
Abstract
Background:
Arsenic is a well-known toxin which may contaminate household water. It is harmful when ingested over prolonged periods of time. As a result, public health experts recommend that water should be screened and treated to prevent arsenic ingestion. In the United States, the responsibility of testing and treatment of private wells falls on homeowners. Despite recommendations for routine screening, this is rarely done.
Objectives:
To assess the prevalence of well water use in a Midwestern patient population, how patients and clinicians perceive the risks of arsenic in well water, and whether additional resources on well water testing are desired. These findings will be used to influence tools for clinicians regarding symptom and examination findings of chronic arsenic exposure and potentiate the distribution of informational resources on well water testing.
Methods:
Surveys were sent via email to all actively practicing primary care clinicians at the Mayo Clinic in the United States Midwest, and all active adult patients at the Mayo Clinic in the same region. Our team analyzed survey data to determine whether both patients and clinicians are aware of the health effects of chronic arsenic toxicity from well water, the need for routine well water testing and whether each group wants more information on the associated risks.
Results:
Both patients and primary care clinicians worry about arsenic exposure. Patients with well water are concerned about their water safety yet feel uninformed about testing options. Clinicians do not know how prevalent well water use is among their patients, feel uninformed about the chronic risks of arsenic exposure and the physical examination associated with it. Both groups unanimously want more information on testing options.
Conclusions:
Our findings show a significant reliance on well water use in the American Midwest, and unanimous support for the need for further well water testing information and resources for patients and their clinicians.
Introduction
Arsenic is a well-known toxin which may contaminate potable water sources. It is harmful when ingested over prolonged periods of time, resulting in negative health outcomes. As a result, public health experts recommend that water should be screened and treated to prevent arsenic ingestion. In the United States this is routinely done for communal water, though responsibility for testing and treatment of water from private wells falls on homeowners. Despite recommendations for routine screening, this is rarely done.1,2
Arsenic cannot be seen, tasted or smelled and can vary in concentration between water wells, even in neighboring areas. 3 The variability in arsenic concentration in ground water is due to the arsenic content of the aquifer materials and the varying processes that dissolve arsenic from surrounding sediment into the water. 4
Chronic arsenic exposure has been associated with the development of diabetes mellitus, hypertension, skin cancer, renal, bladder and lung cancers, polyneuropathy, and cardiac QTc prolongation.5 -9 While these conditions are correlated with arsenic exposure, the time of exposure and disease latency mean that direct causation is extraordinarily difficult to prove. 10 Emerging data show that exposure to arsenic during pregnancy is associated with gestational diabetes in the pregnant mother and low birth weight of the newborn infant. 7
Many symptoms attributed to other conditions may in fact be due to chronic arsenic exposure given their overlap in presentation and latency. For example, 1 case reports an adult patient in Minnesota who reported high arsenic concentrations in her private well after she had 4 dogs die. 11 She requested arsenic level testing to assess the state of her health, stating that this was not something she was aware of as a health risk previously.
The presence of increased concentrations of water contaminants such as arsenic are associated with greater cancer-related mortality in rural populations. 12 In fact, in a comparative cross-sectional study of 172 pregnant women, umbilical cord blood was collected at the time of delivery and analyzed for 20 inorganic elements. Significant differences were found between 2 elements in urban and rural samples. 13
Currently 13% of the American population relies on private wells. 14 The majority of the population is serviced by approximately 150 000 public water systems, with the remainder relying on purchased drinking water that must be transported into the area. 14 The Environmental Protection Agency currently regulates 90 common drinking water contaminants by establishing maximum contaminant levels of substances such as arsenic, nitrates, uranium, and toxic organic entities including pesticides and solvents. 14 Arsenic is found in substantial amounts throughout the United States, aside from the Southeast. 4 In a study by the United States Geological Survey, half of all wells sampled in aquifers used for drinking water nationally had traces of arsenic, with 7% being above the national threshold of 10 µg/L.2,15,16
American well water is not required to meet the drinking water standards of public water supplies and is often found to contain arsenic. 15 In Minnesota well water is only required to be tested once, as lack of arsenic detection initially is felt to indicate that it is unlikely to be found later. 3 Conversely, if it is detected in a newly dug well, it is recommended to be retested 6 months later as levels may vary in the initial months after well construction. 16 In their study analyzing appropriate intervals for well water testing, Mailloux et al 17 concluded that “a single analytical sample of arsenic below a maximum contaminant level is not enough to ensure that drinking water from private wells remains low because of measurement error and because arsenic concentrations change over time” and instead recommend testing at least every 5 years. 17
It is up to well owners to assess their water and eliminate arsenic through commercially obtained water filtration systems. As Zheng and Ayotte 18 write however, “Persistent optimistic bias among well owners against testing and barriers such as cost of treatment mean that a large percentage of the population will not act to reduce their exposure to harmful substances such as arsenic.” A study of 800 households by the Department of Health in Minnesota reported the following reasons in descending order for not testing among home well owners: not concerned about arsenic, not sure what to do or whom to contact, treatment options are too expensive or too difficult to maintain, and lack of time. 19 Furthermore, the survey found that people with less education, lower income, and those who did not know anyone who had tested their well were less likely to install a filtration unit. 19 Similar findings are seen throughout the United States in Maine, New Jersey, and California.20,21
There is a scarcity of data regarding whether patients and clinicians in rural areas are concerned about or even aware of the serious health risks of chronic arsenic exposure. It is likely that most clinicians do not routinely ask their patients about their use of well water or about arsenic testing. Objective data on this phenomenon is warranted given that well water is commonly used in the Midwest, and that testing, and treatment of water is readily available. Often this is subsidized by local public health authorities or non-governmental organizations. However, structural barriers make rural residents—particularly those with limited health literacy—less likely to have access to health information. 22
The aim of this current study was to collect data from both patients and clinicians on the self-reported prevalence of well water use in the American Midwest and their knowledge regarding the importance of testing for arsenic, including the risks of long-term exposure. To our knowledge, this is the first study elucidating clinician knowledge on the risk and symptomatic presentation of patient arsenic exposure from well water. This study is a qualitative cross-sectional survey of patients’ and providers’ current knowledge on the health risks of arsenic by using an exploratory research methodology through a qualitative model.
The purpose of collecting this data is to inform future tools that clinicians and patients may find useful such as adding an additional question in the social determinants of health registration questionnaire in the electronic medical record regarding the use of well water. This would inform clinicians regarding an increased risk of well water exposure to arsenic causing medical symptoms and potentiate the distribution of informational resources on the importance and coordination of well water testing in their specific region(s). As Hendryx et al 12 stated, “better understanding of rural environmental health risks has implications for both population health and health care treatment demands that are placed on rural health care systems.”
Methods
Study Overview and Population
This study is a cross-sectional survey of patients and clinicians currently active at the Mayo Clinic and the Mayo Clinic Health System in the Midwest of the United States, comprising the states of Minnesota, Wisconsin, and Iowa. This includes Mayo Clinic Rochester and more than forty community-based hospitals and clinics across southern Minnesota, western Wisconsin, and northern Iowa. The study was reviewed and determined to be exempt from the requirement for Institutional Review Board (IRB) approval by the Mayo Clinic. Approval number 23-006613 was granted on July 31, 2023.
Data were collected from clinicians and patients to evaluate their understanding of the risk of arsenic in well water, assess their perception of how common well water use is, and determine whether they wanted additional resources for patients on how to test their specific well. Primary care physicians and researchers with expertise in survey creation were involved in developing and editing the questionnaires. Content validity of the study questionnaires was assessed by performing a pilot study of 11 volunteer patients and 10 volunteer clinicians from multiple health systems. Survey questions and results were felt to accurately assess the content domain. No further changes were made to the questionnaire prior to distribution.
Study Methods
Emails containing the survey and a consent script were sent to 2 separate groups. The first was sent to physicians and advanced practice practitioners (including nurse practitioners and physician assistants) who were assigned a panel of primary care patients within the specialties of Family Medicine, Community Internal Medicine and Community Pediatric & Adolescent Medicine. The second was sent to all adult patients over the age of 18 years with an email address who had consented to participating in research studies. Active patient and clinician email addresses fitting our study criteria were obtained from existing clinical data repositories. About 280 000 patient email addresses and 670 clinician email addresses were initially included. Those patients and families with a duplicate email address only received 1 survey (resulting in the removal of 22 367 email addresses). Survey sampling is illustrated in Figures 1 and 2.

Study protocol for inclusion of patients.

Study protocol for inclusion of providers.
Survey responses were kept confidential and de-identified prior to analysis or report to study investigators. Non-responders received 2 follow-up reminders to complete the survey. Data was then analyzed by our team and used to determine objectively whether both patients and clinicians are aware of the health effects of arsenic toxicity from well water, the need for routine well water testing and whether each group respectively wants more information on the risks of chronic arsenic toxicity.
Statistical Analysis
Survey questions were reported using frequencies and percentages for those that had answered that they had well water. There were 229 patients that reported they had well water but did not answer any additional survey questions, so they were not included in the denominator. Clinician surveys were also reported using frequencies and percentages. Chi squared test was used to assess relationship between survey answers and demographics of respondents. SAS software (SAS Institute, version 9.4) was used to develop reports.
Results
Participant Characteristics
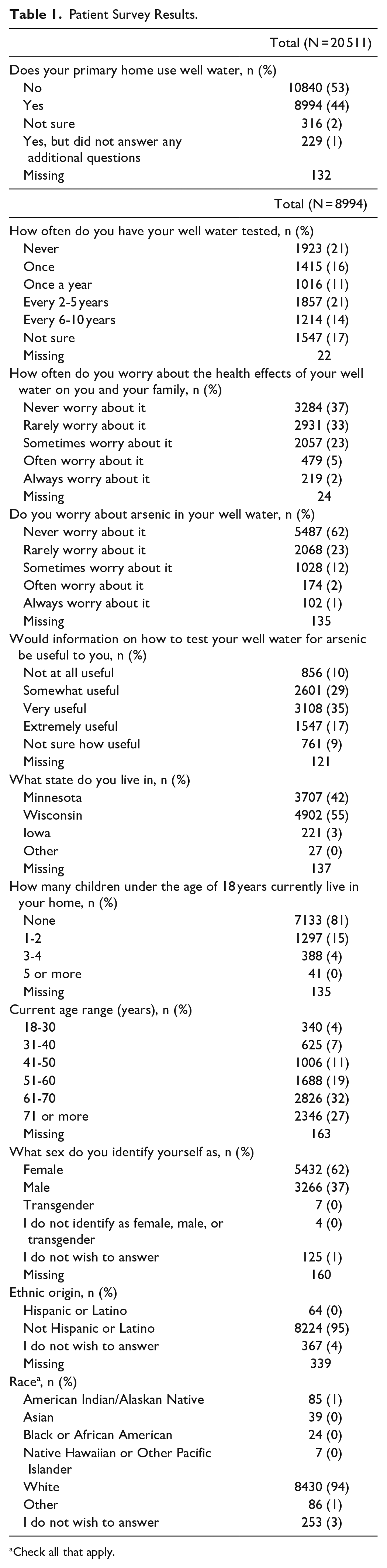
Of the 257 431 participants that were invited to take the survey, 20 511 opened the survey (8% response rate). Patients at our institution (which is actively involved in many areas of research) are frequently requested to participate in research, and as such we suspect participation fatigue was a factor. Nearly half (44%) of respondents reported primarily using private well water in their home, which is greater than the national rate of 13%, 14 Iowa rate of 7%, 23 Minnesota rate of 22%, 3 and Wisconsin rate of almost 25% 24 (Table 1 and Figure 3). After excluding 229 patients that did not answer any additional survey questions, 8994 patient participants completed the remainder of the survey. The demographics of the patients are presented in Table 1. The patient respondents were mostly female, White, older, and located in Wisconsin.
Patient Survey Results.
Check all that apply.

Patient survey participant response to whether they use well water.
Of the 671 clinicians that were invited to take the survey, 121 opened the survey (18% response rate). After excluding the 10 clinicians that did not have an assigned patient panel, a total of 111 clinicians in primary care completed the survey. The demographics of the clinicians are presented in Table 4. The clinician respondents were primarily female, White, aged 31 to 50 years, Family Medicine clinicians located in Southeast Minnesota. All survey results are available in the Supplemental Appendix.
Patient Responses
The distribution of responses from the survey of patients is presented in Tables 1 to 3. More than a third (39%) of patients reported that their well water had never been tested or were unsure if it had (Table 1). Both younger adults aged 18 to 30 years and older adults older than 71 years old reported testing their well water more frequently than other age groups (Table 2). Having children in the home was not associated with worrying about water safety or testing behavior (Table 3). A minority (37%) of patients reported never worrying about the overall health effects of their well water; however, a majority (62%) never worried about arsenic specifically in their well water (Table 3). Respondents in age groups 18 to 30 and 51 to 60 years, and female respondents as a whole, were more likely to often or always worry about health effects of their well water, with women and non-White respondents more likely to worry about arsenic specifically (Table 3). A majority (52.5%) reported information about how to evaluate well water for arsenic would be very or extremely useful.
Patient Demographic Variables in Relation to How Frequently Their Well Water is Tested.

Chi-Square P-value; There were 22 people who did not answer the question.
Patient Demographic Variables in Relation to Worry about Arsenic in their Well Water.

Chi-Square P-value; There were 135 people who did not answer the question.
Clinician Responses
Clinician responses to the survey are summarized in Table 4. Nearly half (43%) of clinicians estimated a very low proportion of their patients use well water at home (0 to 20% of their panel). Only 14.5% of clinicians report frequently or always asking about well water use. Physicians were more likely than advanced practice practitioners to report asking about well water use, and pediatricians were more likely to ask than family medicine or internal medicine physicians. Two-thirds of all clinicians (67%) reported being unaware of the health risks of chronic arsenic exposure in drinking water, and 76% did not know the physical exam findings of chronic arsenic toxicity. More than a third (39%) of clinicians did not know their community’s resources for well water testing. The majority (55%) reported it would be very or extremely useful to have general information about well water testing to share with patients.
Clinician Survey Responses.

Check all that apply.
Discussion
We found that both patients and primary care clinicians in our survey express worry about arsenic exposure. Patients with well water reported concern about their water safety yet were uninformed about testing options. Clinicians were unaware how prevalent well water use is among their patients, and felt uninformed about the chronic risks of arsenic exposure and the physical examination findings related to them. Both groups indicated a desire for more information on testing availability (82% of patients and 89% of clinicians).
The patient survey results showed significant correlations between advancing age and likelihood to test for arsenic. Those patients who were worried about both the overall health effects of well water and about arsenic in their water were older and more likely to be female. Patients who would find information useful for testing were older, female, and self-identified as White. This is consistent with previous research from the field of psychology which has illustrated greater worry regarding health risks among women versus men. 25 The clinician survey results did not show any significant demographic correlations, although pediatricians were more likely to ask their patients if they use well water.
Rural patients are more likely to use well water regularly.26,27 Existing epidemiologic studies have linked water pollution to health outcomes in rural populations.21,28 Remarkably, a large proportion of our surveyed patients use well water (45%) compared to the national average (13%), although there is likely an element of response bias favoring participation by those with well water. Primary care clinicians sampled are largely unaware of this prevalence, as over 55% indicated that they either did not know or thought that less than 20% of their patients used well water, although this would be in keeping within published Midwestern statistics. 14
Appropriate filtration is the only method known to prevent the health risks associated with exposure. As is the norm nationally, testing and filtration of personal well water requires attention at the individual homeowner level, beginning with testing, installation of filtration units, and ongoing upkeep. 29 Previous research has shown that this is not commonly done for numerous reasons, the most frequently reported being temporal and financial constraints. 19
Existing data shows that patients who are informed about the risks of arsenic in their household water and the methods of testing for arsenic adjust behavior to include switching to treated water for daily consumption for themselves and for their children.30,31 Murray et al 32 report that clinician and nursing staff discussion on the importance of water testing and reminders to test were associated with a twofold increase in the likelihood of water well testing by parents. Our study identifies a gap in knowledge among patients and clinicians that needs to be addressed.
Based on our study results, education for clinicians regarding chronic arsenic exposure will also be needed. Electronic health record functionality could be utilized to identify patients and alert clinicians to this risk. As cost of well water testing has been shown to be a barrier, addressing funding for, and disbursement methods of well water testing kits will also be crucial.
Strengths of this study include the purposeful broad sampling and representation of patients and physicians residing in the American Midwest, the original gathering of data directly from those both using well water and their clinicians, and the congruency of the patient and clinician responses, respectively.
The limitations of our study included self-selection bias in completing the survey and potential misunderstanding of the survey by patients. We received questions from patients regarding municipal versus private well use and current versus prior use. The email inviting participation itself clarified that we were researching personal water wells only, but some patients automatically began the survey without reading the instructions. Similarly, some respondents noted that they had already installed a filter for their personal well and as such, felt that their concern for their water safety had already been lowered as a result. Future work could focus on identifying patient cohorts with the greatest exposure history and consideration of objective screening for conditions deemed to be of greatest risk, as we know that there is a lag between exposure and disease onset.
Conclusion
The safety of ingested well water is an important consideration impacting individual and community health, particularly in rural regions. Our findings demonstrate a paucity of knowledge reported by patients and clinicians about the detrimental health effects of arsenic in well water. They support the need for further well water testing guidance and resources for patients and their primary care clinicians with regards to the presence of arsenic. In addition, information should be available through health systems and community education to inform and educate patients and clinicians about the importance of well water testing and mitigation with filtration of unhealthy water. Further studies are needed to determine the most efficient way to identify patients with well water and to educate these individuals and their clinicians on the importance of regular testing.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241247984 – Supplemental material for Arsenic Exposure in Well Water From the Perspective of Patients and Providers
Supplemental material, sj-docx-1-jpc-10.1177_21501319241247984 for Arsenic Exposure in Well Water From the Perspective of Patients and Providers by Dominika Jegen, Julie Maxson, Karen Fischer, Matthew Bernard, Randy Foss, Brandon Hidaka, Rachael Passmore, Jessica Sosso, Stephen K. Stacey and Tom D. Thacher in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors are grateful to each of the volunteer patients and providers who participated in survey development including Dr Ivana Croghan PhD, librarian Leslie Hassett, and the Mayo Clinic Survey Research Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Department of Family Medicine at Mayo Clinic.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.