
Abstract
Introduction:
When examining health literacy and disease specific knowledge levels across ethnicities and communities, ethnic minority groups are known to be at a higher risk of being below the average health literacy threshold which is a factor linked to poor health status and higher mortality rates. This study examined disease specific knowledge levels, perceived severity, and perceived susceptibility surrounding anal cancer and HPV-related screening behaviors.
Methods:
The following research questions were explored: (1) “What are the common themes and/or beliefs when asked about anal cancer, HPV, and preventive screening?” and (2) “What are the common themes and beliefs surrounding the severity and susceptibility of contracting anal cancer?”. This study utilized a cross-sectional design to survey 26 individuals regarding their knowledge level and perspectives regarding anal cancer and HPV. An 8-question survey was developed de novo based on an application of the Health Belief Model (HBM) elements. This study employed thematic analysis to explore critical themes to construct a model to understand knowledge levels, attitudes, and risk perceptions regarding anal cancer and intention to participate in preventive screenings. The fundamental attitudes and themes related to anal cancer risk and intention to participate in preventative screenings were elicited using a qualitative descriptive technique. Coded data was utilized to analyze themes based on (1) knowledge and (2) perceived risk, both severity and susceptibility.
Results:
Overall, the findings indicate very low levels of knowledge regarding screening, anal cancer, and HPV across all genders. The low levels of anal cancer and HPV knowledge were seen in 13 coded segments (50% of surveys) which showed no familiarity with or comprehension of HPV, and 4 coded segments indicated no familiarity with anal cancer. In addition, 15 respondents (57%) had low or no preventive or screening-related knowledge. While some respondents (46%) illustrated high perceived severity for anal cancer, only 23% indicated high perceived susceptibility for anal cancer.
Conclusion:
The results from this study may be used to inform practitioners, providers, and policymakers in developing interventions addressing low levels of understanding and disease specific knowledge surrounding anal cancer in support of creating a standardized health screening procedure.
Keywords
Introduction
Across ethnic groups and communities, inequities in health have been attributed to low health literacy rates and gaps in related knowledge regarding disease specific processes and risks. When examining health literacy and disease specific knowledge levels across ethnicities and communities, ethnic minority groups are at a higher risk of being below the average health literacy threshold, and limited health literacy has been linked to poor health status and higher mortality rates. 1 Three types of health literacy impact individuals’ health outcomes: functional health literacy, interactive health literacy, and critical health literacy—each dimension of health literacy aids in understanding the varying health outcomes across communities. Interactive health literacy specifically encompasses an individual’s ability to develop and apply knowledge regarding a specific health risk or health behavior. The complexities of defining health literacy stem from varying cultural values, beliefs, economic systems, and environmental factors. Yet, researchers in the healthcare setting have defined health literacy as the capacity individuals have to obtain, process, and understand the basic health information and services needed to make appropriate decisions about their health. 2 However, evidence-based approaches to improving health literacy through patient education can generate systematic changes via community organization and engagement with healthcare providers. 2 The importance of health literacy in health communication cannot be overstated. With a wide range of definitions, all of which reflect the complexities of what it means to be health literate, health literacy is proliferating and demands more interdisciplinary audiences to recognize the multifaced structure that comes with health literacy rates.
Cancer is the leading cause of mortality globally, with approximately 10 million fatalities expected in 2020, accounting for roughly 1 in every 6 deaths. 3 In low- and middle-income nations, cancer-causing diseases, such as the human papillomavirus (HPV), account for around 30% of cancer cases, with breast, lung, colon, rectum, and prostate cancers being the most frequent malignancies. 4 However, many cancers can be cured if caught early and appropriately treated. Various cancer disparities affect all demographic groups in the United States. Particular groups endure a disproportionate burden of cancer relative to others owing to social, environmental, and economic disadvantages. Social determinants of health, behavior, biology, and genetics all of which can have a substantial influence on cancer risks and outcomes.
There is increasing evidence that adults with lower health literacy and less knowledge regarding key health risks are less likely to use preventive health services such as cancer screenings, thus having higher mortalities. 5 Cancer beliefs, information-seeking habits, and perceived control over cancer risks are all linked to low levels of health literacy. 6 There is a high correlation between health literacy and education. 7 Thus, it is vital to understand that low health literacy is a social determinant of health significantly associated with cancer-related disparities. 2
Anal cancer is a condition in which the tissues of the anus develop malignant (cancer) cells. 8 HPV frequently causes this form of anal cancer. The incidence of anal cancer in the U.S. increases in men and women. 9 According to the National Cancer Institute, anal cancer affects roughly 8590 persons in the United States annually. 10 Compared to cancers of the colon or rectum, anal cancer is relatively uncommon; However, anal cancer is rare; the American Cancer Society estimates anal cancer in the U.S. in 2023 will be about 9760 new cases, with an estimated number of 1870 people who will pass away from Anal Cancer. 9 At the same time, domestic cases of anal cancer for women are 6580 per year, while cases of anal cancer annually for men are 3180. 11
The primary risk factor for anal cancer is HPV infection. HPV is a collection of more than 150 related viruses that cause cervical cancer and other types of cancer. HPV has been classified by the International Agency for Research on Cancer as a human carcinogen for several cancer types, including cervical and anal cancer. 12 Women who have had cervical cancer (or pre-cancer) have a higher chance of developing anal cancer. More specifically, the incidence of anal cancer in the U.S. has increased in both men and women. 9 Increasing evidence indicates that oncogenic strains of HPV, subtypes explicitly HPV-16 and HPV-18, cause anal cancer. 13 Annually, there are an estimated 27 000 new cases of anal cancer worldwide, with a ratio of females to males as high as 5:1. 14 Thus, the need for increased awareness of screening for anal cancer precursors is high.
Preventative screening tests can aid in detecting cancer in its early stages before symptoms occur. If discovered early, treating or curing aberrant tissue or cancer may be easier. Between 30% and 50% of malignancies can be avoided by avoiding risk factors and using evidence-based preventative measures. 4 Accessible preventive health services such as vaccines and screenings specifically for HPV are vital in ensuring patients can prevent diseases such as anal cancer. Although there is a vaccine to prevent HPV, the vaccine was only recently introduced in 2006. 11 Thus leaving older individuals still at risk of developing some form of HPV and HPV-related cancer.
There are preventive measures in place for various types of cancers. There are screening recommendations for cervical cancer; there are no official national screening recommendations for anal squamous cell carcinoma (SCC). 15 With the prevalence rate of cervical cancer at 50 cases per 100 000 before the cytologic screening, guidelines for preventative screening for women were implemented, and it is currently 7 cases per 100 000 women after screening began. 16 Yet, with domestic cases of anal cancer in women rising more than in men, according to the American Cancer Society, anal cancer screening tests are not usually suggested for everyone. Nonetheless, some specialists advise anal cytology testing for patients at a higher risk of anal cancer. 9
Anal cancer has historically had a very high mortality rate, but because of advancements in treatment, it is now growing increasingly treatable. 17 Yet, currently available evidence indicates that knowledge of anal cancer 20and its dangers is not widely disseminated. 18 In more recent population-based research of people in the U.S., awareness of anal cancer was found to be generally poor and to have remained so from 2014 to 2017. 18 The generalizability of these studies is uncertain, given their dependence on convenience samples drawn without regard to probability. Thus, the creation and effectiveness of specialized health education initiatives aimed at anal cancer require more investigation.
Purpose of the Study
This study examined disease specific knowledge levels, perceived severity, and perceived susceptibility surrounding anal cancer and HPV-related screening behaviors across genders. In order to gain an understanding of the participant’s interactive health literacy pertaining to anal cancer and HPV, the knowledge levels, perceived risks, and perspectives regarding screening were explored. The overall purpose of this study was to explore common themes and beliefs surrounding anal cancer, preventative screening, and HPV through qualitative methods. Specifically, this study employed thematic analysis and employed continuous data collection and review methods present grounded theory to explore critical themes and construct a model to explain and characterize knowledge levels and perceptions regarding anal cancer risk as well as intention to participate in preventive screenings.
Methods
A qualitative descriptive technique elicited the fundamental attitudes and themes about participant’s knowledge and knowledge and attitudes related to anal cancer and HPV risk and the intention to participate in preventative screenings. The following research questions were explored, (1) What are the common themes and beliefs when asked about anal cancer, HPV, and preventive screening? (2) What are the common themes and beliefs surrounding the severity and susceptibility of contracting anal cancer? To aid in the exploratory processes of examining common themes and elements surrounding anal cancer, preventative screening, and HPV, this study used a cross-sectional design to survey people about their knowledge level and perspectives regarding anal cancer and HPV severity and susceptibility. An 8-question survey was developed and administered de novo (see Supplemental Appendix A). The survey and data collection protocol were approved by the California Baptist University Institutional Review Board (IRB).
The survey included 3 questions regarding demographics (age, gender, and ethnicity) and 5 open-ended questions constructed based on applying the Health Belief Model (HBM) elements of perceived susceptibility and severity to anal cancer health literacy. The HBM encompasses various components theorized to explain why people participate in preventive medicine, screening, and management. Perceived susceptibility and severity of a medical condition are “perceived threats” combined. Additionally, environmental cues cause behavior and affect personal beliefs, such as perceived advantages and vulnerability. In contrast, self-efficacy affects perceived danger (perceived susceptibility and severity) and perceived rewards versus perceived barriers, which supports the start of a health behavior change.
The population for this study was adults ages 18 to 99 years at an underserved family practice clinic in Southern California, inclusive of all genders but with a special focus on capturing the perspective of underserved female patients. Participants were recruited from a predominantly underserved community in Riverside County and primarily included participants insured through managed Medi-Cal benefits offered by Inland Empire Health Plan (IEHP). Participants were asked to participate in a non-identifiable survey via pen and paper and complete it in the clinic office. In total, the study obtained a sample of 26 participants. The inclusion criteria for this study included all adult patients over 18 years of age, including both adult men and women, and all age categories. Exclusion criteria include participants who do not meet the proper age requirement, including minors. The participants were given an informed consent form outlining the risks and benefits of the study, study procedures, confidentiality, and voluntary participation before being given the survey.
Initially, all survey responses were transcribed as written to understand the survey responses’ meaning, mood, context, and intent. This process was done daily by the research team to allow for review of the data and determination of theoretical saturation. Transcribed responses were uploaded and coded in MAXQDA software. Specifically, manual open coding methods were utilized to code all question responses in the MAXQDA qualitative analysis software. Following the initial open coding process, codes were grouped further into axial and selective codes using thematic analysis.
Survey questions 4, 6, and 7 were primarily utilized to assess levels of participant knowledge regarding anal cancer, HPV, and preventive screening; however, responses were also coded according to levels of perceived severity and susceptibility if respondents provided this information. Specifically, responses to survey question 4, which asks, “What do you think about when you hear the phrase ‘anal cancer’?” were coded according to whether the respondent illustrated no, some, or high levels of anal cancer knowledge. Responses to knowledge questions were also coded based on statements indicating low, medium, or high levels of perceived susceptibility or severity. An “unsure of susceptibility” code was also incorporated for those responses that indicated a lack of understanding regarding perceived susceptibility. Responses to survey question 6: “What do you know about HPV?” were coded according to whether the respondent illustrated no, some, or high levels of HPV-related knowledge. Responses to survey question 7: “To the best of your knowledge, explain preventive cancer screening?” were coded according to low, some, or high levels of screening knowledge. Survey questions 5 and 8 were created to assess the anal cancer-related perceived susceptibility of participants; however, responses to these questions and the knowledge-related questions above also provided information regarding perceived severity levels. Survey questions 5: “What do you think is your level of risk to get anal cancer?” and 8: “Do you believe you are vulnerable to contracting anal cancer?” were coded according to unsure, low, some, or high levels of perceived susceptibility. In the case where participants commented on the severity of the condition, results were also coded based on perceived severity.
The primary researcher reviewed the coding with a secondary researcher and advisor to capture accurate results and reduce the likelihood of researcher bias impacting the coded data. The researchers each worked to identify common themes in responses across surveys using inductive content analysis. The data was then reviewed to determine agreement on the main themes. The research team utilized the coded data to create open categories, axial codes, and finally, selective codes based on higher-level themes based on (1) knowledge and (2) perceived risk, both severity and susceptibility. Hierarchical models for classifying responses, including knowledge levels, perceived severity, and perceived susceptibility, were created, as shown in Figures 1 and 2 below. While the axial and selective codes were created by grouping the themes discovered through open coding, applying the core constructs of the health belief model informed the creation of the groups into the evidence-based selective code categories of risk and knowledge.
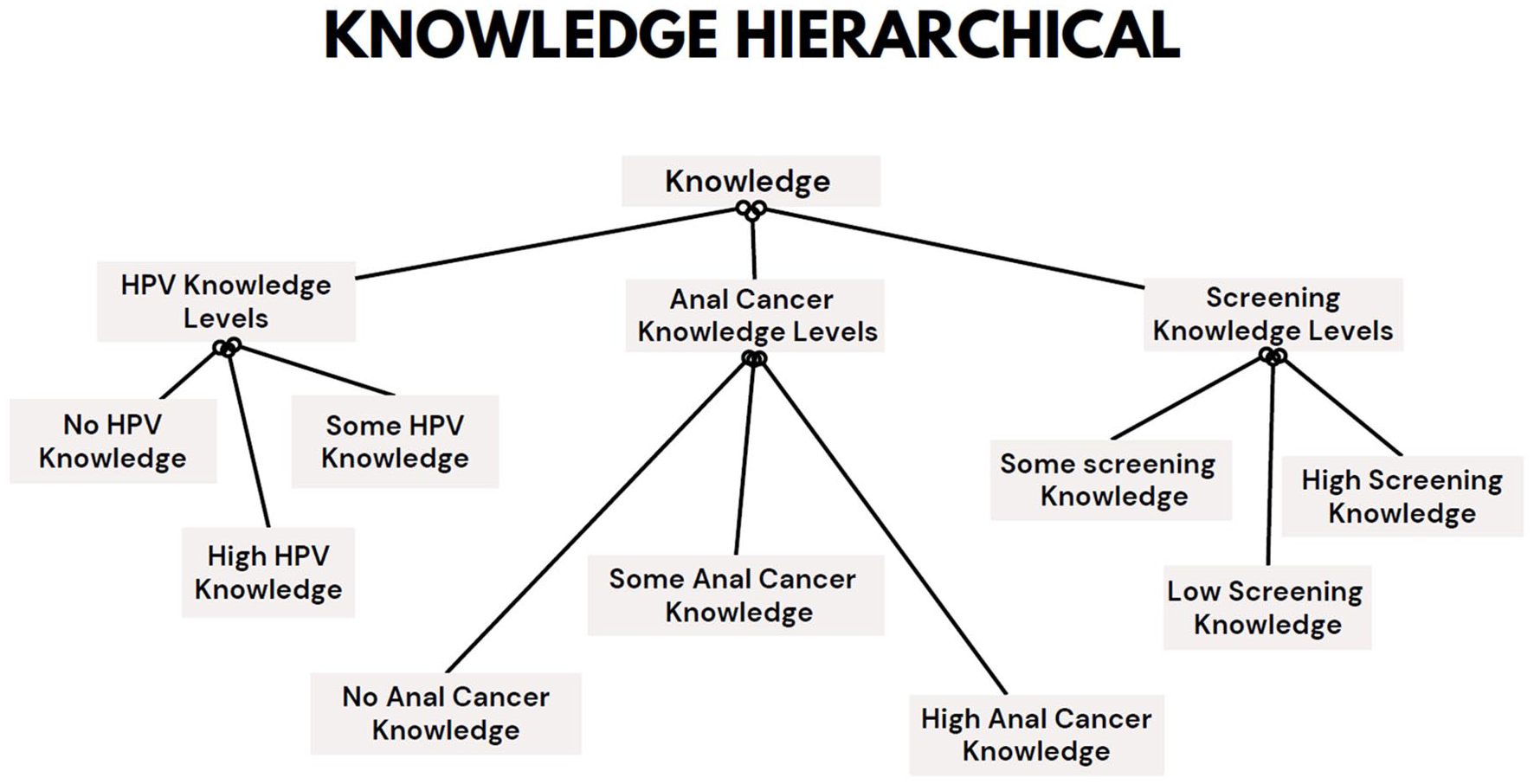
Model of codes utilized to categorize respondent knowledge levels.

Model of codes utilized to categorize respondent risk perception.
Results
Participant Demographics
The survey included 26 adult participants, all recruited from a predominantly underserved clinic in Riverside County. Of the participants, 18 (69.2%) identified as female, and 8 (30.8%) identified as men. Of the same population, 2 (7.69%) identified as African American, 11 (42.31%) identified as Hispanic, 6 (23.08%) identified as Caucasian, 6 (23.08%) identified as Asian, and 1 (3.85%) identified as Native American. Of the same sample, the number of participants whose ages ranged from 18 to 29 years was 7 (26.92%), the number of participants whose ages ranged from 30 to 39 years was 5 (19.23%), and the number of participants whose ages ranged from 40 to 59 years was 9 (34.62%). The number of participants aged 60+ was 5 (19.23%).
Manual open coding techniques in the MAXQDA qualitative analysis program were utilized to code every response to a question. Using thematic analysis, codes were further categorized into axial and selected codes after the first open coding procedure. When asked open-ended questions related to severity, susceptibility, and knowledge, the analysis revealed several findings.
Themes Identified Regarding Anal Cancer, HPV, and Preventive Screening Knowledge
Several findings were revealed when investigating research question 1: “What are the common themes and/or beliefs when asked about anal cancer, HPV, and preventive screening?” The findings revealed that the participants shared common beliefs when questioned about anal cancer, HPV, and preventative screening were presented (see Supplemental Appendix B: Table 1). Some of the participants shared the same common ideas and conceptions when asked about anal cancer. One participant’s response to the question, “What do you think about when you hear the phrase ‘anal cancer’?” was “cancer in or around the anal” (Female, 33). Participants were also asked, “What do you know about HPV?” to which many participants shared similar responses. In contrast, only1 participant (Female, 42) out of the 26 had a thorough understanding of HPV, including its prevention via vaccination and its link to cervical cancer. Only 4 people demonstrated a high degree of screening knowledge, and one of them replied, “FOBT, or fecal occult blood test,” (Female, 35) when asked, “To the best of your four knowledge, describe preventive cancer screening.”
When examining female responses against male participants, only 6% of the female responses were coded as having high HPV knowledge. In contrast, none of the male responses could be coded as having a high level of HPV knowledge. When coding for screening knowledge, half of the females’ (50%) responses could be coded as having a low level of screening knowledge. On the other hand, when coding for levels of anal cancer knowledge, specifically for some anal cancer knowledge, men (50%) had remarkably more knowledge than women (22%). Overall, the findings indicate very low levels of anal cancer health literacy—13 coded segments (13 surveys—50%) show no familiarity or comprehension of HPV, and 4 coded segments indicate no familiarity with anal cancer. In addition, 15 respondents (57%) had low or no preventive or screening-related knowledge.
Themes Identified Regarding Perceived Severity and Susceptibility
Several findings were revealed when investigating research question 2: “What are the common themes and beliefs surrounding the severity and susceptibility of contracting anal cancer?”. The findings revealed that participants showcased similar beliefs around the severity and susceptibility of contracting anal cancer, which was coded as risk perception. Participants’ perceptions of their vulnerability to anal cancer were measured specifically by survey questions 5 and 8. However, the researcher classified any replies to all survey items that indicated a level of susceptibility or severity (low, medium, or high). Responses to these and the knowledge-related questions above also revealed how severe respondents believed the disease to be. Survey questions 5: “What do you think is your level of risk of getting anal cancer?” and 8: “Do you believe you are vulnerable to contracting anal cancer?” along with any responses to other questions indicating a degree of susceptibility were categorized as unsure, low, some, or high levels of perceived susceptibility. The results were also classified according to the condition’s perceived severity when participants commented on its seriousness.
A larger portion of participants (46%) responded with comments that indicated high perceived severity. While half as many respondents indicated high levels of perceived susceptibility (23%), the total female responses coded were 27%. however, when analyzing female versus male respondents for perceived severity, over half of the responses coded for having high perceived severity (61%) were from female participants. Remarkably, the same percentage of women believed they had a low level of susceptibility. In total, 15 out of 26 (58%) surveys contained coded segments that indicated low perceived susceptibility, and 6 out of 26 (23%) contained coded segments that indicated high levels of perceived susceptibility. On the other hand, 12 surveys (46%) contained coded segments indicated high perceived severity. Only 1 respondent included a response that indicated a low level of perceived severity, which was starkly compared to the 15 respondents who indicated lower levels of perceived susceptibility.
While a large portion of participants indicated high perceived susceptibility when asked, “What do you think is your level of risk of getting anal cancer?” and “Do you believe you are vulnerable to contracting anal cancer?” comments such as “dangerous cancer,” indicating high perceived severity, was paired with “not high, for it does not run in my family,” indicating low perceived susceptibility (Female, 34). Another example of this dissonance was found in another survey, in which the participant stated “terminal,” indicating high perceived severity and “not that likely (hopefully [smiley face])” when asked about personal risk (Female, 47).
When asked, “What do you believe is your degree of risk to have anal cancer?” some individuals gave comments that suggested they were unclear about their perceived susceptibility. Responses included comments such as “I don’t know enough to make a guess” (Male, 23), “I have no idea” (Male, 24), and “no idea” (Female, 85). Additionally, according to the individual survey coding, low levels of perceived susceptibility were shared in tandem with a lower level of awareness, as shown by the statement, “Since I never hear about it, I would consider my risk level is quite low” (Male, 24). In short, a large portion of respondents believed anal cancer was life-threatening, but only a smaller portion believed they themselves could be impacted. A sampling of quotes from survey respondents has been provided in Supplemental Appendix B: Table 1 to further illustrate the low levels of knowledge and perceived susceptibility.
Discussion
The coding of the responses from participants was based on the HBM application of the perceived susceptibility and severity components to anal cancer health literacy. When asking open-ended questions about severity, susceptibility, and knowledge, the analysis revealed several findings. Some of the participants shared the same common ideas and conceptions when responding to questions on anal cancer, HPV, and preventive screening knowledge. The responses to the questions surrounding levels of susceptibility, those participants felt they had low levels of contracting anal cancer yet had higher levels of perceived severity. These findings highlight the HBM’s constructs of perceived severity and susceptibility, which define perceived severity as an individual’s ideas on the seriousness of contracting an illness or disease. According to the HBM, people who perceive high susceptibility and severity would be more inclined to avoid the disease if the health advantages outweigh the barriers and they feel they can participate in the activity. 19 There has been conflicting and ambiguous research on the effect of the notions of perceived susceptibility and severity. In general, many people’s perceptions of their own susceptibility are underestimated, even though some research suggests that beliefs about perceived susceptibility predict engaging in health-promoting behaviors like healthy eating and exercise, quitting smoking, self-examinations, and dental care. 20
Overall, low levels of knowledge were demonstrated in the survey questions, which were in line with low levels of perceived susceptibility; however, high levels of perceived severity were shown in the coded replies. In summary, a considerable proportion of respondents, especially female respondents, believed anal cancer was fatal. The contradiction around anal cancer, HPV, and preventative screening knowledge is illustrated by the fact that a lesser percentage of people thought they might personally be affected.
This study has several limitations including self-report bias and social desirability bias prominent in cross-sectional in-person survey based studies. The limited sample size was also a limitation of the study. However, sample sizes are in qualitative research are typically smaller in order to facilitate the in-depth case-oriented analysis central to this type of inquiry. 21 Limitations also come along with the framework of the health belief model (HBM). The HBM brings limitations because it does not provide a pathway for altering activities relating to one’s health and is more descriptive than explicative. Early research on preventive health practices revealed that perceived susceptibility, advantages, and obstacles were regularly linked to the desired health activity, although perceived severity was less frequently connected. Depending on the health result of interest, each individual construct is essential; however, for the model to be used most effectively, it should be combined with other models that consider the environmental context and offer change-management techniques.
Conclusions
The low levels of perceived susceptibility highlighted in this study should inform efforts to create patient education materials and inform policy change to increase patient understanding of their own personal risk. The findings in this study are impactful in helping address the importance of health literacy concerning preventative health behaviors such as health screenings, vaccinations, and lifestyle choices. Yet, when addressing interactive health literacy, which includes disease specific knowledge and perceived risks, it is essential to note that health literacy is a crucial component of an individual’s capacity to comprehend, interpret, and act on health-related information. While this study focused on representations of levels of knowledge and levels of perceived risk, this is only one element of understanding the health literacy challenges faced by women, and people of all genders, accessing anal cancer screening services. The results from this study will be used to aid practitioners, providers, and policymakers in developing interventions addressing low health literacy rates surrounding anal cancer in support of creating a standardized health screening procedure. In doing so, health inequities in preventative healthcare will debunk the stigma surrounding anal cancer, health literacy, and social inequities.
Anal cancer specific knowledge and interest in participating in screening services should be addressed through the appropriate allocation of adequate resources for both patients and clinicians. Collaborating with policy writers, healthcare professionals, community-based organizations, and professional organizations such as the American Medical Association (AMA) and National Institute of Health (NIH) to develop policies and provide funding for new initiatives that promote access to and capability of health resources. For example, according to the National Academies of Science, Engineering, and Medicine, a grassroots alliance called the Oklahoma Health Equity Campaign was established in 2008 and increased its focus on health literacy in 2011. 22 Its goal addresses the reality that Oklahoma routinely ranks last in national health rankings. Additionally, the Health Care Institute (HCI) provides health education and prevention programs that draw 80% of families to outreach activities and provide culturally sensitive materials that family members can understand and use to take action to improve their families’ health, the Health Care Institute’s mission is to strengthen the managerial capacity of Head Start agencies. 22 The program promotes parental knowledge of health warning signals, encourages parental reaction to early indicators of sickness, and directs parents to the right use of health reference resources for first-line assistance, according to qualitative assessments of results for families and staff. 21
Future research should further investigate preventive screening intentions and self-efficacy in order to create informed recommendations for increasing the provision and uptake of these services. Any strategy for tackling health literacy must increase service accessibility, create and strengthen efficient programs and policies, and promote the efficiency of the healthcare system. 23 By bringing together various stakeholders who can each provide a skill set that can help increase the integration of health literacy into healthcare; healthcare professionals may be proactive in creating partnerships to solve this issue. Improving health literacy will lead to greater self-efficacy and potentially lower perceived susceptibility paired with high levels of perceived severity, which, according to the HBM, are the best predictors of actions promoting health.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241243198 – Supplemental material for A Qualitative Analysis of Knowledge Levels, Perceived Susceptibility, and Perceived Severity Surrounding Anal Cancer and Human Papillomavirus
Supplemental material, sj-docx-1-jpc-10.1177_21501319241243198 for A Qualitative Analysis of Knowledge Levels, Perceived Susceptibility, and Perceived Severity Surrounding Anal Cancer and Human Papillomavirus by Adriana Jovanov, Ashley Parks, Cynthia Jovanov and Xolani Mdluli in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319241243198 – Supplemental material for A Qualitative Analysis of Knowledge Levels, Perceived Susceptibility, and Perceived Severity Surrounding Anal Cancer and Human Papillomavirus
Supplemental material, sj-docx-2-jpc-10.1177_21501319241243198 for A Qualitative Analysis of Knowledge Levels, Perceived Susceptibility, and Perceived Severity Surrounding Anal Cancer and Human Papillomavirus by Adriana Jovanov, Ashley Parks, Cynthia Jovanov and Xolani Mdluli in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.