
Abstract
Background:
The Nyakaza-Move-for-Health intervention program was developed in response to the alarming rise in non-communicable diseases (NCDs) globally, in sub-Saharan Africa and South Africa. The rise in NCDs is attributed to the low levels of participation in physical activity (PA) among adolescents. Therefore, this study aimed to design a culturally tailored PA intervention for adolescents, guided by the Intervention Mapping (IM) protocol. The intervention program aims to address the multifaceted determinants of physical activity behavior, promote healthy lifestyles and improve adolescent fitness levels.
Methods:
The Intervention Mapping protocol was applied to design the intervention program. The IM has 6 steps: (1) Needs assessment, (2) developing a logic model of the problem (LMP), (3) Formulating program outcomes and objectives, (4) Program design and production, (5) Generating implementation plan, and (6) Generating intervention evaluation plan. Participants included (n = 48) adolescent learners recruited from 8 (n = 8) participating schools. Adolescent learners participated in focus group discussions (FGD) to identify personal, interpersonal and environmental determinants of physical inactivity. Twenty-six (n = 26) key informant stakeholders participated in a stakeholder engagement workshop (SEW) to determine the motivators and constraints in implementing physical activity interventions.
Results:
The Nyakaza intervention program’s process development involved extensive stakeholder engagement, capacity development training, and integration of community feedback into the design. The intervention included a social marketing campaign and structured after-school physical activity sessions based on the Health Belief Model (HBM) and Transtheoretical Model (TTM). Implementation and evaluation plans were created, emphasizing real-time monitoring and adaptations. Strategies to enhance parental and community support were developed to address participation barriers. Although not tested in this study, these plans laid a robust foundation for fostering sustainable behavior change and improving physical activity among adolescents in resource-constrained settings.
Conclusion:
The Nyakaza-Move-for-Health intervention demonstrates a promising framework for promoting adolescent physical activity and addressing Non-Communicable Diseases in a culturally relevant manner. The systematic approach, grounded in the intervention mapping protocol, ensured a robust and replicable intervention design. Future research should focus on long-term follow-up, integrating objective physical activity measures, and expanding the program to include nutrition education. Addressing identified barriers, such as parental involvement, is crucial for enhancing the intervention’s effectiveness and sustainability.
Keywords
Introduction
Physical Activity (PA) is any bodily movement produced by the skeletal muscles that result in energy expenditure and is categorized into sports, exercise, recreation, occupation, and household activities. 1 PA has numerous health benefits, including improving physical fitness (PF), cardiometabolic health, bone health, mental health, cognitive outcomes and reduced adiposity. 2 Therefore, the World Health Organization (WHO) has recommended that children and adolescents participate in at least 60 min of moderate to vigorous physical activity (MVPA) daily to obtain these benefits. 3 However, 81% of adolescents aged 11 to 17 are insufficiently physically active globally, presenting a critical public health issue. 4 In South Africa, nearly 30% of adolescents fail to meet PA recommendations, increasing obesity and NCDs. 5
NCDs are chronic diseases which cannot be transferred from one person to another and are mainly caused by genetical, physiological, environmental and behavioral factors.6 -8 The main types of NCDs include cardiovascular diseases, cancers, respiratory diseases and diabetes, 8 and are reported to cause about 22% mortality in adolescent boys and 28% in adolescent girls in South Africa. 8 The modifiable behavioral risk factors of NCDs are alcohol and tobacco use, unhealthy diet, and physical inactivity. 8 Prolonged physical inactivity leads to metabolic risk factors of NCDs, which include raised blood pressure, hyperglycemia, hyperlipidemia and overweight and obesity. 9
Overweight is defined as Body Mass Index (BMI) of 25 and 29.9 kg/m² and obesity as BMI of 30 kg/m² or higher in adults. 10 Children and adolescents are considered overweight if their BMI-for-age is above the 85th percentile but below the 97th percentile, while obesity is defined as a BMI-for-age at or above the 97th percentile when using the age- and sex-specific percentile charts. 11 In 2016, South African adolescent boys (20%) were overweight and (9%) obese.12,13 Of adolescent girls, 32% were overweight and 13% obese.12,13 The high prevalence of overweight and obesity among South African adolescents is an indication that a significant number of adolescents are susceptible to NCDs. Being overweight and obese increases the risk of developing NCDs, such as cardiovascular diseases, type 2 diabetes, certain cancers, and musculoskeletal disorders later in life. 12 Recent global statistics highlight the alarming prevalence of NCDs in younger populations; approximately 390 million children aged 5 to 19 were estimated to be overweight worldwide in 2022, with a significant portion at risk of developing NCDs. 14 Childhood obesity not only impacts immediate health but also predisposes individuals to long-term health complications, highlighting the urgency of preventive measures and early intervention strategies.15 -17
The United Nations held a high-level meeting on NCDs in 2011 and reported that about 50% of NCD risk factors are modifiable, including physical inactivity, obesity, and unhealthy diet. 18 The United Nations encouraged all their member regions and states to develop global, regional and national strategies to prevent and manage NCDs,18,19 emphasizing modifiable risk factors. However, NCDs have since disproportionately risen in low-income and lower-middle-income countries. 20 The lower-middle-income countries are reported to lack the scale necessary to accelerate progress toward target 3.4 of the sustainable development goals (SDG) “to reduce premature mortality from NCDs by one-third.” 21 Therefore, interventions to curb NCDs’ behavioral and biological risk factors in low and middle-income countries should be urgently prioritized.22,23
Implementing global initiatives on PA and conducting community-wide public education campaigns were recommended by the World Health Organization as effective strategies to curb NCD risk factors. 23 Consequently, PA intervention studies24 -26 have been conducted on South African children and adolescents. These studies have provided significant insights into the positive impacts of PA interventions among children and adolescents. However, while these studies included some implementation and evaluation procedures, they did not offer detailed descriptions of the step-by-step intervention development process, trial implementation, and evaluation plans. Providing more comprehensive information in these areas could further enhance the ability of others to replicate and build upon these successful programs at the community level.
Enhancing behavioral intervention’s effectiveness requires systematic, participatory, theory, and evidence-based development.27,28 However, detailed descriptions of the intervention development process are seldom published, impeding transparency and progress in the field. 28 This study addresses this gap by describing the application of the IM protocol in the stepwise development of the Nyakaza Move-for-Health intervention program for adolescents. The IM protocol involves a thorough assessment of the health problem, its behavioral and environmental causes, and the determinants of these conditions.29 -31 Since individual, behavioral and environmental factors significantly influence the problem and strategy, it is crucial to determine these factors before designing an intervention program. 32 The IM protocol considers multiple theoretical perspectives to find answers to the problem. 31 The IM protocol has been widely utilized in developing health promotion interventions,33 -35 demonstrating its robustness and adaptability in diverse contexts.
Based on the broad context described above, this study outlines the steps in designing the Nyakaza-Move-for-Health intervention program, highlighting the results of the formative research conducted under specific Intervention Mapping (IM) steps. The main aim is to provide a detailed account of how these steps led to the development of the Nyakaza Move-for-Health intervention program.
Methods
Study Design
This study utilized a systematic Intervention Mapping (IM) protocol to develop the Nyakaza Move-for-Health intervention program. IM protocol ensures that all stakeholders are involved in the intervention development process; it applies well-established theoretical frameworks and an ecological approach. 34 The IM protocol consists of 6 steps: (1) Needs assessment, (2) developing a logical model of the problem, (3) Formulating program outcomes and objectives, (4) Program design and production, (5) Generating implementation plan, and (6) Generating intervention evaluation plan.29,31,32
Step 1: Needs assessment
a) A systematic literature review was conducted to gather epidemiological data on NCDs among adolescents in sub-Saharan Africa. The focus was on risk factors such as physical inactivity and sedentary behavior (SB). Additionally, PA interventions targeting adolescents were reviewed to identify effective strategies. A systematic literature review was conducted using the search terms “non-communicable diseases,” “NCDs,” “adolescents,” “youth,” “sub-Saharan Africa,” “physical inactivity,” “sedentary behavior,” and “physical activity interventions.” Databases searched included SA-Epublications, EBSCOhost, PubMed, Scopus Web of Science, Google Scholar and African Journals Online (AJOL). The review criteria were based on the type of study, which offered quantitative or qualitative data on the prevalence and risk factors for NCDs. and on success of PA interventions in sub-Saharan African adolescents. The systematic review employed PICO (Population Intervention, Comparison and Outcome) format to formulate the research questions and objectives. 36 Studies included in the literature search were from 2010 to 2023. The search conducted at first revealed (N = 127) articles. Papers included for review were selected based on whether they provided information on the epidemiology of NCDs among adolescents in sub-Saharan Africa or the efficacy of PA interventions. Research articles that concerned other regions or populations of the world except sub-Saharan were removed. This was done to avoid mixing the results among the 91 articles identified after excluding duplicates. Applying inclusion criteria and excluding the irrelevant ones. Forty-two (n = 42) remained for further analysis. Data extraction included searching for new or significant observations relevant to NCD risk factors and possible PA interventions.
b) Focus Group Discussions (FGD) were conducted with (n = 48) adolescent learners to explore personal, interpersonal, and environmental determinants influencing their PA behaviors. These participants were recruited from a preliminary investigation of the Nyakaza project titled Physical Activity Patterns and Levels among Adolescents. 37 Participant’s recruitment ensured diversity in age, gender, and socio-economic background and were grouped into sessions of 6 to 8 adolescents. Six adolescent learners were randomly chosen from each of the 8 participating schools to ensure representativeness and diversity. This resulted in a total of 48 adolescents. These students were already part of the larger Nyakaza-Move for Health study cohort.37,38 Participants who engaged in the FGD duly consented. Ethical guidelines were followed to ensure informed participation and protection of their rights throughout the research process. Inclusion criteria included adolescents aged 13 to 17 years attending schools within the target geographical area of the study and willingness to participate in group discussions on PA behaviors. Adolescent learners not part of the preliminary investigation37,38 were excluded, and those who could not meet the age requirement of 13 to 17 years old. Each focus group lasted between 45 and 60 min. All FGD were audio recorded. The research assistants took notes. Data collected in the focus group was thematically analyzed. Audio recordings were transcribed verbatim by the primary researcher and imported into NVivo software. This was done for systematic coding and analysis. Themes were identified through an iterative process. Coding and interpretation were essential. This allowed for extracting key factors influencing adolescent PA behaviors.
c) Another part of the needs assessment involved one-on-one meetings with potential stakeholders and adopters of the intervention program. In order to draft, implement and evaluate an adolescent health and wellness program, initial meetings were conducted with principals from schools as well as senior officers representing the eThekwini Metropolitan Municipal Parks and Recreation Unit, KwaZulu Natal (KZN) Department of Health and community groups. A SEW was thereafter scheduled with these identified stakeholder organizations and groups. The workshop was attended by 26 representatives from selected schools, communities and partner organizations, including officials from the EThekwini Metropolitan Municipality Sports and Recreation Department (n = 4), community healthy lifestyle facilitators (n = 8), life orientation teachers (n = 4), sports science and physical education lecturers (n = 5)and university postgraduate students in leisure/exercise sciences (n = 5). Six agenda items were discussed during the workshop, that is: (i) Presentation of the World Health Organization’s recommended areas for action; presentation of what has been done so far by Sport and Recreation South Africa regarding PA; (iii) Problems in communities; (iv) Development of a shared vision and goals for the proposed program; (v) Identification of enabling and prohibiting factors for effective implementation of the intervention in the selected communities, and (vi) Identification of possible intervention components. Audio recordings from one-on-one meetings and SEW were transcribed verbatim by the primary researcher and research assistants and imported into NVivo software for systematic coding and analysis. Themes were identified through an iterative process of coding and interpretation, allowing for extracting key information on a shared vision and goal of the program, enabling and prohibiting factors for effective program implementation, and the intervention components.
Step 2: Logic model of the problem
Step 2 of the IM involved a systematic approach that was aligned with IM reporting guidelines. The results of the literature review, FGD and stakeholder workshop (Step 1) were used to identify critical determinants of physical inactivity among adolescents. These determinants were categorized into personal, interpersonal and environmental determinants. A visual diagram was created to represent the logic model, using boxes and arrows to illustrate the relationships between components.
Step 3: Logic model of change
In step 3 of the IM, a logic model of change (LOC) which specifies change objectives, performance objectives and behavioral outcomes related to personal determinants of PA behavior was established. Change objectives are desired changes that need to occur to achieve a change in the PA behavior of adolescents. The performance objectives imply specific actions or behaviors individuals must perform to achieve behavioral outcomes. Behavioral outcomes are the ultimate behavior that the intervention aims to achieve. A graphic visual presentation of the LOC is presented in this study.
Step 4: Program design and production
In Step 4 of IM, the Program Design and Production step, the theoretical frameworks, the Transtheoretical Model (TTM) 39 and the Health Belief Model (HBM) 40 were used to guide the design of intervention components aimed at improving PA levels, changing PA behavior and improving adolescents’ PF levels. The TTM helps identify the participant’s stages of behavior change (pre-contemplation, contemplation, preparation, action, and maintenance), ensuring a targeted intervention is designed. The HBM emphasizes an individual’s perceived susceptibility and severity to lifestyle diseases, as well as perceived benefits and barriers, which then informs the type of intervention that can move adolescents from being sedentary and physically inactive to being sufficiently and regularly physically active and maintaining the behavior. Methods such as conscious-raising messages, persuasive communication techniques, and empowerment strategies were identified and integrated into the Nyakaza intervention program components (Social Marketing Campaign and the After-school PA program). The Nyakaza intervention program was described using the Template for Intervention Description and Replication (TIDieR) framework. 41 This framework documents each intervention component, including materials used, procedures followed, and how the intervention was delivered. 41 This level of detail enhances transparency in reporting, supports replication of the intervention in other settings, and allows for a thorough assessment of fidelity to the original design. 41
Step 5: Intervention implementation plan
In step 5, an intervention implementation plan was meticulously developed through a systematic approach that integrated outcomes from the preceding steps. The outcomes and performance objectives of the program were articulated, providing a clear roadmap of what the program aimed to achieve and the benchmarks for success. Then, the matrices of change objectives, detailing and aligning the desired changes with the program’s goals, were constructed. The performance objectives, methods, and their practical application, as well as the implementers of the intervention and the implementation timelines, are described in the implementation plan.
Step 6: Intervention evaluation plan
In Step 6 of the intervention development process, an evaluation plan was devised to assess the effectiveness of the Nyakaza intervention program in increasing PA levels and improving PA behavior and PF among adolescents. The evaluation employed a mixed-methods approach, integrating quantitative and qualitative methodologies to capture the intervention’s impact comprehensively. Quantitative methods included pre- and post-intervention assessments of BMI, Waist-to-Hip Ratio and predicted VO2 max using a multistage fitness test. Self-efficacy and physical activity levels were measured pre-and post-intervention using the scale for physical activity self-efficacy and self-reported PAQ-A. Qualitative methods involved focus group discussions, facilitator feedback, PA logs and observation notes. These methods offer in-depth insights into participants’ experiences, perceived benefits, challenges and overall engagement with intervention.
Results
Key Literature Review Findings
Epidemiological findings
The literature review on epidemiological factors revealed that, in sub-Saharan Africa, NCDs are the leading cause of morbidity and mortality, adding to the burden of communicable diseases already prevalent in the region.42 -44 Without rapid interventions, NCDs are projected to become the leading cause of mortality in sub-Saharan African countries by 2030, particularly impacting younger populations. 9 Risk factors for NCDs among adolescents in the region include tobacco and alcohol use, unhealthy diets, sedentary lifestyles (SL), reduced PA, and increasing rates of overweight and obesity.45 -49 South Africa, like many other countries in sub-Saharan Africa, faces a high burden of NCDs, with cardiovascular diseases being a significant contributor to mortality. 47 NCDs have surpassed injuries and communicable diseases as a major cause of disability-adjusted life years (DALYs) among adolescents, highlighting the urgent need for intervention programs targeting this population group.16,50 The prevalence of overweight and obesity among adolescents is rising, posing significant health risks and increasing the likelihood of developing cardiovascular diseases and metabolic syndrome.51 -53 SB and physical inactivity further exacerbate the risk of NCDs, emphasizing the importance of promoting healthy lifestyles and regular PA among adolescents. 53 The epidemiological data highlights the critical need for comprehensive interventions to address NCD risk factors, particularly among adolescents, to mitigate the growing burden of NCDs in sub-Saharan Africa.
Physical activity interventions
The literature review on PA interventions highlights various strategies with mixed results regarding their effectiveness. Community-based interventions, particularly group-based formats, have shown potential in addressing barriers like lack of social support and promoting health-related behavior change, yet they often suffer from high attrition rates and methodological weaknesses.25,54,55 Cognitive behavioral approaches, which incorporate goal setting, self-monitoring, and addressing barriers, have successfully increased PA among socially disadvantaged groups. 56 Mediated approaches, utilizing media such as print, telephone, and web-based technology, are effective when theoretically grounded and tailored to individuals, with social marketing emerging as a promising strategy for promoting health-related behavior change. 57 School-based interventions, including physical education curriculum changes and comprehensive approaches, have shown efficacy in enhancing PA and fitness among children, though time constraints within the school setting limit their overall impact.58 -60 Despite the potential of after-school programs to reduce sedentary time and improve PA levels, these interventions often experience high dropout rates and limited effectiveness, mainly due to insufficient community involvement in their development and implementation.25,61 Furthermore, many interventions have focused on immediate behavioral change without adequately assessing participants’ readiness to change, resulting in poor adherence and sustainability. The literature review’s results directed this research’s focus toward understanding behavior change mechanisms in group-based interventions and ensuring community engagement to enhance intervention effectiveness and sustainability.
Key Findings From the Focus Group Discussions
FGD were conducted with 48 adolescent learners to explore personal, interpersonal, and environmental determinants influencing their PA behaviors. These participants, aged 13 to 17, were recruited through schools to ensure diversity in age, gender, and socio-economic background. The groups comprised of 50% boys and 50% girls, with each session including 6 to 8 adolescents. Equal numbers of participants were selected from 8 participating schools.
Personal determinants
Adolescents’ perceptions of the benefits of PA, which include physical, physiological, and psychological advantages, serve as motivational factors for active engagement. Conversely, inactive peers expressed intentions to participate in PA but mentioned that they lacked sufficient information about PA benefits, leading to SL. Additionally, adolescents cited their perceived susceptibility to lifestyle diseases as a motivating factor for PA involvement. However, a lack of knowledge about the dangers of physical inactivity was identified as a significant barrier attributed to limited participation in PA. PA self-efficacy emerged as crucial, with many adolescents expressing feelings of incompetence and anticipating exercise difficulty and discomfort.
Interpersonal determinants
The FGD revealed that there are interpersonal determinants of PA. The influential role of parental and peer support in PA participation was highlighted as a significant interpersonal determinant. Adolescents believed increased parental support and permission would enhance their PA engagement, while a lack of peer support and negative comments were discouraging factors impacting motivation and self-esteem.
Environmental determinants
The FGD also identified some environmental determinants of PA and physical inactivity. The availability and variety of PA programs near communities were cited as factors that enable or prevent participation in PA. Adolescents generally preferred non-competitive, fun, and social activities such as dance, music, and aerobics. However, gender differences were noted: males showed a preference for competitive sports and body-building, while females expressed concerns about exercise’s potential effects on appearance. The factors identified in the FGD are essential in designing and producing a tailored and culturally relevant PA intervention program.
Key Findings From Stakeholder Engagement
Twenty-six representatives from selected schools, communities, and partner organizations attended the workshop. The demographics of the participants included officials from the eThekwini Metropolitan Municipality Sports and Recreation Department (n = 4); community healthy lifestyle facilitators (n = 8); life orientation teachers (n = 4); sport science and physical education lecturers (n = 5); and university postgraduate students in the field of leisure and exercise sciences (n = 5). The stakeholder engagement meetings and workshop produced several outcomes that informed the development and implementation of the intervention program. Stakeholders agreed to create active adolescents, provide a structured program within their communities, and form partnerships between affected organizations and communities. Factors identified to facilitate the successful implementation of a community-based PA intervention program included forming working partnerships between stakeholders, institutional monitoring, and support throughout the implementation phase. Capacity development training for facilitators was identified as crucial for the program’s success. Perceived constraints included a lack of parental support and permission for children to attend the program and a lack of program monitoring and support. Consequently, strategies to involve parents and other community role players were deemed necessary, and all partners committed to supporting and actively participating in the intervention’s development, implementation, and evaluation.
Logic Model of the Problem
The logic model in Figure 1 visually represents these determinants of physical inactivity and their interconnections, providing a holistic understanding of the issue. The logical model of the problem identified personal, interpersonal, and environmental determinants of physical inactivity. The personal determinants included lack of knowledge of PA benefits, lack of knowledge about dangers of SL and physical inactivity and low self-efficacy. Interpersonal factors were lack of parental and peer support. Lastly, the identified environmental determinants were lack of structured PA programs and unsafe neighbohoods.

Problem logic model.
Logic Model of Change
In the IM step 3, a LOC Table 1, was developed for the current study, it is already published 59 to illustrate the LOC and provide a set of matrices to achieve the desired behavior. The LOC shows the personal determinants of behavior change identified in step 1 of the IM, the change objectives (what the intervention intends to change), the performance objectives (how will we know if the intervention produced the desired change) and lastly, the behavioral outcomes (what will be the short term or long term outcome of the intervention). The first change objective is to improve adolescents’ knowledge of PA and its benefits. The performance objective is for participants to be able to identify the importance and benefits of PA. The expected behavioral outcome is increased knowledge, risk perception, attitudes, and beliefs about PA and its benefits. The second change objective is to raise awareness of the dangers of a SL and physical inactivity. The performance objective is for participants to identify their risks of physical inactivity. The expected behavioral outcome is an increased awareness of the risks of physical inactivity. The third change objective is to improve PA self-efficacy among adolescents. The performance objective is for participants to feel confident about their capabilities to engage in PA. The expected behavioral outcome is enhanced confidence in engaging in PA. The last and final change objective is to provide opportunities for structured PA. The performance objective is for participants to participate in structured PA over an extended period. The expected behavioral outcome is increased participation in PA, improved PF, and enhanced PA behavior.
Logic Model of Change.
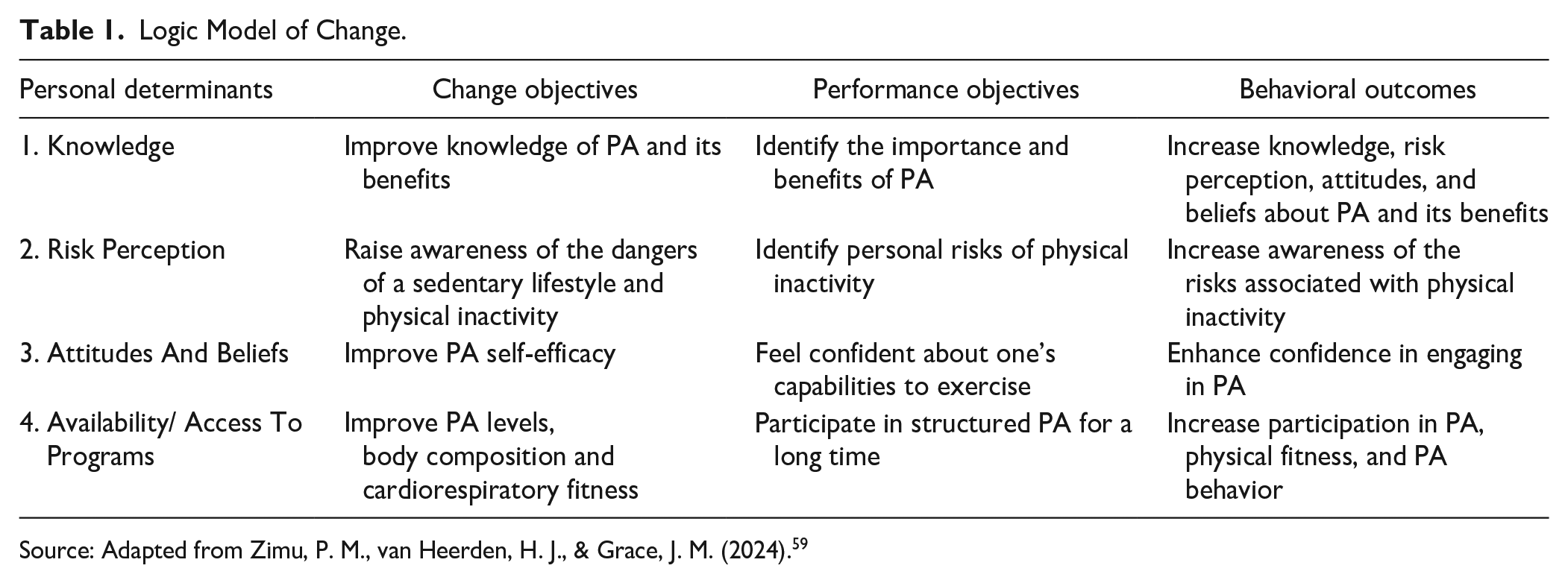
Source: Adapted from Zimu, P. M., van Heerden, H. J., & Grace, J. M. (2024). 59
Program Design and Production
The intervention program design and production phase translated change objectives into practical methods and applications grounded in relevant theories Table 1. The integration of the TTM and the HBM informed the intervention design by addressing the psychological and behavioral determinants of PA among adolescents. Specific methods such as social marketing campaign, persuasive communication, and empowerment techniques were identified for their potential to influence adolescent physical PA behavior. Social marketing campaigns (Component 1) utilized conscious-raising messages to improve knowledge and awareness. Persuasive communication techniques were utilized to enhance PA self-efficacy by providing positive reinforcement and tailored messaging to boost confidence in one’s ability to engage in regular PA (eg, providing praise and encouragement to participants for completing challenging exercises during the after-school PA program). Additionally, empowerment techniques were implemented to foster a sense of autonomy and control over PA behaviors, empowering adolescents to make informed choices and take ownership of their health and well-being (eg, encouraging adolescents to set personal goals related to PA participation during the after-school program, allowing them to take ownership of their health behaviors). These methods were practically applied through the delivery of the Nyakaza social marketing campaign (Component 1) and the structured after-school PA program (Component 2), ensuring alignment with theoretical frameworks and addressing the specific determinants of PA identified in earlier phases of the IM process. The Nyakaza intervention program is fully described in Table 2 using the TIDieR framework.
Nyakaza Intervention Program Described With the TIDieR.

Intervention Implementation and Evaluation Plan
Intervention Implementation Plan
The intervention implementation and evaluation plan in Table 3 guides the implementation and evaluation of the Nyakaza program. The intervention unfolds over 12 weeks. Commencing with a social marketing campaign, the campaign starts 6 weeks prior. This serves as a critical precursor. It aims to build awareness and readiness for behavior change among adolescents. Disseminating infographics, posters, exercise book covers and social media posts highlighting PA’s benefits and the risks of a sedentary lifestyle. The after-school PA component is implemented during weeks 1 to 12 following the campaign. A variety of moderate to vigorous physical activities (MVPA) are included. These include fitness dance classes and fitness challenges. Participants are encouraged to engage for at least 60 min per day. Facilitators provide positive feedback and set achievable goals to enhance self-efficacy, creating opportunities for mastery experiences that foster participants’ confidence in their ability to engage in PA.
Implementation and Evaluation Plan.

Source: Adapted from Zimu, P. M., van Heerden, H. J., & Grace, J. M. (2024). 59
Intervention Evaluation Plan
The evaluation of the Nyakaza Program will be conducted through both process and outcome assessments, allowing for a comprehensive understanding of the intervention’s effectiveness. Process evaluation will involve monitoring participation through attendance logs and collecting feedback via surveys to assess participants’ engagement and perceptions of the campaign’s relevance and impact. Outcome evaluation qualitative methods will included measuring changes in knowledge and awareness using pre- and post-intervention FGD surveys at the start (Week 0) and end (Week 12) of the intervention. Outcome evaluation quantitative methods will include measuring self-efficacy assessed through validated scales administered at Weeks 6 and 12, capturing participants’ confidence in their ability to engage in regular PA. Additionally, fitness assessments, such as anthropometry measures and cardiorespiratory fitness, occur at the program’s beginning (Week 1) and at its conclusion (Week 12). Anthropometry measures include BMI, Waist and Hip Measurements, Waist-to-Hip ratio, and cardiorespiratory fitness using field-based VO2 max (multistage fitness test). PA level is evaluated using a standardized questionnaire PAQ-A. These quantitative and qualitative measurements aim to assess the intervention’s efficacy and effectiveness in improving knowledge of PA and its benefits, raising awareness of the dangers of a sedentary lifestyle and physical inactivity, improving PA self-efficacy and improving daily PA levels, decreasing body mass index and improving the VO2 max (cardiorespiratory fitness) of the adolescents.
Discussion
This research has provided a detailed development process for the Nyakaza intervention program. Following an IM protocol, a Nyakaza-move-for-health intervention program premised on the TTM and HBM models was developed. This section explores the critical findings of this research, compares them with existing literature, and highlights the intervention’s strengths and limitations. Additionally, it provides insights into the practical implications for future PA promotion programs and suggests directions for further research.
The literature review highlighted the urgent need for intervention programs targeting adolescents to mitigate the growing burden of NCDs in sub-Saharan Africa. The projected increase in NCD-related mortality by 2030, particularly among younger populations, highlights the critical importance of early intervention. 62 Similar studies have emphasized the role of early-life interventions in preventing NCDs by promoting healthy behaviors during adolescence.16,50 The rising prevalence of overweight and obesity among adolescents in South Africa poses significant health risks, aligning with global trends observed in other developing regions.12,13,53
The literature review on PA interventions showed mixed results, reflecting the complexity of influencing health-related behavior change. Community-based interventions have potential but often face challenges such as high attrition rates and methodological weaknesses.63,64 Cognitive-behavioral approaches, incorporating goal setting and self-monitoring, have been successful among socially disadvantaged groups.65,66 Mediated media and technology approaches have shown promise, particularly when tailored to individual needs and grounded in theoretical frameworks.67,68 While effective in enhancing PA and fitness, school-based interventions are limited by time constraints and require more comprehensive approaches.58,69,70 These findings suggest that a combination of strategies, including community and school-based interventions, may be necessary for sustained behavior change.
The FGD offered a wealth of information regarding the personal, interpersonal, and environmental factors influencing PA among adolescents. Knowledge of the benefits of PA, perceived risk of contracting lifestyle diseases and self-efficiency were considered major antecedents of PA behavior. Consistent with Bandura’s Social Cognitive Theory, self-efficacy was identified as another predictor of PA engagement.71,72 The interpersonal factors, parental and peer support were also noted, as have other studies on social support in increasing PA among adolescents.73 -76 Factors within the environment include the accessibility and available choices of PA programs, which could act as enablers or barriers to the targeted populations’ participation. There were also differences in preferences for PA activities by gender, as observed at the societal level.77 -81
The stakeholder engagement meetings revealed the need to develop partnerships enabling schools, communities, and other organizations to implement PA interventions effectively. As seen in comparable community-based PA interventions, capacity development training for facilitators acknowledges the necessity for involving parents and other stakeholders in the community. The stakeholders’ endorsement to support the development, implementation and evaluation of the Nyakaza intervention program is evidence of the paradigm shift that involves the community in the planning, execution and monitoring processes necessary for successful and sustainable health promotion programs.
Development of a Behavior Change Physical Activity Intervention
The intervention design phase started with the creation of the LOC. The LOC shows personal determinants of PA among adolescents, the change objectives, performance objectives, and behavioral outcomes which guides the intervention development. The first change objective of the LOC is to improve adolescents’ knowledge of PA and its benefits, with the performance objective being identifying the importance and benefits of PA. The TTM and the HBM guided the development of the intervention methods and practical application strategies, offering sound concepts for addressing the psychological and behavioral factors contributing to PA. The TTM uses stages of change to integrate processes and principles of change from different theories of intervention. The 5 stages of change include pre-contemplation, contemplation, preparation, action, and maintenance. 39 The TTM postulates that behavior change revolves within a series of stages informed by cognitive and motivational constructs, decisional balance and self-efficacy. 82 Decisional balance is the comparison of the advantages and disadvantages of a certain behavior while self-efficacy, taken from the social cognitive theory, 71 explains motivation, planning and perseverance abilities of an individual depending on a belief that he or she can make a change. 83 The HBM, on the other hand, posits that if a person is aware of the threat that is posed by harmful behavior, the adoption of a mechanism to mitigate the potential damage will be adopted. 40 The 4 HBM constructs are perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. 40 Therefore, aligned with the first change objective (to improve adolescents’ knowledge about the importance and benefits of PA), a social marketing campaign was designed to move adolescents across the stage of change continuum of the TTM. The campaign delivers messages through visually appealing infographics and posters emphasizing the susceptibility and severity of adolescents to lifestyle diseases, and highlighting the benefits of engaging in PA. 39 Previous research has found that social marketing strategies significantly increased PA levels among adolescents by enhancing their knowledge and positive attitudes toward PA.84 -88 Targeted messages in the Nyakaza social marketing campaign educate participants on the health dangers of inactivity, such as obesity, diabetes, and cardiovascular diseases. This is achieved through school book covers featuring compelling statistics and personal stories. Previous research has shown that educational campaigns focusing on the risks of inactivity can effectively change adolescents’ perceptions and motivate them to increase their PA levels.87 -89 Therefore, the social marketing intervention component is likely to improve knowledge of PA and its benefits and raise awareness about the dangers of sedentary lifestyle and physical inactivity.
In framing this research, the study adopted a human movement conceptual framework. 90 The human movement framework postulate that PA is a behavior that drives human movement. The framework suggest that PA behavior should always be studied in the context of other constructs of human movement such as sedentary behavior. 90 Sedentary behavior can be divided into 2 domains, discretionary and non-discretionary domains. The nondiscretionary sedentary domain as “activities such as sitting during work or school hours or while in a car driving, and discretionary sedentary activities as “sitting while watching television, reading, playing video games, or computer use during nonwork or school-related hours.” 90 The human movement conceptual framework further posit that PA behavior provides physical and physiological outcomes such as energy expenditure, improved PF (body composition, cardiorespiratory fitness, muscular fitness and flexibility) and ultimately improved quality of life. Therefore, participation in any of the 4 domains of PA (leisure-time PA, occupation, transportation and household activities) may provide positive effect in the health and quality of life of those participating. On the other hand, the framework posit that physically inactive and sedentary individuals expend less energy and are likely to have poor PF and ultimately a compromised health. 90 Based on this framework, the personal, interpersonal and environmental determinants identified in the early IM stages, an after-school PA program component was designed and tailored for the action stage of the TTM. The after-school PA program focus at facilitating regular participation in PA. This component enables adolescents to be actively involved in PA on a consistent basis, in turn improving their physical health and encouraging desirable behavioral patterns regarding PA. This approach enhances their PF and fosters positive PA behaviors. The structured sessions help build self-efficacy by providing the support and resources needed to maintain regular PA and overcome perceived barriers. To improve PA self-efficacy, persuasive communication and empowerment techniques were employed. To achieve this, facilitators provided consistent positive feedback during PA sessions and created opportunities for participants to experience mastery by gradually increasing the difficulty of physical activities. Self-efficacy is a critical factor in behavior change, and interventions that improve self-efficacy lead to sustained PA engagement.71,91
Intervention Implementation
The Nyakaza program is strategically structured to enhance PA participation among inactive adolescents through a comprehensive approach that integrates the HBM and the TTM. The implementation plan spans 18 weeks, with the initial 6 weeks (6 weeks) dedicated to a social marketing campaign designed to build awareness and motivation among participants. This timing is crucial, as research indicates that early engagement through informative campaigns can effectively prime adolescents for behavior change.91 -94 By commencing the social marketing campaign before the after-school PA intervention, the program aims to address cognitive and motivational barriers, creating a solid foundation for subsequent participation in structured activities.
The integration of the social marketing campaign with the after-school PA program is a key feature of the intervention’s design. The campaign focuses on improving knowledge about the benefits of PA and raising awareness of the dangers associated with a sedentary lifestyle. This is critical, as studies have shown that enhanced knowledge significantly predicts increased PA levels among adolescents. 95 Following this preparatory phase, the structured PA intervention will include diverse activities aimed at promoting consistent engagement, which is essential for behavior maintenance according to TTM. 39
Intervention Evaluation
Outcome measures have been carefully selected to evaluate the effectiveness of the intervention. Knowledge and awareness will be assessed through pre- and post-intervention surveys (FGD), which are grounded in validated instruments that have demonstrated reliability in previous studies.33,35,76 Self-efficacy, a critical predictor of behavior change, will be measured using established self-efficacy scales, 96 which have been shown to possess strong psychometric properties. 97 Additionally, PA levels and fitness outcomes will be monitored through fitness assessments, activity logs and self-reported questionnaires, ensuring a comprehensive evaluation of the intervention’s impact on both behavioral and health-related outcomes.
The duration of the after-school PA component, spanning 12 weeks, aligns with recommendations from the literature suggesting that sustained engagement over time is necessary for significant behavior change and health improvements. 98 This timeframe allows for adequate exposure to the intervention components and the opportunity for participants to internalize the benefits of PA and develop new habits. The combination of a robust implementation plan and thorough evaluation framework positions the Nyakaza program to effectively address the complex factors influencing adolescent PA.
Recommendations for Future Research
Future research should focus on conducting long-term follow-up studies as they are essential in assessing the sustainability of the intervention. Objective measures of PA, such as accelerometers or motion sensors, should be integrated to provide more accurate and reliable data on participant’s activity levels. While the Nyakaza intervention included multiple components to influence the behavior of adolescents, it is recommended that nutrition education be included to further enhance the impact on adolescent health outcomes by addressing dietary behavior alongside PA. The intervention should be implemented and assessed for effectiveness in other regions and diverse populations to test its generalizability and replicability. While this intervention emphasize the need for parental involvement and support, future studies using the Nyakaza intervention should seek to involve other adolescents and broader community engagement to address some identified barriers and enhance the intervention’s effectiveness. Incorporating technology-based intervention materials such as electronic infographics and mobile health applications could improve participant engagement and provide additional support for behavior change.
Limitations
The Nyakaza intervention program’s limitations include the reliance on self-reported data for PA outcomes, which may introduce bias and affect the accuracy of the results. The intervention’s duration (12 weeks) is short and may limit the ability to assess long-term sustainability and effectiveness.
Conclusion
The findings of this study underscore the importance of addressing the complex interplay of personal, interpersonal, and environmental factors influencing adolescent PA behaviors through tailored and culturally relevant intervention programs. The Nyakaza intervention holds promise in promoting PA and mitigating the burden of NCDs among adolescents in sub-Saharan Africa. This research has complemented the body of knowledge on health promotion by presenting a step-by-step process for the development of a PA intervention program (Nyakaza-Move-for-Health). The Nyakaza-Move-for-Health intervention program which has 2 interrelated components (healthy lifestyle social marketing campaign and a structured after-school PA program was systematically developed following an IM protocol, an approach that is structured and grounded in theory and evidence. The application of IM protocol has allowed researchers to collect first-hand data to diagnose the health problem that needs to be addressed and to develop theoretically sound methods and practical applications to address the health problem. This research has also generated implementation and evaluation plans that can be used for future implementation and evaluation of the Nyakaza-Move-for-Health intervention program.
Footnotes
Acknowledgements
The authors acknowledge Mrs. Catherine Connolly for her assistance with statistical analysis. We are grateful to the KZN Department of Education and School Principals for their cooperation. The authors appreciate the eThekwini Metropolitan Municipality for granting permission to use their facilities. Financial support from the National Research Foundation (NRF) and the University of KwaZulu-Natal, College of Health Sciences, is gratefully acknowledged.
Acronyms
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the National Research Foundation (NRF) and the University of KwaZulu-Natal, College of Health Sciences.
Ethical Approval and Informed Consent Statements
The research protocol was approved by the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal, Protocol reference number HSS/1407/017D. Permission to conduct the research at the schools was obtained from the KZN Department of Basic Education, and from the principals of all the schools involved. Participants, parents and guardians provided informed assent and consent.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to [reasons such as privacy or confidentiality] but are available from the corresponding author on reasonable request.