion that initiated antidepressant pharmacotherapy in the past 3 months (P = .480). CRAFFT scores were higher in the Parents Not Together group (1.02 ± 1.55 vs 0.46 ± 1.05, P < .001).
Clinical Characteristics of Both Parents in Household and Parents Not Together Groups.
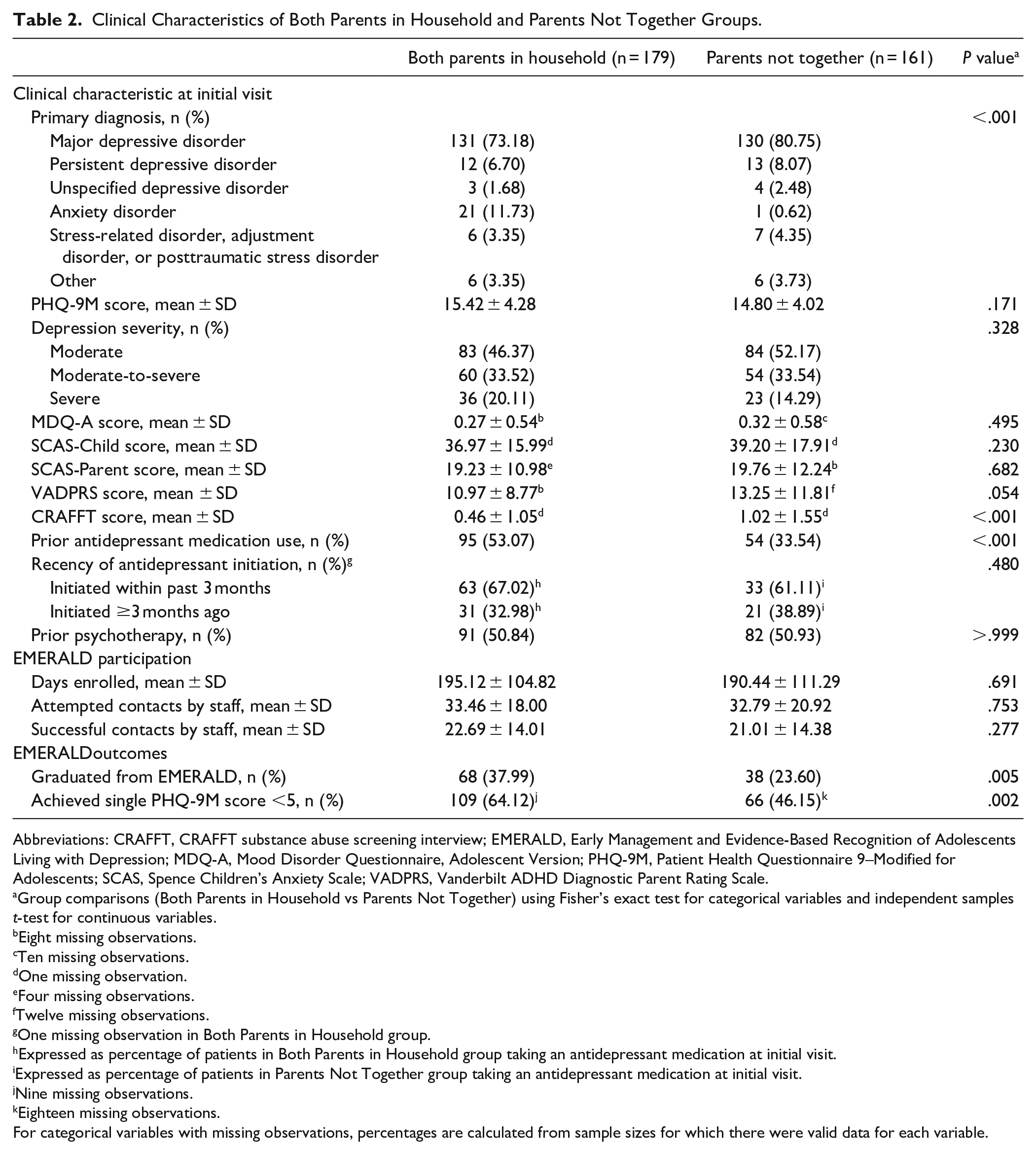
Abbreviations: CRAFFT, CRAFFT substance abuse screening interview; EMERALD, Early Management and Evidence-Based Recognition of Adolescents Living with Depression; MDQ-A, Mood Disorder Questionnaire, Adolescent Version; PHQ-9M, Patient Health Questionnaire 9–Modified for Adolescents; SCAS, Spence Children’s Anxiety Scale; VADPRS, Vanderbilt ADHD Diagnostic Parent Rating Scale.
Group comparisons (Both Parents in Household vs Parents Not Together) using Fisher’s exact test for categorical variables and independent samples t-test for continuous variables.
Eight missing observations.
Ten missing observations.
One missing observation.
Four missing observations.
Twelve missing observations.
One missing observation in Both Parents in Household group.
Expressed as percentage of patients in Both Parents in Household group taking an antidepressant medication at initial visit.
Expressed as percentage of patients in Parents Not Together group taking an antidepressant medication at initial visit.
Nine missing observations.
Eighteen missing observations.
For categorical variables with missing observations, percentages are calculated from sample sizes for which there were valid data for each variable.
In the overall sample, 106 patients graduated from the program; this included 68 adolescents in the Both Parents in Household group and 38 adolescents in the Parents Not Together group. The graduation rate for Both Parents in Household group (38.0%) was significantly higher than for Parents Not Together group (23.6%, P = .005). The multivariable logistic regression model containing family structure, enrollment PHQ-9M score, prior antidepressant use, CRAFFT score, and HOUSES z-score as predictor variables was significantly predictive of the binary outcome of graduation or lack of graduation (omnibus test: χ2 = 11.40, df = 5, P = .044). In this model (Table 3a), family structure (Both Parents in Household vs Parents Not Together) was a significant predictor (OR = 1.78, 95% confidence interval [CI] 1.02-3.13; P = .044). Other covariates (enrollment CRAFFT score, PHQ-9M score, HOUSES z score, and prior antidepressant use) were not statistically significant predictors.
Multivariable Logistic Regression Models for EMERALD Program Outcomes.

Abbreviations: CI, confidence interval; CRAFFT, CRAFFT substance abuse screening interview; EMERALD, Early Management and Evidence-Based Recognition of Adolescents Living with Depression; PHQ-9M, Patient Health Questionnaire 9–Modified for Adolescents.
Both parents in household versus Parents not together.
The proportion of patients achieving a single PHQ-9M score <5 during EMERALD participation also was higher for Both Parents in Household adolescents (64.1%) than for Parents Not Together adolescents (46.2%, P = .002). The multivariable logistic regression model containing family structure, enrollment PHQ-9M score, prior antidepressant use, CRAFFT score, and HOUSES z-score as predictor variables was significantly predictive of the binary outcome of achievement or non-achievement of a single PHQ-9M score less than 5 at any time during EMERALD participation (omnibus test: χ2 = 13.93, df = 5, P = .016). In this model (Table 3b), family structure was a significant predictor (Both Parents vs Parents Not together, OR = 2.17, 95% CI 1.26-3.73; P = .005), as was enrollment PHQ-9M score (per 1 point, OR = 0.94, 95% CI 0.88-0.99; P = .033), while CRAFFT score (P = .817), HOUSES z-score (P = .937), and prior antidepressant use (P = .407) were not significant predictors. The c-statistic for the graduation model was 0.627, and for PHQ-9M model was 0.629. When subgroups of the Parents Not Together group were analyzed separately and compared to Both Parents in Household, only the Single Parent subgroup was found to have significantly lower graduation rates (22.0% vs 38.0%, P = .019) and achieving a single PHQ-9M score <5 (42.2% vs 64.1%, P = .002).
Discussion
Collaborative treatment programs involving primary care providers and mental health professionals are more effective than care as usual 31 and are cost-effective 32 in the treatment of adolescent depression. Family structure was a significant predictor of both successful completion of the program and achieving a single PHQ-9M <5 for adolescents in our collaborative care program. To our knowledge, this is the first study to evaluate how family structure affects depression treatment in a large, community-based, adolescent population.
Our study demonstrated that although adolescents from both family structure groups had comparable depression severity and other baseline clinical scores, the children of parents living together had significantly higher rates of outcomes related to improvement in depressive symptoms while in the EMERALD program than did children of parents not living together. In a subgroup analysis, these findings were confirmed with Single Parents versus Both Parents In Household, but not with other subgroups of Parents Not Together, which may in part be due to low sample sizes in the split custody and “other” groups. Lower PHQ-9 score at enrollment was associated with achieving a single PHQ-9M score of <5 but not associated with EMERALD completion, so enrollment PHQ-9M was a predictor of having 1 score <5, but not a predictor of maintaining a score <5.
Both groups had similar metrics of participation in the program, such as duration of enrollment and contacts with EMERALD care staff. However, it is possible that children of parents living together had a greater degree of unmeasured parental participation in programming or attendance at their treatment sessions, which could have had an effect on outcomes. Other studies have found that relationship status in diverse family structures affects adolescents’ mood. 33 Loss of contact with parents is a significant risk factor associated with depressive and externalizing disorders in adolescents. 34 In our study, it is unclear whether adolescents with Parents Not Together had less contact with their caregivers than those with Both Parents in Household. An unexpected finding was that children of parents living together were more likely to have been prescribed an antidepressant medication prior to EMERALD, yet the proportion of adolescents previously engaged in psychotherapy was comparable between the 2 groups. It is possible that parents living together were more agreeable to starting a medication for their child in contrast to parents not living together; however, prior antidepressant use did not significantly predict either outcome. Prior work has found prescribers to be more hesitant to start a medication if parents are in disagreement about medication initiation. 35 There may be unmeasured, poorly understood factors impacting prescriber–parent interactions and decision making in the care of depressed adolescents. This highlights the need for prospective studies to clarify particular reasons for differences in treatment methods among patients with differing family structures. It has been observed that transitions to new family systems (divorce, separation, parental death) can be associated with children and adolescents exhibiting higher levels of externalizing problems. 36 However, socialization theory posits that parents can have lasting and positive influence on their children regardless of the family structure in which the child is raised. 37 Parents who practice warmth, closeness, close monitoring as well as effective discipline strategies may promote capability for adjustment in their children, independent of family structure. 38
In our study, adolescents with Parent Not Together had a higher baseline risk of having a primary diagnosis of MDD and those with Both Parents in Household had a higher baseline risk of having a primary anxiety diagnosis. Nevertheless, family structure groups did not differ on scales of depressive, anxiety, or ADHD symptom severity at baseline; thus, it is unlikely that these co-morbidities impacted our study outcomes. Future prospective studies aiming to characterize and measure the severity of depressive and anxiety symptoms in diverse adolescent populations are needed to elucidate how these internalizing symptoms are manifested among youth living in different family structures. Our study also found that adolescents with depression whose parents were not together scored higher on the CRAFFT questionnaire in comparison to adolescents whose parents were together. This finding is consistent with other studies that report that people who have experienced parental separation/divorce in their childhood were more likely to report alcohol initiation at a younger age as compared peers.39 -41
Our study was strengthened by adjustment for socioeconomic status in the analysis using the HOUSES Index. However, our study has several important limitations. The retrospective study design and extraction from clinical records is prone to biases, including inconsistent data entry and incomplete data. Our definition of children living with Parents Not Together was broad and included children living with 1 parent only, children with joint physical custody, and children living with relatives or others. There is a large diversity of family structures, 42 as was reflected in our sample. However, to better understand the mental health correlates of children’s living arrangements, future studies with larger sample sizes should assess family structure with greater nuance than 2 broadly characterized groups. We also were unable to assess for the presence or absence of parental conflict within the family structure. It would be helpful to understand if the level of conflict between parents is similar for children whose parents are together versus those whose parents are not together. Previous studies have demonstrated that parents who live separately are more prone to mental health issues, financial issues, and familial discord, which can impact a child’s wellbeing, 43 and parental conflict has been shown to impact adolescent depression outcomes.44,45 However, the parents’ relationship with the child can be more important for the child’s mental health than their relationship with each other. 46 Additionally, the ability of parents to collaborate regarding their child’s care after separation can have significant influence on a child’s wellbeing. Measurement of parental conflict and amicability after separation would necessitate prospective longitudinal studies with pre- and post-separation assessments. Lastly, our study did not track if psychotherapy was provided by therapists in the institution or outside the institution, and this could have an impact on program outcomes as the psychotherapy could have varied in duration or intensity.
Conclusions
In a sample of adolescents ages 12 to 18 years with moderate-to-severe depression who enrolled in a collaborative care program for treatment of depressive symptoms, patients with parents together did not differ from patients whose parents were not together on the majority of baseline clinical characteristics. However, patients who lived with both parents were more likely to complete the treatment program, and to achieve a PHQ-9M score <5 while enrolled in the program, than did adolescents whose parents were not together. Substance use differed between family structure groups and may affect some outcomes related to successful depression treatment. Further studies are needed to better understand how family structure specifically affects depression outcomes and treatment response in children and adolescents whose parents live together versus whose parents are not together. By understanding these important factors, targeted treatments, community services, and guidelines to better inform policies regarding custody may provide youth with a secure network to aid in depression recovery. Future studies with larger sample sizes will be able to analyze diverse subgroups of youth whose parents are not together with appropriate statistical power. Future research should also evaluate metrics of parental relationship quality, family conflict, and parenting behaviors and their impact on treatment outcomes for youth with depression.
Footnotes
Acknowledgements
This study was made possible using the resources of the HOUSES program of the Precision Population Science Lab of the Mayo Clinic. The content of this article is solely the responsibility of the authors and does not represent the official views of the HOUSES program.
Abbreviations
ADHD, attention-deficit/hyperactivity disorder
BHCC, behavioral health care coordinator
CAP, child and adolescent psychiatrist
CRAFFT, CRAFFT substance abuse screening interview
EMERALD, Early Management and Evidence-Based Recognition of Adolescents Living with Depression
MDD, major depressive disorder
MDQ-A, Mood Disorder Questionnaire, Adolescent Version
OR, odds ratio
PCP, primary care provider
PHQ-9M, Patient Health Questionnaire 9–Modified for Adolescents
SES, socioeconomic status
SCAS, Spence Children’s Anxiety Scale
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Magdalena Romanowicz, Brian Lynch, Kristin Mara, Aiswarya L. Nandakumar. The first draft of the manuscript was written by Magdalena Romanowicz, Brian Lynch and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul E. Croarkin has received research grant support from Neuronetics, Inc., NeoSync, Inc., and Pfizer, Inc. He has received grant in-kind (equipment support for research studies) from Neuronetics, Inc. and MagVenture, Inc. He received grant in-kind support from Assurex Health for supplies and genotyping. He has served as paid consultant for Engrail Therapeutics, Myriad Neuroscience, Procter & Gamble Company, and Sunovion. Jennifer L. Vande Voort has received grant-in-kind from Assurex Health. Charles P. Lewis has received research grant funding from the National Institute of Mental Health of the National Institutes of Health (K23MH127307), the Brain & Behavior Research Foundation (NARSAD Young Investigator Grant No. 27488, Alan G. Ross Memorial Investigator), the American Foundation for Suicide Prevention (Young Investigator Grant YIG-0-108-20), and the Klingenstein Third Generation Foundation (Fellowship in Depression). Dr. Lewis previously served as a site investigator for multicenter trials funded by Neuronetics, Inc., and NeoSync, Inc., and has received a speaker’s honorarium and travel expenses from CentraCare Health System, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
The study (#15-003112) was approved by the Mayo Clinic Institutional Review Board. In accordance with Minnesota Statute 144.335, only adolescents whose parents (or themselves) had provided research authorization to review their child’s medical records for general research studies were included in this study.
Data Availability Statement
The study data is available upon request.