
Abstract
Objectives:
This study aims to investigate the impact of gender and parental tasks on social participation, health-related quality of life (hrQoL), and mental health in persons with long COVID.
Methods:
A mixed-methods approach was followed including a cross-sectional web-based survey and semi-structured interviews. Multivariable linear regressions were used to quantify the effect of gender and parenting tasks on social participation, hrQoL, and mental health. Qualitative data from interviews with participants experiencing long COVID symptoms was analyzed using content analysis.
Results:
Data from 920 participants in the quantitative study and 25 participants in the qualitative study was analyzed. Parenting tasks were associated with increased impairments in family and domestic responsibilities in persons with long COVID compared to lower impairments in persons without long COVID (P = .02). The qualitative data indicate that coping with long COVID and pursuing parenting tasks limit participants’ ability to perform leisure activities and attend social gatherings. In long COVID, men had higher anxiety symptoms than women, and in those without long COVID, the opposite was observed (P < .001). In the qualitative study, participants expressed feelings of dejection and pessimism about their future private, occupational, and health situations. No differences between the genders could be observed.
Conclusions:
Long COVID is associated with impairments in family and domestic responsibilities in individuals who have parenting tasks. Among participants with long COVID, anxiety symptoms are higher in men than women.
Introduction
Approximately 7.5% of initially non-hospitalized SARS-CoV-2 (COVID-19) infected people continue to experience symptoms beyond the acute phase of their infection. 1 This condition which has been introduced as “post-acute COVID-19” or “Post-Acute Sequelae of SARS-CoV-2” is considerably more prevalent among initially hospitalized patients 2 : Among hospitalized COVID-19 survivors, 52.6% reported the persistence of at least 1 symptom. 3 Long COVID is associated with a variety of symptoms including cognitive impairment (“brain fog”), fatigue, muscle and joint pain, dizziness, and depression.4 -8 While typical definitions of long COVID require the persistence of symptoms over at least 4 weeks after acute COVID infection,9,10 many people with this condition describe lasting symptoms for months or even years. 11 There is a plethora of research stressing the immensely negative impact of long COVID symptoms on many aspects of social lives, 12 impairing quality of life, social participation, occupational perspective,13,14 and mental health. 15 However, a significant knowledge gap exists regarding how gender and gender roles, as well as caregiving responsibilities such as raising children, can moderate the quality of life, social participation, and mental well-being of individuals grappling with long COVID. This gap in understanding is especially pertinent since females have been found to have a higher risk of developing long COVID. 2
Research within the social sciences has consistently highlighted gender inequities in caregiving responsibilities, family roles, employment, career advancement, and income, all of which are deeply rooted in social norms and expectations.16 -18 The COVID-19 pandemic has resulted in pressure toward pre-existing established social roles, for example, by increasing care work for family members (eg, through home-schooling) during stay-at-home orders (lockdowns), absence from work and shift to home-office, etc. Furthermore, females have been particularly affected by dismissal from work during the COVID-19 pandemic compared to males.19,20 Some qualitative research has indicated that these factors contribute to lower quality of life and poorer mental health among female long COVID patients. 21 However, larger quantitative studies assessing these aspects, including the impact of childcare responsibilities, are lacking. In this study, we hypothesize that:
(1) Raising children is associated with greater social and health limitations including anxiety and depressive symptoms among participants with long COVID compared to those without long COVID, and
(2) social and health limitations including anxiety and depressive symptoms differ between long COVID status, gender, and persons with and without parenting task.
This comprehensive approach seeks to advance the understanding of the complex interplay between gender, caregiving, and the long-term consequences of COVID-19.
Methods
This study examines health and social effects of long COVID using a mixed methods convergent parallel design. A cross-sectional study was conducted as part of the quantitative aspect of the study. The qualitative study portion comprises 25 guided interviews. Analyses and discussion were conducted considering the mixed methods appraisal tool by Hong et al. 22 The study protocol 23 and a data protection plan were approved by the research ethics boards of Hannover Medical School (9948_BO_K_2021) and University Medical Center Göttingen (29/3/21). The study is registered in the German register for clinical trials (DRKS00026007).
Recruitment
Quantitative component
The survey was accessible through the project website (defeat-corona.de) starting from September 2021, and it remains open. To promote the survey, QR codes linking to the project website were displayed on posters and flyers in public locations such as libraries, town halls, and churches, as well as medical and research centers primarily in the German Federal State of Lower Saxony. Additionally, information material was sent to 400 randomly selected primary care, internal medicine, radiology, and occupational therapy practices in Lower Saxony. To reach participants with long COVID, patient advocacy groups focused on long COVID were asked to share the survey link on their social media channels.
The SoSci Survey online platform (SoSci Survey GmbH in Munich, Germany) was used to create and administer the survey, which was only available in the German language. To take part in the study, participants had to register with an e-mail address and a password. Multiple participation with an already registered e-mail address was not possible. Before filling out the questionnaire, participants were required to provide digital consent and confirm their age of at least 18 years. Data collection was conducted anonymously without any personally identifiable information. Pseudonyms were assigned to participants to enable follow-up surveys. Further information can be gathered from the study protocol. 23
Qualitative component
The recruitment process for the interviews involved several methods: (a) issuing a call for participation on the websites of the Department of General Practice at the University Medical Center Göttingen (UMG) and the Hannover Medical School (MHH); (b) posting on social media platforms, such as on the Instagram and Facebook accounts of the affiliated universities; (c) utilizing a snowball system, where participants recommended other individuals for participation; (d) distributing leaflets about the study in general practices in Lower Saxony and at the Public Health Authority of the City of Göttingen; and (e) sending emails requesting participant to n = 130 randomly selected individuals that previously completed the quantitative survey. 4 The recruitment activities took place in January and February 2022. Prior to the interviews, the recruited participants provided written consent to participate and allow publication of their data. The sample size was determined based on established guidelines for qualitative research, suggesting a minimum of 12 interviews.24 -26 A compensation of 40 Euros (approximately 40 USD) was provided to the participants for their involvement.
Eligibility Criteria
Quantitative component
Eligible participants needed (a) to be 18 years or older, (b) currently residing in Germany and (c) proficient in the German language. Duplicates were removed from the data set, and participants with missing information were excluded from the analyses. In addition, participants who were 68 years of age or older were excluded from the analyses because this study focuses on working-age people and the regular German retirement age is 67 years.
Qualitative component
Eligibility criteria included (a) having long COVID according to the definition of the German Institute of Public Health Robert Koch-Institute (persisting symptoms beyond the acute phase of SARS-CoV-2 infection of 4 weeks and not explained by any other diagnosis10,27), (b) a minimum age of 18 years, and (c) consent to participate in a videoconference or in-person interview group.
Quantitative Measures: Dependent Variables
IMET (Index for Measuring Participation Restriction)
The IMET consists of 9 items each representing a different dimension of social participation using a 11-point (0-10) Likert-scale. 28 The sum of all items ranging from 0 to 90 shows the overall social participation with a high internal reliability (Cronbach’s alpha .90). Higher values across all items and the sum score indicate greater self-reported impairments to social participation. The concept of social participation is based on the International Classification of Functioning, Disability and Health 29 from the WHO. The IMET was initially developed to collect data from people with different chronic diseases and used especially for rehabilitation research. This instrument was also already used by various authors to measure social impairment during the COVID-19 pandemic.30 -33
In this study the sum score of the IMET and the item “family and domestic responsibilities” were used as individual outcome measures.
EQ-5D-3L
The EQ-5D-3L consists of 2 main components: the EQ-5D descriptive system and the visual analogue scale (VAS).34,35 The descriptive system includes 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 levels: no problems, some problems, and extreme problems. Participants indicate their level of difficulty for each dimension using a 1-digit number. These digits are then combined into a 5-digit number representing the participant’s health state. These statements can be converted into EQ-5D index values, which reflect the health-related quality of life (hrQoL) on a scale from 0 (worst health) to 1 (best health). The VAS is used to collect data on self-rated health status. Participants select a value between 0 and 100, where 0 represents the “best imaginable health state,” and 100 represents the “worst imaginable health state.”
PHQ-9 (Patient Health Questionnaire-9)
The PHQ-9 is used to evaluate the severity of depressive symptoms. It consists of 9 items that assess various aspects of depression, including feelings of sadness, loss of interest, and disruptions in sleep patterns. 36 Each item is rated on a 4-point Likert-scale, ranging from 0 (not at all) to 3 (nearly every day). By summing the scores for each item, a total score between 0 and 27 can be obtained where higher scores indicate more severe depressive symptoms. When using a cutoff score of 10 a sensitivity of 88% and a specificity of 85% for diagnosing major depressive disorder was observed. 37 The PHQ-9 has demonstrated robust internal consistency, with Cronbach’s alpha coefficients ranging from .83 to .89 across different populations.36,38
GAD-7 (Generalized Anxiety Disorder-7)
The GAD-7 is a widely used self-report questionnaire designed to screen and assess the severity of generalized anxiety disorder symptoms. 39 It consists of 7 items that measure different aspects of anxiety, such as excessive worrying, restlessness, and difficulty controlling worry. Each item is rated on a 4-point Likert-scale, ranging from 0 (not at all) to 3 (nearly every day). The scores for each item are summed to obtain a total score, which can range from 0 to 21 where higher scores represent higher anxiety levels. Using a cutoff score of 10 a sensitivity of 74% and a specificity of 83% for diagnosing generalized anxiety disorder was observed. 40 The GAD-7 has demonstrated good internal consistency, with Cronbach’s alpha coefficients ranging from .89 to .92.39,41
Primary Exposure Variables
Parenting tasks
To assess if participants undertake parenting tasks, the 2 items, “Do you have children?” and “Do children under 18 live in your household?” were used. If participants answered both questions in the affirmative, they were categorized as having children’s educational tasks in the household.
Long COVID status
Participants were categorized into 1 of 2 groups according to their SARS-CoV-2 infection status and COVID-19 course: (a) Long COVID when they stated to have persistent or new symptoms 4 weeks.10,27 after a COVID-19 infection confirmed by an antibody test, PCR or positive rapid antigen test, and (b) NoCOVID when the participants were not known to be infected during or before the questionnaire was filled out.
Covariates
Covariates included gender (“To which gender identity do you most identify?”), age (in years), completed educational degree based on secondary school (low: no or low secondary school diploma; medium: intermediate secondary school diploma; high: college preparatory), marital status, employment status (full-time, part-time, and unemployed), pre-existing conditions grouped as cardiac conditions (hypertension, heart failure, coronary heart disease, or cardiac arrhythmia), and autoimmune diseases (colitis ulcerous, chronic hepatitis, psoriasis, various allergies, neurodermitis, Graves’ diseases and Hashimoto’s thyroiditis, rheumatoid arthritis, or rheumatic diseases).
Development of the Interview Guideline
The interview guideline was developed through a workshop involving 6 researchers at the Department of General Practice on October 29, 2021 (Supplemental File 1). The interview guideline consisted of 26 open-ended questions and a section of closed questions to gather sociodemographic information. To gather genuine insights, researchers did not provide participants with the used guideline before the interviews.
Data Collection Qualitative Component
The interviews took place from January to May 2022. Out of the 25 interviews, 21 were conducted using Zoom video conferencing software (Zoom Video Communications, Inc., San Jose, CA, USA). This method was chosen to accommodate participants with mobility limitations due to their health conditions, allowing them to participate from the comfort of their homes. Four interviews were conducted in person at the Department of General Practice in Göttingen and the Hannover Medical School. This decision aimed to gain deeper situational understanding and capture non-verbal communication, which can be limited in a digital setting. 42 During most of the interviews, only the participants and the researchers were present at the location where the data were collected. In some Zoom interviews, an artist was present as a silent observer to provide graphic interpretations of the participants’ statements. 43 One researcher conducted the interviews (SR). The online interviews and the face-to-face interviews were captured using a digital audio recording device. Additionally, the researcher made note of significant content during the interviews.
Data Analyses
Quantitative component: Statistical analysis
Participant characteristics are presented as number of observation and proportions for categorical variables or mean and standard deviations for continuous variables, stratified after long COVID status. To quantify the association of educational tasks of children in the household between participants with and without long COVID on social participation hrQoL and mental health linear regression models were performed. The IMET score (social participation), EQ-5D-3L index values (hrQoL), VAS scores (hrQoL), GAD-7 scores (anxiety symptoms), and PHQ-9 scores (depressive symptoms) were used as dependent variables. As independent variables long COVID status and educational tasks of children in the household were included with an interaction between the 2 variables. Additionally, the regression models were adjusted for gender, age, school education, marriage status, and comorbidities (cardiac condition and autoimmune disease). An interaction term between gender and long COVID status was included as literature suggest a possible differences of severity of COVID symptoms between the genders.44,45 Regression coefficients were reported with 95% confidence intervals and corresponding P-values. P-values <.05 were considered as statistically significant. As goodness of fit measure of the linear regression models R2 was reported.
Qualitative component
First, audio recordings were transcribed using a content-semantic transcription method.46,47 Then, a team of 2 researchers trained in social science (TS and SR), along with 3 study assistants (including GK), conducted a qualitative content analysis.48,49 To ensure quality, the research team used a consensus-based approach: they independently performed analysis steps and then discussed their findings to reach agreement.
The research team developed a category system, employing a combination of deductive and inductive strategies. The deductively derived main categories were based on the interview guideline. During the initial coding phase, top categories and subcategories were inductively derived from the data and linked in an axial manner. Once the category system was finalized, a codebook was developed through discursive discussions, outlining category definitions, coding rules, and anchor examples. All transcriptions were then recoded using the code system and MAXQDA software version 20.0.8 (VERBI Software GmbH, Berlin, Germany).
Table 1 displays relevant excerpts from the category system, which consist of 3 hierarchical levels. The category system includes 5 main categories and a total of 33 top and subcategories. This study specifically focuses on the categories “social environment,” “personal history,” and “health situation.” Following coding, the original statements made by the study participants were paraphrased and generalized. Finally, pertinent quotes and generalizations related to the study themes were compiled from the interviews, subjected to comparison and interpretation.
Excerpts From the Category System.

In the results chapter, the primary assertions of the participants are reinforced by direct quotations from the interviews. The discussions were translated into English using forward translation. The quotes and Table 2 are marked with the following abbreviation: “I” represents Interviewees.
Overview of Sociodemographic Characteristics of Participants.

Parent or grandparent of minor children.
Results
Description of Cohorts
Qualitative component
A total of 27 individuals responded to the interview invitation, but only 25 interviews were conducted and evaluated. One person withdrew their consent without stating a reason, and another had to cancel due to health issues. The participants were recruited regardless of their parenting tasks, as 1 aim of the study was to find out to what extent parental status is a relevant issue in the context of long COVID and what the proportion of people with parenting tasks is in a sample of people with long COVID from the general population. Furthermore, a parallel analysis of people with and without parenting tasks was intended to identify possible differences between these groups in terms of daily life experiences, burden, social participation, mental health, and quality of life. The mean age of the participants was 44.5 years (min: 21 years, max: 67 years). Most of the participants were female (n = 18, 72%). A majority of 84% (21 participants) reported being employed. Table 2 displays the selected socio-demographic characteristics of the participants, arranged chronologically based on the date of data collection. The interviews occurred between January and May 2022 and had an average duration of 38 min (min: 17 min, max: 57 min)).
Quantitative component
Out of 1,901 enrolled participants, 920 participants were included in the data analysis (Figure 1). From 920 participants 69.0% (n = 635) had long COVID, and 30.1% (n = 277) participants had children and adolescents aged 17 years or younger in their households. Participant characteristics with mean and standard deviation of the examined measures stratified by their COVID statuses are shown in Table 3. Comparison of characteristics of included and excluded participants is shown in Supplemental Table 1. Stated long COVID related symptoms with their self-perceived severity are presented in Supplemental Table 2.

Flowchart.
Characteristics of Enrolled Subjects Stratified After Long COVID Status (N = 920).

Data is n (%) if not stated otherwise.
Some or extreme impairments according to EQ-5D-3L.
Social Participation
Qualitative results: Living situation, daily routines, and social participation of parents with long COVID
As shown in Table 2, 9 of the 25 interview participants have parenting tasks for a child or grandchild. During the interviews, several long COVID parents and grandparents, highlighted significant difficulties in caring for and supporting their children. Individual parents of minor children reported that they lacked physical energy to prepare meals for their children or pick them up from kindergarten. Other parents of school-age children experienced difficulties in maintaining the support they had provided before long COVID with homework or studying for exams. One grandfather pointed out that he was no longer able to visit his grandchild and support his daughter in coping with parenting tasks due to his reduced physical resources. “I can no longer care for my grandchildren [. . .] because it’s far too exhausting” (I11, male, 67 years). These limitations or challenges posed a substantial burden, making it much more challenging or even impossible for them to engage in other social or leisure activities.
“I also realize that I just can’t be there for the kids as much. That I can’t support them as much. On bad days, it’s often too much already that I have to go about my day and I actually forget things. So they tell me ‘next week I’m writing an English test’ and then I say ‘then let’s study for it and we can do this and that.’ And I really can’t remember two days later.” (I5, 44 years, female)
“Yes, there [in the realization of hobbies and vacations] I simply notice my illness very much, because the combination of the illness and the small children makes it so that I am glad that I can manage the daily routine here in the meantime and know how we manage it.” (I1, 30 years, female)
These female participants indicate that parenting tasks can help to maintain daily routines and protect against social isolation. Still, the combination of long COVID symptoms and parenting tasks create a situation in which activities beyond daily routines and childcare, such as leisure and relaxation, or engaging in social gatherings with friends and acquaintances, can no longer be pursued, or are severely limited. This experience is shared by 2 other male participants, who stated that without parenting tasks, they would not leave the house and see people from other households. Simultaneously, they give up activities that do not relate to the household or childcare to be able to cope with them and fulfill their role as a father.
“I try to use the resources that I still have available somehow here in the household to fulfill my part here at home. Whether it’s the commitment of a family home or the children. That’s sport enough.” (I17, male, 37 years)
One employed mother explained that her daily routine is so busy with work, parenting tasks, and appointments related to the treatment of her long COVID symptoms that she has neither the time nor the physical resources for other activities.
“I get up at half past five and then I make breakfast for the children and then I take them to the station because they take the train to school. And then I get ready myself and drive to school. At the moment, because I’ve been ill so much, I’ve had a limited timetable. That means I had school from eight to one. [. . .] And then I came home and then I continued with the appointments for the children, but also with my appointments for physiotherapy, massage, and whatever else. Then at some point in the evening I just fell into bed and, if I was lucky, I was able to sleep.” (I22, female, 48 years)
These examples show that the different complaints, symptom severities, daily life limitations, and disease progression in the context of long COVID also result in different limitations and challenges regarding parenting tasks. While some parents or grandparents with long COVID are just able to manage the tasks with a high use of physical resources, for others this is no longer possible or only to a limited extent. The 9 participants with parenting tasks have in common that their physical resources are exhausted after (or even before) they have completed their parenting tasks, that they are usually unable to pursue any further activities, and that they therefore experience considerable limitations in their social life and leisure time. This in turn has a negative impact on their well-being, perceived quality of life, and mental health. Several parents or grandparents with long COVID struggled with their situation and felt that they were no longer able to fulfill their role as parents or grandparents and no longer participate in social or family life. This led to frustration, sadness, hopelessness, or anxiety and therefore represented a major emotional burden for them.
“It’s such a vicious circle, because then you can no longer take part in family life or you’re no longer a support for the family. The children also realize ‘Mum’s not well, I’d better not bother her with it’.” (I22, female, 48 years)
Quantitative results
IMET sum scores were not significantly associated with gender at birth or parenting tasks. Significant covariates were significantly age, employment status, and long COVID status (Table 4). Participants aged between 51 and 67 years were associated with significantly higher IMET sum scores compared to participants <30 years. A higher IMET sum score was significantly associated with being currently unemployed compared to full-time employment and with currently having long COVID compared to currently not having long COVID (Table 4).
Regression Analysis (N = 920) of IMET Sum and Item “Family and Domestic Responsibilities” Score.
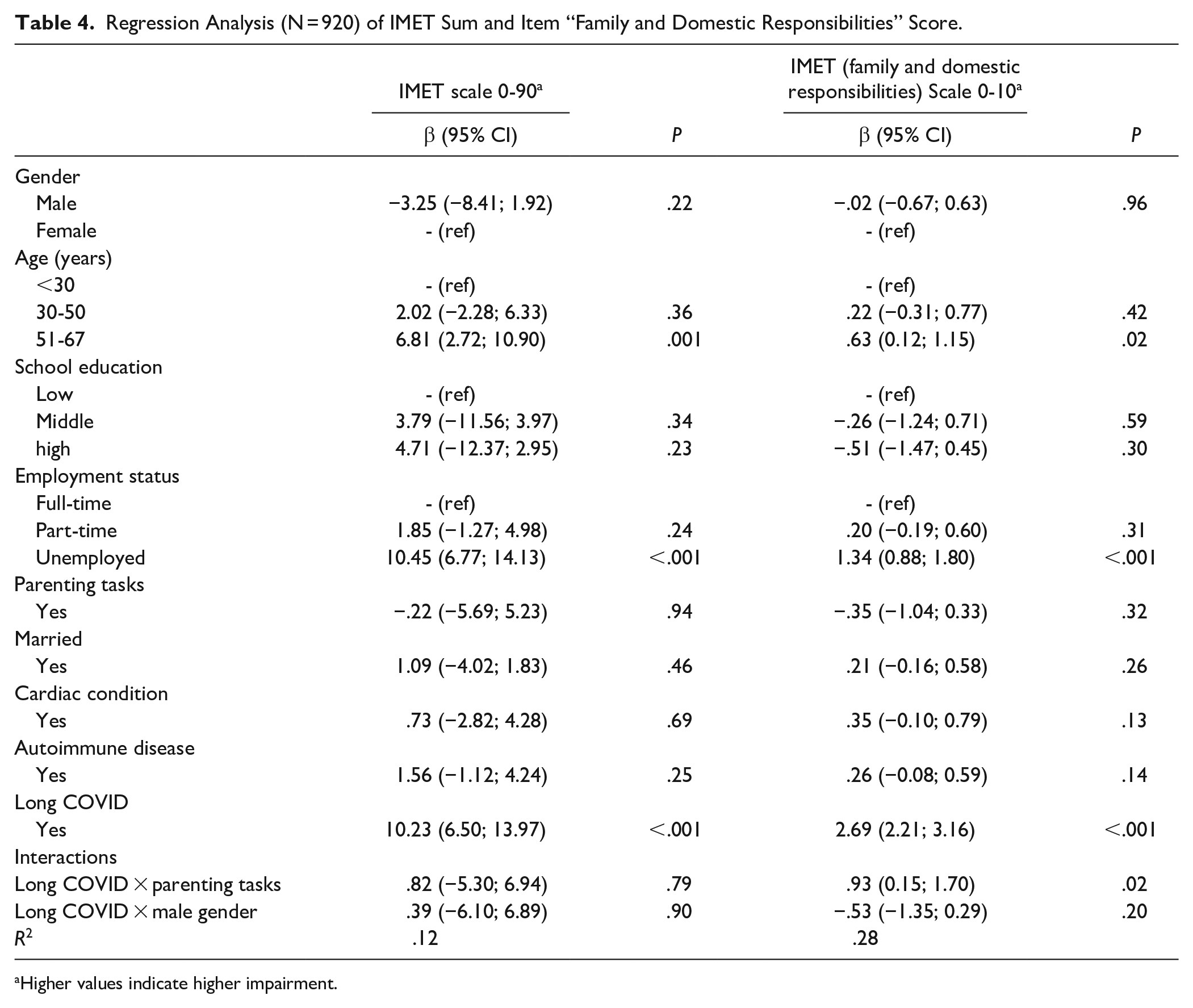
Higher values indicate higher impairment.
A significant interaction between the long COVID status and parenting tasks was observed when investigating IMET scores of the item representing “family and domestic responsibilities”. Raising children was associated with higher IMET item scores in participants with long COVID but not in participants without long COVID (Figure 2). The same covariates were significantly associated as in the IMET sum scores (Table 4).
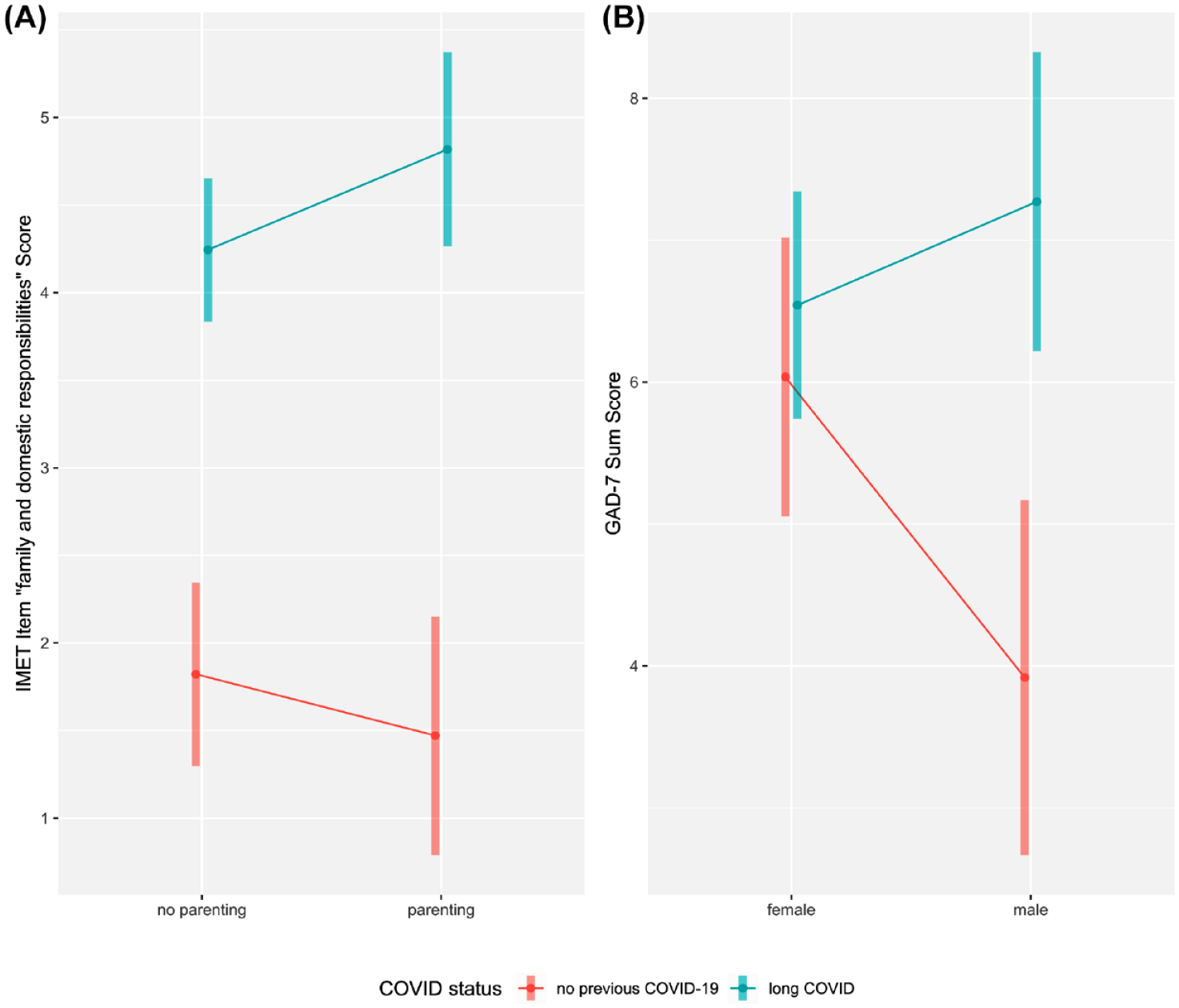
Interaction with its 95% CI between COVID status and parenting tasks on IMET item “family and domestic responsibilities” scores (A) and COVID status and gender on GAD-7 sum scores (B) adjusted for gender, age, school education, employment status parenting tasks, long COVID, cardiac condition, and autoimmune diseases. Higher scores indicate higher levels of depression or impairment of social participation.
Health-Related Quality of Life
Multiple linear regression model revealed significantly higher EQ-5D index values for men compared to women. Parenting tasks and interactions between gender, long COVID status, and parenting tasks were not significantly associated with EQ-5D index values. Other significant covariates that were associated with EQ-5D 3L index values included low school education (vs high school education), being unemployed (vs full-time employment), long COVID status, and having an autoimmune disease (vs not having an autoimmune disease). For the EQ-5D VAS scores, the same variables were significant compared to the EQ-5D index scores (Table 5).
Regression Analysis (N = 920) of EQ-5D Index Value and EQ-5D VAS Score.

Mental health
Participants with long COVID (vs not having long COVID) showed higher PHQ-9 scores. Parenting tasks or gender nor its interactions with long COVID status were not significantly associated with PHQ-9 scores. Employment status was found to be a significant covariate with regard to depressive symptoms. Anxiety symptoms (GAD-7 scores) were less common among males. Additionally, an interaction between gender and long COVID status was observed on the GAD-7 sum score. In participants without long COVID, men showed lower GAD-7 scores compared to women. This was reversed in participants with long COVID, where the male gender was associated with higher GAD-7 scores compared to females. (Figure 2). Identical to PHQ-9 scores the employment status was a significant covariate (see Table 6).
Regression Analysis (N = 920) of PHQ-9 and GAD-7 Sum Scores.

Discussion
This mixed methods study revealed negative associations of long COVID with people’s usual activities of daily life (eg, leisure activities, social participation, health-related quality of life, and mental health). Furthermore, our results show that parenting tasks worsens those outcomes, due to the increased burden of complaints during and after care work and difficulties in coping with parenting tasks. Gender differences were found in anxiety symptom severity between individuals with and without long COVID.
Social Participation
Long COVID was strongly associated with impaired social participation in the quantitative survey. The qualitative study section echoed these findings, with interviewees describing multiple challenges such as maintaining close relationships, attending gatherings with family and friends (eg, common tasks and activities can no longer be performed, and appointments often have to be canceled at short notice, which sometimes leads to tensions), as well as the rebound of long COVID symptoms after performing usual activities of daily life, resulting in a lack of energy for leisure activities.
Quantitatively, parenting tasks were associated with higher social participation among those without long COVID but were associated with lower social participation for those with long COVID.
The qualitative findings of this study suggest that on the one hand, parenting tasks can help maintain fixed daily structures. On the other hand, there were finding that coping with long COVID symptomatology and pursuing parenting tasks limit the ability to perform any activities beyond managing usual activities of daily life and caring for children, such as leisure activities, or attending social gatherings. Some interviewees reported major limitations in caring for their children, resulting in a feeling of failing in parenting tasks.
Studies on various chronic medical conditions, including type 2 diabetes, 50 chronic mental health conditions, 31 major amputations, 51 and chronic bowel diseases, 52 have consistently reported impaired social participation. de Coninck et al 53 analyzed the functionality and social participation of people with chronic conditions using in-depth qualitative interviews. Using an analytical framework based on various dimensions of social participation, they revealed interdependences between health conditions, social activities, body functions, and environmental and personal factors. These findings mirror what we observed in our study regarding long COVID, where the health condition itself, its impact on bodily functions, and social environmental factors such as employment and parenting tasks all intersect to affect social participation. Participants of another study by Wurz et al 54 reported limited opportunities to engage in social activities as a result of long COVID symptoms, similar to participants in this study. The change of participation and social environmental factors can lead to a change of the health condition for example, through less physical activities and less social contacts.
It is crucial to recognize that the symptoms of long COVID are highly variable and often fluctuating. 3 This variability underlines the need for tailored interventions and support structures, moving away from the idea that one-size-fits-all solutions, as often promoted in evidence-based research, are sufficient.55 -58 Various social factors and medical comorbidities among our studied population showed different impacts on social participation, which needs to be considered when developing interventions and support structures.
Health-Related Quality of Life
Quantitative data revealed that individuals with long COVID showed considerable impaired health-related quality of life compared to those without long COVID. Gender or parenting tasks showed no impact on hrQoL when stratified by long COVID status. The qualitative data illustrated various ways in which long COVID symptoms can impair hrQoL. Participants reported that the uncertainty about the course of the condition, the multiple health and social impairments, and the resulting limitations in family, work, and leisure time lead to frustration, despair, or anxiety. This emotional burden is exacerbated when participants feel they cannot fulfill their parenting tasks or are limited in activities that are meaningful to them and are part of their social lives because parenting tasks completely deplete the energy resources reduced by long COVID. These interdependencies between health status and social participation limitations are also represented in the International Classification of Functioning, Disability and Health (ICF) framework by the WHO. 59 Like the ICD, the ICF is an international classification system. It refers to the classification of functioning, disability, and health.
Other quantitative studies showed impaired hrQoL in persons with long COVID, often without a comparison to non-long COVID individuals or without adjustments for social demographic and medical factors.60,61 Malesevic et al 62 used the EQ-5D and SGRQ as an instrument for quantifying hrQoL; they reported comparable impairments in the EQ-5D dimensions of usual activities, pain/discomfort, or anxiety and the SGRQ activity component among long-COVID individuals from Switzerland. Malesevic et al showed similar results to our study’s finding for example, a lower hrQoL compared to individual without long COVID during the COVID-19 pandemic in a cohort with comparable gender and age proportions. Also, as long COVID is a disease with heterogeneous symptoms, it is associated with different impaired health dimensions between the individuals. 3 The variety of symptoms in persons with long COVID and different social impairments could also be observed in our qualitative and quantitative findings.
Mental Health
In quantitative analyses, long COVID was significantly associated with mental health, particularly higher depressive symptoms. Gender differences emerged concerning anxiety symptoms: Similar to studies covering the general population,63 -67 females in the non-long COVID group displayed higher levels of anxiety compared to males; however, in the long-COVID group, men reported higher anxiety levels than females. In the interviews, several participants reported depressive symptoms, feelings of sadness or dejection, reduced psychological resilience, and disturbances in sleep patterns. In addition, some participants expressed pessimism about their future private, occupational, and health situations. Participants described an emotional downward spiral, resulting in a perceived lack of perspective. Notably, qualitative data did not exhibit gender disparities in these aspects.
The prevalence of anxiety disorder is generally higher in females, a pattern that continued during the COVID-19 pandemic.63 -67 While higher anxiety levels were also observed in study participants without long COVID, in long COVID this gender difference was inverted. While other studies associated the female gender with a higher prevalence of long COVID.68 -70 differences in symptom were not examined but could explain our results.
While the long COVID status in interaction with the occurrence of parenting tasks showed no association with mental health in our study, other studies show difficulties in managing parenting tasks in parents with mental disorders. Van der Werf et al 71 report that half of the adolescents surveyed with chronically ill family members in the household experienced negative consequences in daily life. Mental illnesses were more likely to have negative consequences in daily life than physical illnesses. A meta-analysis on parenting with mental illness of qualitative findings identified parenting difficulties such as the connection to the child, struggling for control and amplification of struggle due to symptoms and medication. 72 Also, parents without support experienced the most significant challenges and some found it unrealistic to raise a child alone.
A meta-analysis identified decreased anxiety symptoms, sleep disturbances, PTSD, and depression as among the most common psychological symptoms in persons with long COVID. 73 Hossain et al 74 reported that especially the fear of getting sick, becoming infected again, or infecting others impairs the psychosocial well-being of persons with long COVID. Moreover, social stigma around mental health problems further hinders affected individuals from sharing their concerns with others. Scholz et al 75 highlighted the role of social stigma in the context of long COVID that may result in further mental health impairments: applying a cross-sectional online survey, they found that experiences of social stigma of people with long COVID lead to increased perceived stress, depressive symptoms, and higher levels of anxiety. The large number of ongoing studies into the causes and various innovative therapeutic approaches (eg, online occupational therapy 76 ) for long COVID could help to reduce this stigma and improve the care in the future.77,78 In addition, care guidelines should be kept up to date due to extensive research and communicated with medical service providers and social organizations to enable evidence-based care.
Strengths and Limitations
This study comes with several limitations. The quantitative survey was based on a cross-sectional study and does not allow for the establishment of a temporal relationship between examined factors and outcomes. Our sample is based on a convenience sample and therefore not representative of the German population. For example, more women and persons with a high school education were included in our study than make up the general German population as a percentage. As we used an online survey that was only available in the German language, people with limited proficiency of the German language and people without internet access were excluded. The survey was conducted as a self-assessment, and long COVID was not objectively diagnosed. Comprehensive sociodemographic data (eg, household income) and health conditions that may pose an impact on the outcomes was not collected in this study. Further parenting tasks were defined only 2 binary questions (“Do you have children?” and “Do children under 18 live in your household?”) which does not quantify the parenting demands or provide the age of the child(ren) which could have an influence on the outcomes.
The qualitative research involved a total of 25 adults and was conducted over a 5-month period in 2022. The sample size was in accordance with established guidelines for qualitative research, which recommend conducting at least 12 interviews.24 -26 A limitation relevant to the thematic focus of this study is that only 9 of the 25 interview participants stated that they had parenting tasks and that men (28%) are underrepresented in this sample. Furthermore, the majority of the participants were employed individuals of German origin residing in the federal state of Lower Saxony. Certain population groups, such as individuals with a migration background, older adults, and those with a lower level of education, were also not adequately represented in the samples. Individuals with severe long COVID who were unable to engage in a 1-h conversation were excluded from the study. However, by providing the option for videoconferencing interview options, we were able to include participants with impaired mobility who otherwise could not have participated in the study.
Conclusions
Our study suggests that parenting tasks in the context of long COVID have a negative impact on social participation. Furthermore, long COVID complaints can lead to limitations in the performance of parenting tasks, which may result in role conflicts and impairments in health-related quality of life or mental health. The situation of parents with long COVID should be given more attention in future research and health policy to address inequities. Gender differences could be observed in hrQoL and mental health. Further studies are needed that explicitly recruit parents with long COVID from various socioeconomic statuses and with different living situations, family constellations, and parenting models, focusing on parenting’s impact on health, social life, mental health, and quality of life. Robust support services, including financial aid for household help, childcare, and counseling, can alleviate perceived social limitations, given individual life situations and the disease’s heterogeneity.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241255592 – Supplemental material for Parenting and Gender as Impact Factors for Social Participation, Quality of Life, and Mental Health in Long COVID
Supplemental material, sj-docx-1-jpc-10.1177_21501319241255592 for Parenting and Gender as Impact Factors for Social Participation, Quality of Life, and Mental Health in Long COVID by Dominik Schröder, Tim Schmachtenberg, Stephanie Heinemann, Christina Müllenmeister, Sascha Roder, Iman El-Sayed, Gloria Heesen, Gloria Königs, Alexandra Dopfer-Jablonka, Eva Hummers, Marie Mikuteit, Christian Dopfer, Simon Grewendorf, Jacqueline Niewolik, Sandra Steffens, Valerie Doze, Frank Klawonn and Frank Müller in Journal of Primary Care & Community Health
Footnotes
Author Contributions
All authors contributed to the study conception and design. The first draft was written by Dominik Schröder, Tim Schmachtenberg, and Frank Müller. Data analysis was performed by Dominik Schröder and Tim Schmachtenberg. Material preparation and data collection were done by Jacqueline Niewolik, Marie Mikuteit, Sascha Roder, and Gloria Heesen.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is part of the DEFEAT-Corona Project funded by the European Regional Development Fund (ZW7-85152953).
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Hannover Medical School (9948_BO_K_2021) and University Medical Center Göttingen (29/3/21). The study is registered in the German register for clinical trials (DRKS00026007).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
The datasets generated and analyzed during the current study are not publicly available in accordance with the decision of the involved Research Ethics Boards but are available from the corresponding author on reasonable request within a data sharing agreement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.