
Abstract
Introduction
Background Knowledge
Improving care delivery through evidence-based continuous quality improvement (QI) is a key component of the patient-centered medical home (PCMH) model.1-3 PCMH team members are expected and encouraged to work together to implement improvement initiatives to enhance the quality of care for their patients. In theory, the PCMH model is well suited to QI work because of its emphasis on longitudinal multidisciplinary patient-centered collaborations.4,5 However, little is still known about QI work within the context of PCMH teams6,7 despite the recent rapid uptake of the PCMH model by large health care systems such as the Veterans Health Administration (VHA). 8 To begin to address this knowledge gap, we initiated an examination of QI work in our local PCMH clinic environment.
Local Context
Our large academic primary care practice converted to a PCMH care model in May 2011. This transformation was part of VHA’s (our clinic’s health care system) large-scale effort to move to the PCMH model (known within VHA as patient-aligned care teams or “PACT”). 8 As part of PCMH implementation, clinical staff engagement in QI work was encouraged via several system-wide initiatives, including distribution of nationally developed materials that encouraged team-centered QI activities and discussions of QI-related topics at national PCMH meetings. 9 In our local context, a variety of QI training opportunities were offered, including (a) basic training in QI-specific methodology (2 separate 2-hour sessions) and (b) a 2-day Yellow-Belt Lean Six Sigma certification program that covered introduction to QI methodology, identification and incorporation of optimal tools to address clinical quality challenges, and completion of a final written test for certification. 10
Additionally, consistent with prior work suggesting that formal training in QI may not be sufficient for successful implementation of improvement techniques,11-13 other QI-specific resources were also provided to staff: at least 2 hours weekly without direct patient care responsibilities, open access to local QI experts, assistance with data gathering, and access to a project coach with Lean Six-Sigma master black belt certification.
Here, we report a case study to better understand how successful resources have been at enabling QI work by PCMH teams. We examine (a) progress of QI work and (b) the barriers and/or facilitators to QI work reported by PCMH teams. We use the Standards for Quality Improvement Reporting Excellence (SQUIRE) framework to report our findings. 14
Methods
Data Collection and Analysis
In order to understand QI project progress and to identify challenges and facilitators to QI work, we performed unstructured interviews with PCMH team members. Face-to-face discussion occurred with at least one member of each of the clinical teams, and in most cases, multiple members. Consistent with frameworks for understanding factors related to successful implementation (eg, RE-AIM: Reach Effectiveness Adoption Implementation Maintenance; CFIR: Consolidated Framework for advancing Implementation Research),15,16 these interviews were used in conjunction with documentation (eg, aim statements) gathered from team members to characterize the team QI work and to identify challenges and facilitators to project implementation.
Ethical Issues
Discussions with team members were informal and voluntary. No names are included in the summary of projects, though local identification of specific team projects is possible. To ensure a variety of perspectives, we sought authorship representation on this article to include facility clinical (SA) and quality (BW) leadership, PCMH providers (SS, MKS), and a PCMH nurse case manager (CW).
Setting
Our work focused on the Louis Stokes Cleveland Veterans Affairs Medical Center outpatient primary care clinic site, an inner-city campus with numerous physician and nurse practitioner trainees. Within the clinic, there are 11 PCMH teams, each with a panel of approximately 1000 patients. Each team is composed of a physician or nurse practitioner provider, a registered nurse (RN) care manager, a licensed practical nurse, and a clerical staff member. Other supporting clinical staff (eg, pharmacists, social workers, mental health providers) are readily available in the clinic setting. The standard VHA comprehensive electronic medical record is used for all clinical documentation.
Results
Quality Improvement Implementation Progress: Alignment With QI Standards?
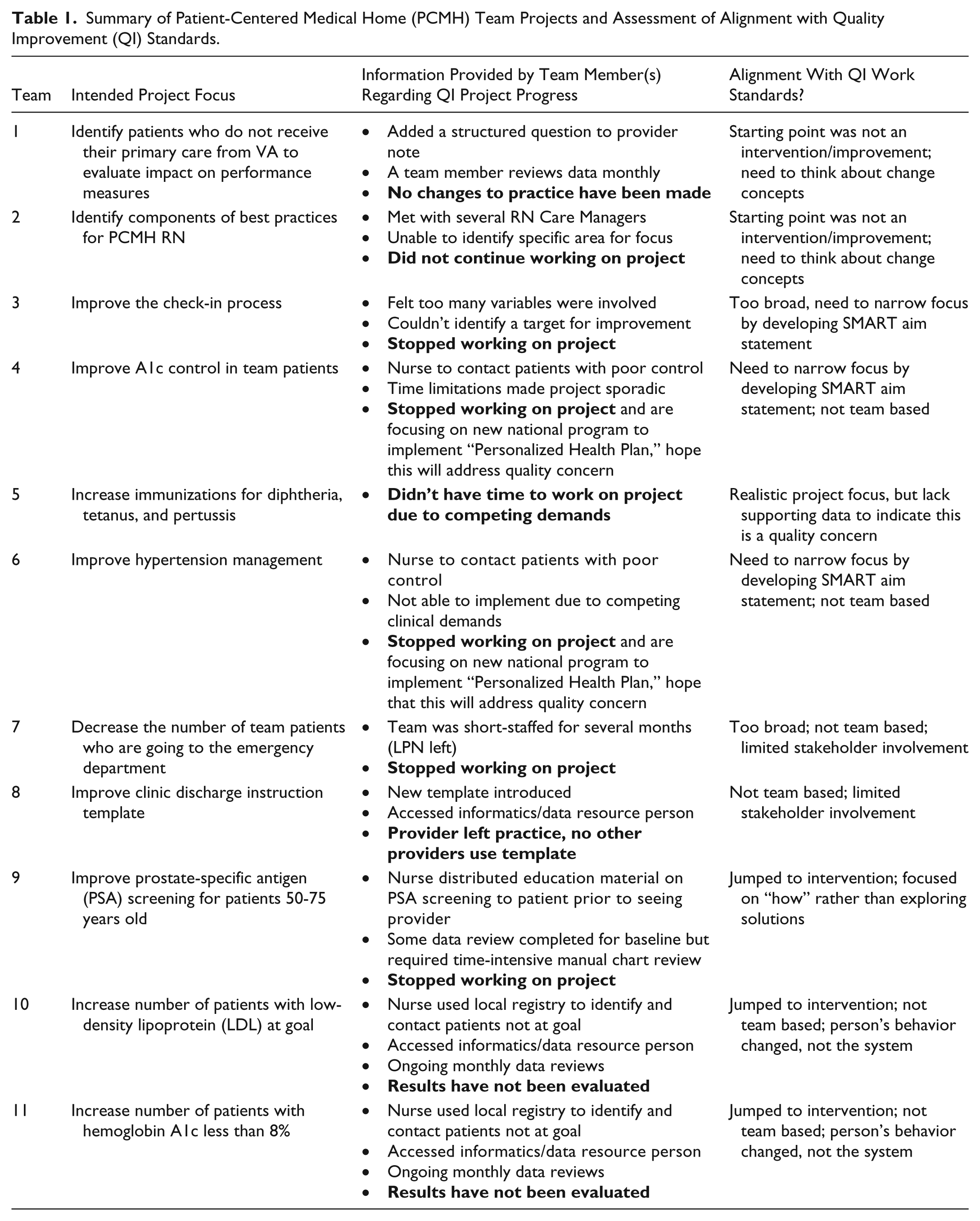
Table 1 presents the key findings related to team QI work. Overall, despite available resources, little progress consistent with QI standards was reported. All eleven PCMH teams in our primary care clinic are represented (100% sample). Each team identified a focus for a team project. The first 2 projects listed in Table 1 did not identify an intervention as a starting point; thus 9 of the 11 projects (82%) demonstrated a choice of project focus consistent with QI work standards. In the 18-month follow-up period, none of the teams developed a formal aim statement for their project. Eight of the 11 teams (73%) developed any type of project plan beyond the initial team discussion. Of the 4 teams that implemented a change (last 4 rows of Table 1, representing 36% of the 11 projects), 2 of the initiatives are still in place, both sustained by the same nurse care manager, though no assessment of the impact of the change has taken place. None of the teams completed assessment of change impact or reported any further changes they had made as a result of project assessment.
Summary of Patient-Centered Medical Home (PCMH) Team Projects and Assessment of Alignment with Quality Improvement (QI) Standards.
Implementation Challenges and Facilitators
Table 2 summarizes themes identified from interviews related to challenges to and facilitators of QI work. Although traditionally accepted facilitators (eg, QI training, leadership buy-in) were in place, QI work remained limited suggesting the barriers outweighed the facilitators. For example, only 1 of the 11 teams (9%) met (only once) with an improvement coach despite awareness and availability of this resource.
Summary of Facilitators and Challenges for Patient-Centered Medical Home Team Project Development and Implementation.

Discussion
Summary
Despite leadership support, formal education sessions, dedicated nonclinical time, and availability of QI coaches, none of the teams completed a single plan–do–study–act cycle. Our findings underscore recent suggestions in the literature that time and educational resources may not be sufficient for frontline teams to engage in QI work.17,18 Based on the feedback from the 11 teams and our observations of the process, we developed a cause–effect diagram (Figure 1) to organize the factors identified in Table 2 structuring the “effect” as the desired outcome: Successful PCMH QI Project. Our goal was to enable action plans to improve the quality and quantity of QI projects in the PCMH teams.

Cause–effect diagram of barriers and facilitators of patient-centered medical home (PCMH) quality improvement (QI) work.
Relation to Other Evidence
The upper half of the Figure 1, “Basic Foundation,” outlines traditionally acknowledged factors (“causes”) of successful QI work that are well established in the literature, for example, get leadership support and buy-in, choose relevant projects5,18 and are consistent with the facilitators identified by our teams. These factors and their subcomponents may provide a necessary foundation for QI work but were not sufficient to propel progress in our clinical environment.
The lower half of Figure 1, “Moving Beyond Basics,” summarizes the novel factors and their subcomponents we identified through this evaluation initiative: Structuring Resources, PCMH Team Development (or “PCMH Maturity”) and System Alignment. The “Moving Beyond Basics” factors align conceptually with the established factors; however, potentially unique nuances are identified in the subcomponents. Further investigation will be necessary to determine the relative importance of these factors and their subcomponents to QI work within the PCMH model and to develop strategies to address them.
Interpretation and Next Steps
Specifically, development of strategies to address the “Moving Beyond Basics” factors and subcomponents may be important to achieving the transformative potential of the PCMH model to facilitate successful QI work. Based on our findings and examination of the existing literature, below we provide some preliminary strategies that may be helpful to translate the 3 identified factors into actionable next steps:
Structuring resources—ensuring that teams do not have competing demands or that time allotment is done in a way to make it conducive for teams to work together. Strategies for implementation may include asking the team to identify a set meeting time each week, facilitating scheduling so that all team members can attend, providing space for the meeting, and requesting routine documentation of the results of the team meeting.
PCMH team development—recognizing the importance of establishing a PCMH teams’ ability to work together, including meeting staffing requirements, before engaging in QI initiatives. This component acknowledges that expectation of QI activities may be counterproductive when teams are struggling with meeting the basic needs of their panel of patients due to staffing deficiencies. Management may be able to assist by providing teams with a timeline of expectations (eg, “WHEN the LPN position is filled, THEN we will plan on beginning our QI meetings . . .”).
System alignment—aligning PCMH QI work transparently with other performance metrics for a clinic or facility. Although addressing this factor at a minimum will require assistance from local quality management/regulatory groups, this would ideally be guided by policy changes at the broader level. For example, development of metrics to evaluate for the presence of QI work in general may be one strategy.
Limitations
This work represents a single-site case study. However, our clinic setting is similar to other large academic primary care practices. In addition, we have 2 years’ experience with integrating the PCMH care model into practice, which provides suggestions for other efforts to enable QI work to become part of routine daily clinic practice, an important consideration as this practice transformation continues to spread throughout primary care.
Conclusions
Successful QI work in the PCMH model may require more than formal education, dedicated time, and leadership support. We offer areas of further investigation and suggestions that may ultimately facilitate the goal of sustainable integration of QI into daily practices of primary care teams.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Veterans Health Administration Office of Academic Affiliations grant titled, “Center of Excellence in Primary Care Education.”