
Abstract
Background:
Anxiety and depression often exacerbate multimorbidity conditions, leading to increased disability rates among affected individuals.
Objective:
The study aimed to assess the mental health status of individuals with multimorbidity belonging to the marginalized population of Karachi, Pakistan. Specifically, the prevalence of anxiety and depression was investigated.
Methods:
A multicenter cross-sectional study was conducted between July 2022 and June 2023 in 10 primary healthcare clinics located in 4 peri-urban areas of Karachi. A total of 9331 participants were included in the study. The Patient Health Questionnaire 4 (PHQ-4), Generalized Anxiety Disorder 7 (GAD-7), and Patient Health Questionnaire 9 (PHQ-9) were used to assess symptoms of anxiety and depression. The data collected were analyzed using the statistical analysis system (SAS) version 9.4.
Results:
Among the study participants, 2894 (31%) were men and 5534 (59.3%) were women. The prevalence of moderate to severe anxiety was 31% among men and 59.3% among women. The age group between 41 and 60 years exhibited the highest rates of moderate to severe anxiety, 19.3% as evaluated by GAD-7 and 34.6% by PHQ-9. The Pathan ethnic group had the highest prevalence of anxiety (11%) and depression (28.3%) in the neighborhoods. Unemployed participants showed moderate to severe anxiety in 21.3% of the cases and moderate to severe depression in 25.5% of the cases.
Conclusion:
The study revealed a significant cooccurrence of anxiety and depression among individuals with multimorbidity in the marginalized population of Karachi, Pakistan. Furthermore, the presence of anxiety symptoms in multimorbidity patients with depression indicates a more unfavorable health state. It is essential to explore the implementation of screening measures and therapeutic interventions for comorbid anxiety and depression in this population to improve clinical outcomes.
What is Already Known About this Subject?
Chronic diseases play an imperative role in causing distress and depression.
What are the New Findings?
The need for on-site therapy for this significant issue is highlighted. Some clinic visitors showed suicidal thoughts and self-harm, which are commonly ignored in general care. Diabetes and chronic pain problems, including back or joint pain, require a better mental health screening due to their potential influence on quality of life.
How Could These Results Change the Focus of Research or Clinical Practice?
The year-long study of a large slum population provided useful information. The results show that sociodemographic characteristics are linked to many chronic diseases in primary care. These variables also increase the risk of mental health problems, lowering the quality of life in these groups. Longitudinal investigations are needed to show the causation between chronic illnesses and mental health issues. These results emphasize the necessity of incorporating mental health screening and assistance into primary care to promote the well-being of marginalized groups.
Introduction
The concept of mental health goes beyond the absence of mental diseases, encompassing various mental illnesses, psychosocial disorders, and other mental states characterized by suffering, impaired functioning, or an increased risk of self-harm. 1 Although people diagnosed with mental health problems are more likely to experience diminished mental well-being, it is essential to recognize that this correlation is not universally applicable or inherently deterministic. 2
From 1990 to 2019, mental problems increased in 31 European countries. However, self-harm in both genders has dropped by more than 20%. Economically developed nations have fewer mental health problems than low- and middle-income countries. 3 In India, 197.3 million people had mental illness in 2017, 45.7 million had depressive disorders, and 44.9 million anxiety disorders. 4 The rates of mental illness in adults in Bangladesh ranged from 6.5% to 31.0%, while the rates in children ranged from 13.4% to 22.9%. 5 Pakistani anxiety and depression rates range from 22% to 60%. 6
Depression and anxiety are becoming more common, and chronically ill people are especially susceptible.7 -10 One in 4 residents of advanced countries has multimorbidity.11 -13 In impoverished countries such as Bangladesh, 53.8% of older people have multimorbidity. 14 Multimorbidity affects 22% of Indians and 4.9% of Pakistanis aged 18 years and older.15,16 Multimorbidity ranges from 4.9% to 67% among countries.17,18 Multiple chronic diseases harm a person’s health and increase financial pressure on families, the healthcare system, and society. 19 A 2013 poll found that 28% of Americans had multimorbidity, which represented 66% of healthcare care spending. 20 Research has found a strong link between socioeconomic position and multimorbidity, regardless of education, 21 income, 22 occupation, 23 or regional disadvantage. 24 Healthcare providers typically struggle to treat multimorbidity, anxiety, and depression. Diabetes, hypertension, stroke, asthma, arthritis, and osteoporosis increase the risk of disability when combined with anxiety and depression. 25
The Rationale of the Study
Mental diseases are common, but underdiagnosed in low- and middle-income countries, making treatment difficult. As a result, it becomes critical to prioritize screening for mental disorders in people with multimorbidity to mitigate the negative impact of comorbidities and improve adherence to multimorbidity therapy. The rationale for conducting this study lies in the urgency to address this knowledge gap and provide essential information on mental health issues among marginalized populations with multimorbidity. By doing so, our aim is to contribute to the development of effective strategies to address mental health challenges in these vulnerable communities.
Methodology
Study design and duration: A cross-sectional study was carried out in collaboration with the SINA Health Education and Welfare Trust (SINA), which included 10 clinics located in the peri-urban regions of Karachi, Pakistan. The study spanned from July 2022 to June 2023. The recruitment of patients and the overall study design are visually represented in Figure 1.

Patients’ screening at study site.
Study population: A total of 10 low socioeconomic slum settlements are spread across 4 towns in Karachi, Pakistan. This research was conducted in the slums of Karachi, a metropolis known for its extensive urban development and its status as the nation’s largest city. These slum regions include Korangi Town, Landhi Town, Baldia Town, and a clinic near the Nazimabad industrial area. These areas are marked by a significant population density, 26 limited access to essential amenities, and challenging living conditions. Individuals within this group frequently face marginalization and confront various socio-economic barriers.
Study site: Significantly, the research was conducted in the SINA premises, a primary healthcare institution offering heavily subsidized health services to the community. 27 This approach ensured that participants received essential healthcare services from certified healthcare professionals. Incorporation of health facilities within selected peri-urban areas reflects a deliberate effort to address the health needs of these marginalized groups.
Inclusion and exclusion criteria: The study included individuals aged 18 and over who visited any of the 10 designated clinics within a 1-year period, from July 2022 to June 2023. These individuals were diagnosed with multimorbidity or chronic disease conditions and were selected for mental health screening. Patients who were referred due to acute conditions were excluded from the study. Additionally, individuals who faced challenges in understanding the survey questions or who declined to participate in the screening were also excluded from the study.
Data Collection Tool
Three distinct scales were used to analyze the results of mental health screening among patients with single or multiple chronic diseases, in conjunction with their sociodemographic status.
Demographic questionnaire: The structured questions designed by the researchers were used to collect information about the age, ethnicity, income, employment status, marital status, and disease status of the participants.
PHQ-4 questionnaire: The questions about mental health symptoms were adapted from the well-established 4-item Patient Health Questionnaire (PHQ-4), which is specifically designed to assess depression and anxiety. These questions aimed to understand the frequency of experiencing distress within the past week. 28
PHQ-9 questionnaire: The Patient Health Questionnaire-9 evaluated depression. Nine questions consistent with the DSM-IV depression criteria are included in this 4-point Likert scale questionnaire. Participants were asked to rate their depression symptoms during the last 2 weeks from 0 (not at all) to 3 (almost every day). A PHQ-9 score of 5 or higher indicated depression. The PHQ-9 is a thorough depression screening instrument that includes a passive suicidal ideation question. PHQ-9, a popular depression screening tool, has been associated with lower suicide risk screening rates in primary care. 29
GAD-7 Scale: Validation has been done on the GAD-7 scale. The initial scores on this scale range from 0 to 3. This survey measures 7 anxiety symptoms and their frequency in the 2 weeks before. For answers such as “not at all,” “a few days,” “more than half the days,” and “almost daily,” patients get scores of 0, 1, 2, and 3. 30
Sample Size
There was no boundary of sample size in this study, those who visited SINA trust in July 2022 to June 2023, were considered for screening. Approximately, a total of 9331 participants were included in the study who were visited SINA with some disease condition.
Data Collection Procedure
Patients at SINA-affiliated hospitals must undergo various procedures. Most importantly, the registration staff requested written permission from the patients after explaining the anonymity and privacy of the information. After sociodemographic verification, the electronic management record system records all new patient and follow-up data at reception. After that, the patient is sent to the vital signs station for height, weight, and vital signs. They are then issued a token number and must wait to visit a doctor or specialist for a medical and early mental health examination. A PHQ-4 scale is used for early anxiety and depression assessment. The ISO-certified SINA diagnostic laboratory conducts the clinical investigation after a physician’s consultation to determine comorbidity or multimorbidity. Figure 1 shows the patient registration at the study site. The patients are then referred to mental health counselors for confirmation of anxiety, depression, or both. After assessing the patient, mental health counselors send them to a psychologist for further therapy. Figure 2 shows the mental health screening process at the study site. The study analysis included all patients from July 2022 until June 2023.

Mental Health Screening at study site.
Statistical Analysis
Microsoft Excel and SAS 9.4 were used to analyze the data. The accuracy and consistency of the data was verified using a comprehensive validation procedure.
We selected 2 key outcome variables from the data: GAD-7 (confirmed anxiety) and PHQ-9 (recorded depression). A descriptive analysis using counts and proportions was used.
We used bivariate analysis to identify multivariate model predictors with P-values of 0.2 or less (20%). We used multinomial regression analysis after carefully selecting predictors for each dependent variable and taking into account the multilevel character of GAD-7 and PHQ-9. This study sought to determine the link between outcome variables and relevant predictor factors.
GAD-7 and PHQ-9 were condensed into 3 categories instead of 5: “mild to minimal,” “moderate to severe,” and “no confirmed anxiety.” This increased their importance. This change enabled more reliable findings and interpretations.
Results
Descriptive Statistics
Table 1 presents the results of the descriptive analysis related to the outcome variables. Of the total of 931 study participants, 2894 (31%) men and 5534 (59.3%) women exhibited moderate to severe levels of anxiety and moderate to severe depression, respectively. In particular, the age group between 41 and 60 years emerged as the most prevalent category for moderate to severe anxiety levels, with rates of 19.3% according to the GAD-7 assessment, and 34.6% according to the PHQ-9 assessment.
Descriptive Statistics of Predictor Variables with Respect to Outcome Variables (n = 9331, July 2022, June 2023).
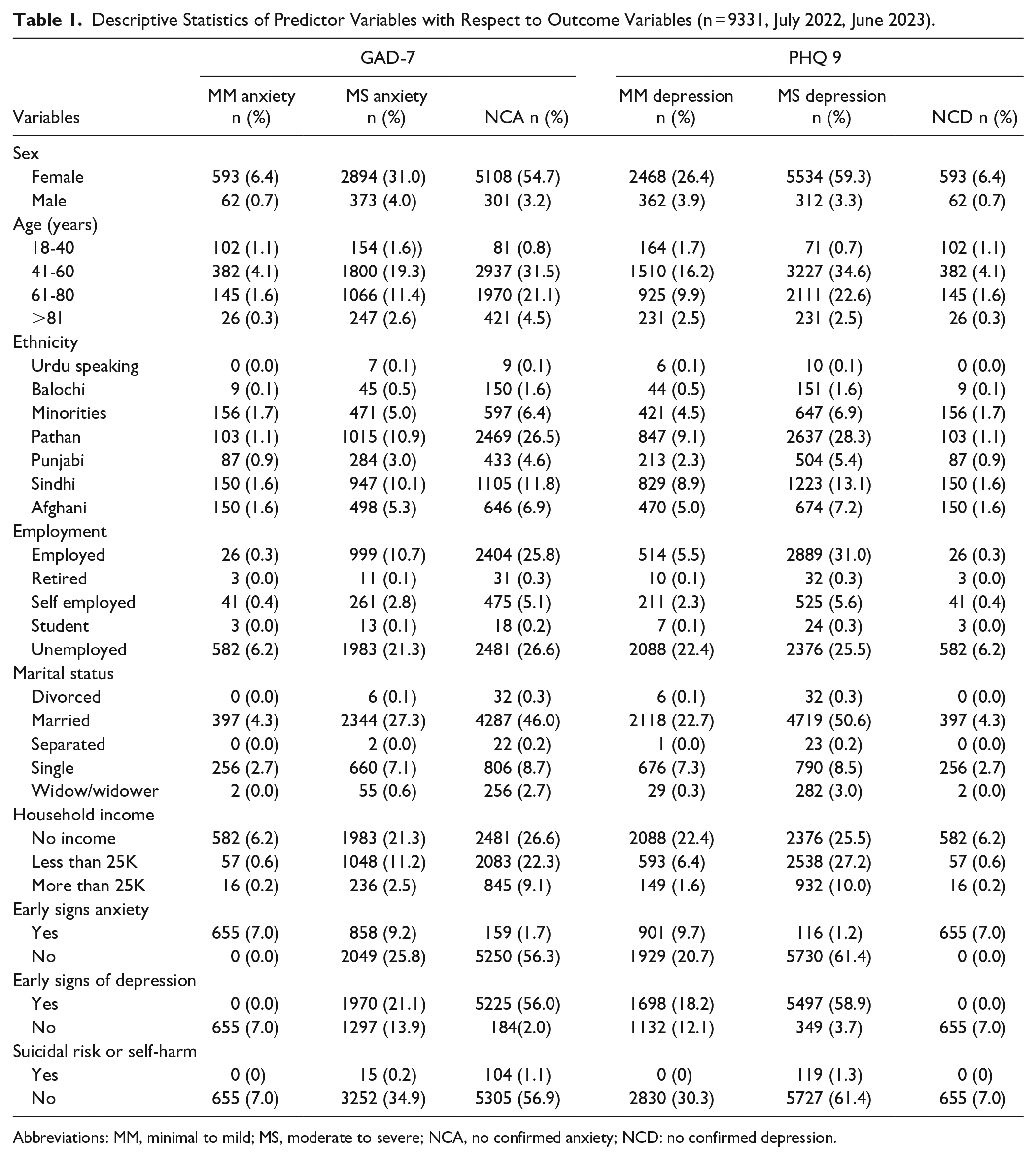
Abbreviations: MM, minimal to mild; MS, moderate to severe; NCA, no confirmed anxiety; NCD: no confirmed depression.
In terms of ethnic distribution within the slum areas, the Pathan community showed the highest prevalence of moderate to severe anxiety levels at 11%, while 28.3% experienced moderate to severe depression levels. The unemployed among the study participants exhibited moderate to severe anxiety rates of 21.3%, while moderate to severe depression rates stood at 25.5%.
Married study participants showed 27.3% with moderate to severe anxiety levels and 50.6% with moderate to severe depression levels. Furthermore, participants without household income revealed moderate to severe anxiety levels of 21.3% and moderate to severe depression levels of 25.5%. Notably, 47.7% of the participants were identified as eligible candidates for specialist counseling.
Within the study population, 9.2% showed moderate to severe levels of early signs of anxiety, while 9.7% exhibited mild to minimal symptoms of depression. Those participants who were assessed as part of the suicidal or self-harm group showed a moderate to severe level of depression in 1.3% of cases.
Table 2 represents the relationship between single morbidity with anxiety and depression. As per Table 2, patients with joint pain 382 (4.1%), diabetes 234 (2.5%), hypertension 162 (1.7%), skin-related problems 258 (2.8%), and anemia 456 (4.9%) show moderate to severe symptoms of anxiety and similar pattern also observed in case of depression. Similarly, Table 3 shows the relationship of multimorbidity with mental health well-being. Among the various comorbidities, “diabetes with back and body pain” emerged as the most prevalent condition, exhibiting an 8.6% moderate to severe level of anxiety and an 18.2% moderate to severe level of depression. These findings shed light on the complex interplay between mental health and physical conditions within the studied population.
Prevalence of Anxiety or Depression Among Patients with Single Morbidity (n = 9331, July 2022, June 2023).

Abbreviations: MM, minimal to mild; MS, moderate to severe; NCA, no confirmed anxiety; NCD: no confirmed depression.
Prevalence of Anxiety and Depression Among Patients With Multimorbidity.
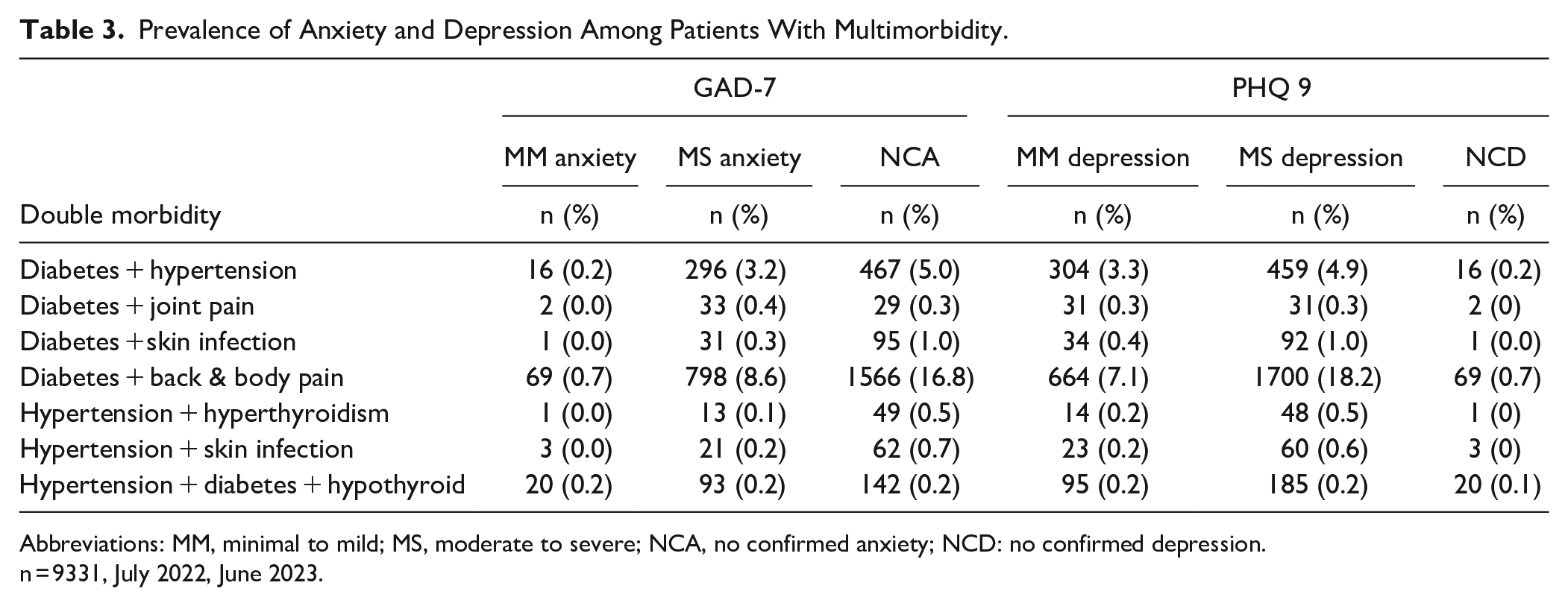
Abbreviations: MM, minimal to mild; MS, moderate to severe; NCA, no confirmed anxiety; NCD: no confirmed depression.
n = 9331, July 2022, June 2023.
Unadjusted Bivariate Analysis Between Outcome and Predictor Variables
Table 4 presents the unadjusted (bivariate) relationships between each dependent variable and the predictor variables. When considering the bivariate analysis for GAD-7 (levels of confirmed anxiety), all variables demonstrated a significant association (P < 0.20), with the exception of marital status. In the case of bivariate analysis with PHQ-9 (levels of documented depression), all independent variables exhibited significance (P < 0.20), except marital status, household income, and employment status. These findings provide insight into the initial correlations between the dependent and independent variables before accounting for other potential factors.
Bivariate (Unadjusted Analysis) Between Dependent and Independent Variables.

Abbreviation: ns, not significant.
Not included in the study.
Significant (P < .20).
Association of the “Level of Confirmed Anxiety (GAD-7)” with Study Predictors
Table 5 elucidates the multilevel association between sign of anxiety levels (GAD-7) and the predictors examined in the study. All study variables showed significant associations with the sign of anxiety levels (P < .05), with the exception of age, ethnicity, employment status, and household income.
Multinomial Adjusted Association Between GAD-7 (Level of Confirmed Anxiety) and Study Variables (n = 9331, July 2022, June 2023).

Abbreviations: CI: confidence interval; MM, minimal to mild; MS, moderate to severe; NCA, no confirmed anxiety; ns, not significance; Ref: reference category.
Level 1 of dependent variable (GAD-7).
Level 2 of dependent variable (GAD-7).
Reference category of dependent variable (GAD-7);
P < .05.
P < .001.
Gender: Females exhibited 2.87 times higher odds of developing a moderate to severe level of anxiety compared to males (P < .001; 95%CI 1.852-4.458).
Early signs of anxiety: Participants displaying early signs of anxiety had 2.86 times greater odds of developing a “moderate to severe” anxiety level compared to those without early signs of anxiety (P < .001; 95%CI 1.288-6.371).
Comorbidities: Individuals with the condition “diabetes and hypertension” had 0.54 times lower odds of developing a “moderate to severe” anxiety level compared to those without any comorbidities (P < .001; 95%CI: 0.303-0.983). Participants with the condition “diabetes with back and body pain” exhibited 1.60 times higher odds of developing a “minimal to mild” anxiety level compared to those without comorbidities (P < .001; 95%CI: 1.160-2.215). Those with hepatitis B or C had 0.48 times lower odds of developing “moderate to severe” anxiety compared to individuals without comorbidities (P < .001; 95%CI 0.260-0.898). Participants with “hypertension with skin infection” had 0.73 times lower odds of developing “minimal to mild” anxiety compared to those without comorbidities (P < .001; 95%CI: 0.576-0.926). Individuals with “women complications (vaginal infection/use of the birth control pill)” had 2.73 times higher odds of developing “moderate to severe” anxiety compared to those without comorbidities (P <.001; 95%CI: 1.910-3.916).
These associations highlight the nuanced interaction between various factors and confirmed anxiety levels within the studied population.
Association of “Levels of Confirmed Depression (PHQ-9)” with Study Predictors
Table 6 unveils the connection between multi-levels of documented depression (PHQ-9) and the predictors under study. All study variables demonstrated a significant association with documented depression levels (P < .05), except for age and ethnicity, which did not show a significant association (P > .05).
Multinomial Adjusted Association Between Level of Confirmed Depression (PHQ-9) and Study Variables (n = 9331, July 2022, June 2023).

Abbreviations: CI, confidence interval; MM, minimal to mild; MS, moderate to severe; NCA, no confirmed anxiety; ns, not significance; Ref, reference category.
Level 1 of dependent variable (GAD-7).
Level 2 of dependent variable (GAD-7).
Reference category of dependent variable (GAD-7);
P < .05.
P < .001.
Gender: Female participants had 1.66 times higher odds of developing a “moderate to severe” level of depression compared to males (P < .001; 95%CI: 1.095-2.505).
Early signs of depression: Participants who manifested early signs of depression had 1.78 times greater odds of developing a “moderate to severe” depression level compared to those without early signs of depression (P < .001; 95%CI: 0.779-4.073; MS vs NCA).
Comorbidities: Individuals with the condition “diabetes with hypertension” exhibited 2.74 times higher odds of developing a level of “moderate to severe” depression compared to those without any comorbidities (P < .001; 95%CI 1.329-5.666). Participants with “diabetes with back & body pain” demonstrated 6.07 times higher odds of developing moderate to severe depression compared to those without comorbidities (P < .001; 95%CI: 1.468-25.09). Those with hepatitis B or C had 5.52 times higher odds of developing a “moderate to severe” depression compared to individuals without comorbidities (P < .001; 95%CI: 1.677-18.20). Participants with hyperthyroidism hypertension exhibited 1.65 times higher odds of developing a “moderate to severe” depression compared to those without comorbidities (P < .001; 95%CI 1.032-2.655). Among female subjects, those with “women complications (vaginal infection/use of birth control pills)” had 2.79 times higher odds of developing a “moderate to severe” depression compared to those without comorbidities (P < .001; 95%CI: 2.281-3.422), while accounting for other factors.
Interaction and confounding effect: Comprehensive evaluations were conducted for potential interaction and confounding effects. However, such effects were not observed among the selected independent variables.
These results underline the intricate interplay between various factors and documented depression levels within the studied population.
Discussion
This study focused on individuals visiting primary healthcare clinics with multi-morbidity assessing their mental well-being through mental health screening. The findings revealed that approximately 35%-50% of women with multimorbidity exhibited moderate to severe levels of depression and anxiety.
In Karachi’s slums, women had more despair and anxiety than men. This trend matches a comprehensive UAE 2019 evaluation of various articles that found a higher prevalence of depression among Arab women. 31 A 2020 Chinese student study found that female students had higher levels of anxiety than male students throughout the year. 32 Medical disorders such as hormone abnormalities and reproduction difficulties may contribute to gender differences.33 -36
The link between unemployment, depression, and anxiety is notable. Unemployment and low income often aggravate anxiety and sadness. This financial burden was evident during the 2019 UK Greece financial crisis. 37 Bangladesh and Sweden’s young university graduates showed similar patterns in 2019. 38 Financial instability in slums increases sadness and anxiety, which may increase suicide rates.39,40
The research found that diabetes with back and body discomfort increased anxiety and despair. The worry of dependence on drugs and back and body pain contribute to this. Studies in the Netherlands and Spain in 2019 on diabetes, back pain, and mental illnesses complement this finding.41,42 Diabetes alone comorbidity also contributes to our research, as shown by a recent study in Karachi slums where diabetics demonstrate depression and suicidal thoughts. 39 A study evaluated 2 validated measures to diagnose depression in diabetes patients and found that Pakistan does not emphasize mental health, therefore, diabetes-related stress screening is scarce. We screen neglected areas in this investigation. Screening and clinical exams are vital, says one research. Recognize physician-related stress in patients during treatment. 43 In our study population, diabetes and hypertension are the third most important multi-morbidities for mental health. A 2018 Turkish study found that people with diabetes and hypertension often had sadness and anxiety. 44
Slum dwellers also have higher rates of mental health problems and multimorbidity with age. Social isolation and loneliness increase mental health risks. The effects of isolation, such as restricted social networks and feelings of abandonment, on anxiety and depressive symptoms were examined in older people 57 and older. 45 A 2014 Egyptian research 46 showed a link between depressed symptoms, cognitive impairment, preclinical neurodegeneration, and vascular abnormalities. Recent research on the physical health of adolescents in Karachi’s slums reported 16.7% metabolic syndrome (MetS) in 2 extensively inhabited slums. 47 MetS are cardio metabolic risk factors that increase the risk of type 2 diabetes and cardiovascular disease. 48 Some patients in our study had diabetes, hypertension, hypothyroidism, and moderate to severe depression and anxiety. Hypothyroidism was associated with sadness and anxiety. 49
Similarly to previous studies, 50 our study found that multimorbidity increases the risk of mental health issues. Multimorbidity in impoverished groups requires comprehensive mental health treatments due to the complex interaction of sociodemographic variables, comorbid disorders, financial hardships, and social isolation.
Conclusion
Deprived socioeconomic groups with multiple chronic diseases are more likely to have depression and anxiety symptoms. Individuals with anxiety, depression, and multimorbidity had worse health outcomes. Prospective longitudinal studies are needed to understand the temporal correlations in this area.
Clinicians should know that multi-morbid patients often have sadness and anxiety. Comorbid depression and anxiety can lead to lower health outcomes in several dimensions. Therefore, the detection and treatment of comorbid depression and anxiety in multi-morbid patients should be carefully considered due to their significant effect on unfavorable health outcomes. This emphasizes the need to treat mental health issues in multimorbidity to improve health.
Significance and Limitations of the Study
This study allowed researchers to examine the search for mental health help in the community. We had a 90% response rate, but only 7% of males aged 41 to 60 participated, and responders and non-respondents had different socioeconomic characteristics.
Cross-sectional data has drawbacks. Inquiring about recent help-seeking activities did not reveal the past and subsequent trends of the participants. Our research did not examine how personal beliefs and motives affected people’s help-seeking intentions and behaviors. To fully grasp this, qualitative research is needed. Our study used 3 measures to evaluate mental morbidity in the general sample, but did not diagnose particular diseases.
Implication of the Study
This study inspires further research, especially longitudinal or prospective cohort studies, to better understand the concerns of slum dwellers. To identify possible links and causes of chronic diseases and mental health disorders, longitudinal studies are necessary. Such research will illuminate the complex relationship between socioeconomic variables, chronic health conditions, and mental well-being, helping to create customized treatments to address these difficulties.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241258658 – Supplemental material for Prevalence of Mental Disorders Among Patients with Multimorbidity Visiting Primary Care Settings in Slums of Karachi, Pakistan
Supplemental material, sj-docx-1-jpc-10.1177_21501319241258658 for Prevalence of Mental Disorders Among Patients with Multimorbidity Visiting Primary Care Settings in Slums of Karachi, Pakistan by Hina Sharif, Sana Sharif Sheikh, Ambareen Main Thompson, Muzna Hashim, Tooba Seemi, Kashaf Zaidi and Sheikh Mohd Saleem in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors thank the SINA Health and Welfare Education Trust medical board for approving this research. Special thanks to Dr. Asif Imam for his important support of our project. The authors also thank Ms. Jannat Mustafa for her invaluable administrative assistance.
Contributors
HS conceptualized and designed the study and prepared the original draft. SSS greatly assisted with data analysis and interpretation. SMS completed the article and supervised the research. MH searched the literature, TS sorted the data, and AKT curated and polished the text, KZ shared the valuable insight of mental health and contribution in initial stage of manuscript. All authors carefully evaluated and approved the final work, allowing its publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations & participants’ consent
An ethical letter was obtained before data analysis, however data was gathered from July 2022 to June 2023. At the time of data collection, permission from the SINA Medical board was taken, and consent was obtained from the participants before the study was conducted. All patients with diabetes, hypertension, hypo/hyper thyroid, anemia, etc. who attend SINA are screened for mental health. The designated clinic routinely screened unidentified data. The study was approved by the SINA Medical Board and SINA Ethical Review Board (SINA-ERB) with approval number ERB0000021/08-23. Patients received written agreement, indicating their voluntary involvement. All research data will be anonymized before publication to safeguard participants’ identity.
Consent for Publication
All authors reviewed and consent for publication.
Data Availability
Data used to support the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.