
Abstract
Objective:
There has been a trend toward hospital systems and insurers acquiring privately owned physician practices and subsequently converting them into vertically integrated practices. The purpose of this study is to observe whether this change in ownership of a medical practice influences adherence to clinical guidelines for the management of type 1 and type 2 diabetes.
Methods:
This is an observational study using pooled cross-sectional data (2014-2016 and 2018-2019) from the National Ambulatory Medical Care Survey, a nationally representative probability sample of US office-based physician visits. A total of 7499 chronic routine follow ups and preventative care visits to non-integrated (solo and group physician practices) and integrated practices were analyzed to see whether guideline concordant care was provided. Measures included 7 services that are recommended annually for individuals with type 1 and type 2 diabetes (HbA1c, lipid panel, serum creatinine, depression screening, influenza immunization, foot examination, and BMI).
Results:
Compared to non-integrated physician practices, vertically integrated practices had higher rates of hemoglobin A1C testing (odds ratio 1.58 [95% CI 1.07-2.33], P < .05), serum creatine testing (odds ratio 1.53 [95% CI 1.02-2.29], P < .05), foot examinations (odds ratio 2.03 [95% CI 0.98-4.22], P = .058), and BMI measuring (odds ratio 1.54 [95% CI 0.99-2.39], P = .054). There was no significant difference in lipid panel testing, depression screenings, or influenza immunizations.
Conclusions:
Our results show that integrated medical practices have a higher adherence to diabetes practice guidelines than non-integrated practices. However, rates of services provided regardless of ownership were low.
Introduction
Diabetes mellitus is a chronic, metabolic condition characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. 1 According to the CDC, diabetes mellitus affects more than 37 million US adults and is the eighth leading cause of death. 2 About 10% of US adults are living with diabetes—0.5% with type 1 diabetes and 8.5% with type 2 diabetes. 3 Diabetes can lead to multiple microvascular conditions such as diabetic nephropathy, neuropathy, and retinopathy. Additionally, it can lead to macrovascular complications, such as coronary artery disease, peripheral arterial disease, and stroke. 4 It is the number one cause of renal failure, lower limb amputations, and adult blindness, and diagnoses have more than doubled in the past 20 years. 2 Given the severe complications associated with the disease, it’s imperative for physicians to provide the appropriate preventive services for individuals with diabetes in order to achieve better outcomes for their patients.
The American Diabetes Association (ADA) and American Association of Clinical Endocrinology (AACE) set forth annual guidelines on measures that can help prevent or delay the onset of more severe complications of diabetes mellitus. Unfortunately, physician adherence to these guidelines is poor,5,6 with certain services, such as hemoglobin A1C testing, offered more frequently than others, such as foot exams.7,8
Current trends show that an increasing number of physician and physician group owned practices are being acquired by large hospital systems and other corporate entities (eg, health insurers and private equity firms), a term coined vertical integration. 9 The Physician Advocacy Institute estimated 44 300 physician practices were acquired by hospitals from 2012 to 2018, a 124% increase. 10 The COVID-19 pandemic accelerated this trend, and an additional 36 200 acquisitions were made from 2019 to 2021, a 36% increase. By the start of 2022, more than 50% of physician practices were owned by a hospital or a corporate entity. 11 Health insurers have also increased their stake in physician owned practice; 1 example is the $69 billion CVS-Aetna merger in 2018. Similarly, UnitedHealth Group acquired DaVita outpatient dialysis centers in 2019, increasing its network of affiliated physicians to more than 45 000. 9
In theory, hospitals and health insurers should have the financial and logistical capabilities to better adhere to diabetes guidelines. This could be accomplished through the use of care management processes (CMPs)—“specific activities performed in a clinical practice with the goal of improving coordinated, effective clinical care.” These can include checklists, targeted reminders, or after-visits follow-up by a non-clinician. 12 Physician practices acquired by hospitals have been found to implement the use of more CMPs, 13 and CMPs have been shown to improve diabetes care measures, 12 suggesting vertical integration could have a positive effect on diabetes management.
While few studies show physicians’ adherence to diabetes guidelines, existing studies show the relationship between vertical integration and diabetes care. However, the diabetes care present in these studies is often limited to a few screening and monitoring measures, or are not nationally representative. For example, it was shown that hospital-based physician groups had higher rates of retinal eye exams, hemoglobin A1C and LDL-C testing for Medicare patients compared to smaller independent groups. 14 Similarly, multispecialty clinics affiliated with the Council of Accountable Physician Practices (most of whom were part of a hospital or health plan) had higher rates of fundoscopy exams, hemoglobin A1C, and lipid testing compared to non-CAPP affiliated practices. 15 Another study used a set of 5 treatment goals (hemoglobin A1C <8%, blood pressure <140/90, LDL-C <100 mg/dL, daily aspirin use, and documented tobacco-free status) to assess diabetes care in 100 clinics that were acquired by health systems in Minnesota from 2007 to 2013. Five years post acquisition, the acquired clinics scored higher in diabetes care metrics than if they had never been acquired. 16 In contrast, Medicare beneficiaries treated at hospital-owned groups had lower HbA1c screening rates compared to physician owned groups. 17
There is a gap in literature on the effect vertical integration has on physicians’ adherence to diabetes guidelines. The purpose of this study is to examine a broad scope of services offered at annual visits for type 1 and type 2 diabetics, as recommended by the ADA and AACE, and whether ownership of the practice influences the likelihood of these services being offered.
Methods
Data Source
We used pooled data from the 2014 to 2016 and 2018 to 2019 National Ambulatory Medical Care Survey (NAMCS), which was the most recent data available at the time of analysis (2017 NAMCS data is not currently available to the public). NAMCS is a nationally representative probability sample of physician office visits in the US conducted annually by the National Center for Health Statistics. 18 The study used de-identified public use data and is exempt from institutional review board approval.
Measures
We measured the rates of services offered during all annual preventative care visits and routine chronic care follow-up visits by patients identified as having type 1 or type 2 diabetes (N = 7499). The services examined include hemoglobin A1C testing, serum creatinine testing, lipid panel testing, foot examinations, BMI measuring, depression screenings, and influenza vaccinations, as recommended by the ADA and AACE.19,20 NAMCS has ownership of a practice divided into 3 categories: physician or physician group; medical/academic health center, other hospital; and insurance company, health plan, HMO, other health care corporation. Due to sample size limitations, we combined the latter 2 categories into 1 “integrated practice” category to ensure there was an adequate number of sampled visits to produce stable estimates. We then compared the rates of services offered during these visits for individuals with diabetes at integrated practices to non-integrated practices (solo/group physician practices).
Patient Characteristics
Patient characteristics that were controlled for in the analysis included age, sex, race (White, Black, or other race), ethnicity (Hispanic or non-Hispanic), total number of chronic conditions, and type of insurance (private, Medicaid, Medicare, other insurance such as worker’s compensation, or uninsured). Table 1 offers a summary of visit characteristics to integrated and non-integrated health practices included in the sample.
Summary of Visit Characteristics to Integrated and Non-Integrated Health Practices.

Characteristics of patients seen during the visit.
Physician Specialty
Physician specialty was coded as family medicine, internal medicine, or all other specialties.
Statistical Analysis
Office-based visits for individuals with type 1 or type 2 diabetes in which a HbA1c, serum creatinine, foot exam, depression screen, lipid panel, influenza immunization, and BMI measuring were offered from 2014 to 2016 and 2018 to 2019 in the USA were estimated. Multivariable logistic regression analyses were conducted to assess whether the odds of having a service offered varied by practice ownership, controlling for patient age, patient sex, patient race/ethnicity, type of insurance coverage, total number of chronic conditions, and physician specialty. Analyses were performed using the survey procedures of Stata 15.1 to allow results to be nationally representative and to account for the complex sampling strategy of NAMCS.
Results
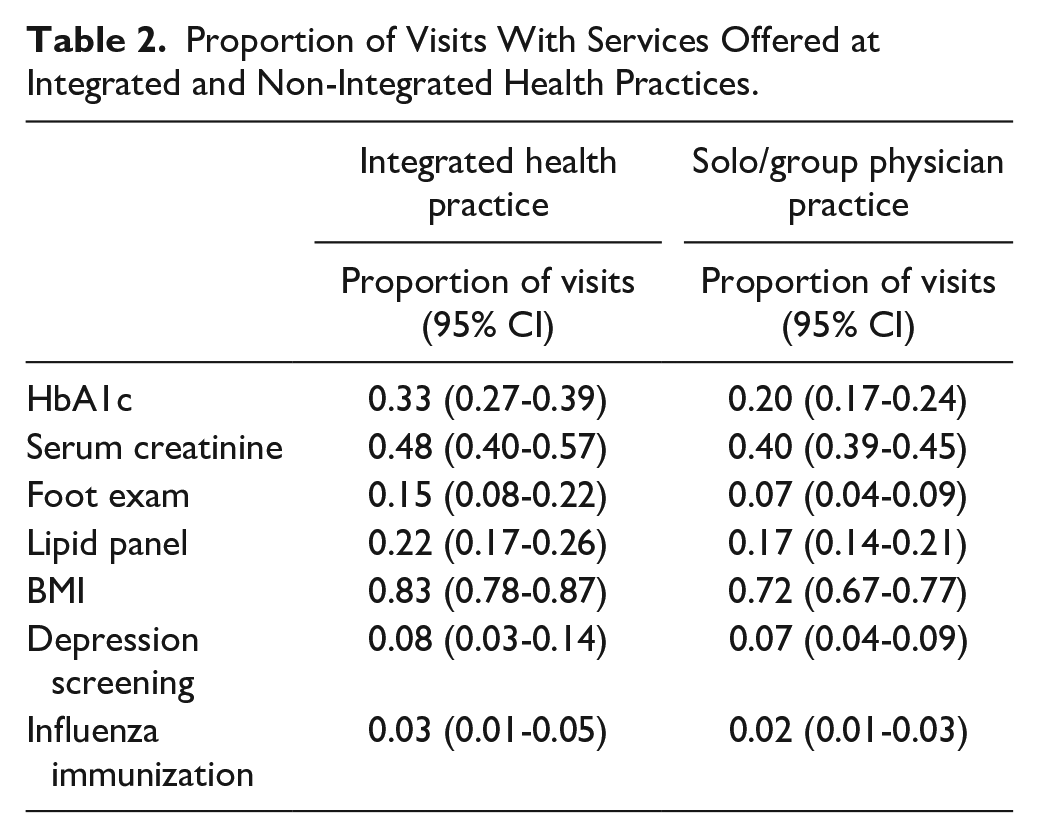
Table 2 shows the proportion of visits with services offered at integrated and non-integrated health practices. Services that showed the greatest difference in the probability of being offered depending on integration status were hemoglobin A1C testing, serum creatinine testing, foot examinations, and BMI measuring. Hemoglobin A1C testing was offered at 33% (95% CI 27%-39%) of visits at integrated practices versus 20% (95% CI 17%-24%) at non-integrated practices. Serum creatinine testing was offered at 48% (95% CI 40%-57%) of visits at integrated practices versus 40% (95% CI 39%-45%) at non-integrated. Foot examinations were offered at 15% (95% CI 8%-22%) of visits at integrated practices versus 7% (95% CI 4%-9%) at non-integrated. BMI measures were performed at 83% (95% CI 78%-87%) of visits at integrated practices versus 72% (95% CI 67%-77%) at non-integrated. The lowest of all services offered regardless of ownership were depression screenings and influenzas immunizations. Depression screenings were offered at 8% (95% CI 3%-14%) of visits at integrated practices versus 7% (95% CI 4%-9%) at non-integrated. Influenza immunizations were offered at 3% (95% CI 1%-5%) of visits at integrated practices versus 2% (95% CI 4%-9%) at non-integrated. Table 3 shows weighted odds ratios of services provided at chronic routine follow up and preventative care visits. Compared to non-integrated physician practices, integrated practices had higher rates of hemoglobin A1C testing (odd ratio 1.58 [95% CI 1.07-2.33], P < .05), serum creatinine testing (odds ratio 1.53 [95% CI 1.02-2.29], P < .05), foot examinations (odds ratio 2.03 [95% CI 0.98-4.22], P = .058), and BMI measuring (odds ratio 1.54 [95% CI 0.99-2.39], P = .054). There was no significant difference in lipid panel testing, depression screenings, or influenza immunizations.
Proportion of Visits With Services Offered at Integrated and Non-Integrated Health Practices.
Adjusted Odds of Services Offered at Integrated Versus Non-Integrated Health Practices.

Discussion
There were clinically meaningful findings in 4 out of the 7 metrics we used to determine adherence to diabetes guidelines, all of which had greater odds of being offered in integrated practices compared to non-integrated practices. This suggests vertically integrated practices may be better suited to treat type 1 and type 2 diabetes. Similar to the studies listed earlier,14 -16 certain services had higher rates of being offered at integrated practices compared to those that are non-integrated. Our data also showed that regardless of ownership, laboratory tests such as hemoglobin A1C and serum creatinine were offered more frequently than others, such as foot exams, similar to what was found in previous studies.7,8 This could be due to the relative ease of completing said services. Ordering a lab test may seem to be simpler than completing a comprehensive foot examination, and in a setting where time constraints are frequent, the latter could be ignored. Across all practices and regardless of ownership, BMI measuring was offered the most. Height and weight, the 2 components of BMI, are usually taken at the beginning of every office visit regardless of the chief complaint and could reflect its high use of implementation. The rates of most other services offered at both integrated and non-integrated practices were surprisingly low. Some, such as depression screenings were offered in under 10% of visits, and flu immunizations in under 5% of visits. This could be because these 2 services may appear not as integral to diabetes management compared to other forms, such as laboratory testing, and may be overlooked. Additionally, influenza immunizations are offered seasonally and may not even be available at time of office visit, potentially contributing to their low service rates. Most surprising was the rate of hemoglobin A1C testing—considered to be the gold standard for diabetes monitoring—was only offered during 33% and 20% of visits at integrated and non-integrated practices, respectively. This seemingly poor adherence to treatment guidelines is concerning, but fortunately, existing studies show how adherence can be improved. A cross-sectional, survey-based study of 400 physicians at the University of Florida found that access to relevant guidelines at the point of care (EMR), improved focus on guidelines during training, and more transparency about physician commercial affiliation would help increase adherence to guidelines. 21 Additionally, programed reminders in an EMR and the implementation of a checklist that monitored the completion of diabetes measures increased provider adherence to diabetes guidelines in primary care settings.22,23
Limitations
It’s important to note that not all the guidelines that are recommended by the ADA and AACE were evaluated. Behavioral factors (assessing physical activity), technology use (reviewing insulin pump settings), pharmacotherapy (discussing medication plan), and social life assessments (identifying social supports) were absent from the NAMCS data set and were excluded. The NAMCS dataset does not include health status or urban/rural status as variables, thus cannot be included as a covariate. Additionally, NAMCS does not include indicators of HMO or managed care in the data, preventing further breakdown of insurance status. Referral data is not present in NAMCS, exuding dilated eye exams, which are required to be completed by an optometrist or ophthalmologist. Urinary albumin to creatinine ratio, a common diabetes monitoring laboratory test, was absent from the NAMCS data set as well. It’s also a possibility that patients refused or had contradictions to the influenza vaccine, or received the vaccine elsewhere (such as a pharmacy) as potential reasons for its low rate.
Conclusion
Visits to integrated practices offered services more frequently for managing type 1 and type 2 diabetes compared to visits to non-integrated practices, which is important to consider if ever seeking treatment for diabetes. However, rates of services are low regardless of ownership, suggesting adherence to diabetes guidelines is poor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.