
Abstract
Introduction/Objectives:
Colonoscopy completion rates after an abnormal fecal immunochemical test (FIT) are suboptimal, resulting in missed opportunities for early detection and prevention of colorectal cancer. Patient navigation and structured follow-up may improve colonoscopy completion, but implementation of these strategies is not widespread.
Methods:
We conducted a quality improvement study using a Plan-Do-Study-Act (PDSA) Model to increase colonoscopy completion after abnormal FIT in a large federally qualified health center serving a diverse and low-income population. Intervention components included patient navigation, and a checklist to promote completion of key steps required for abnormal FIT follow-up. Primary outcome was proportion of patients achieving colonoscopy completion within 6 months of abnormal FIT, assessed at baseline for 156 patients pre-intervention, and compared to 208 patients during the intervention period from April 2017 to December 2019. Drop offs at each step in the follow-up process were assessed.
Results:
Colonoscopy completion improved from 21% among 156 patients with abnormal FIT pre-intervention, to 38% among 208 patients with abnormal FIT during the intervention (P < .001; absolute increase: 17%, 95% CI: 6.9%-25.2%). Among the 130 non-completers during the intervention period, lack of completion was attributable to absence of colonoscopy referral for 7.7%; inability to schedule a pre-colonoscopy specialist visit for 71.5%; failure to complete a pre-colonoscopy visit for 2.3%; the absence of colonoscopy scheduling for 9.2%; failure to show for a scheduled colonoscopy for 9.2%.
Conclusions:
Patient navigation and structured follow-up appear to improve colonoscopy completion after abnormal FIT. Additional strategies are needed to achieve optimal rates of completion.
Keywords
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer death in the United States, accounting for over 150 000 new cancer diagnoses, and over 52 000 deaths annually. 1 Screening can reduce CRC incidence and mortality but is underutilized. The overall screening rate is 58% in the United States, and even lower among underserved populations such as persons of non-white race/ethnicity, those with low income and education, and those who are under/uninsured. 1 Non-invasive screening tests, such as the fecal immunochemical test (FIT) may increase screening rates, but effectiveness of this strategy depends on adherence to repeat annual testing after a normal result, and follow-up colonoscopy completion after an abnormal result. 2 Completion of follow-up colonoscopy is especially important, since failure to complete the screening process with colonoscopy after an abnormal result has been associated with up to a 2.4-fold increase in colorectal cancer mortality. 3 Delays in time to follow-up colonoscopy after an abnormal result can contribute to increased CRC incidence, later stage of disease, and higher mortality.4 -6 Clearly, effectiveness of a FIT-based strategy for CRC screening depends heavily on follow-up colonoscopy completion.
Despite importance of follow-up, colonoscopy completion rates are highly variable, ranging from 22% to 83%.7 -14 Populations vulnerable to adverse CRC outcomes, including those with low socioeconomic position and those of non-white race/ethnicity, may have particularly low rates of follow-up. For example, colonoscopy completion ranged from 18 to 57% among 1229 patients with abnormal FIT across 8 Federally Qualified Health Center systems that disproportionately serve populations vulnerable to poor CRC outcomes in Southern California. 7
Prior systematic reviews have summarized multi-level and multi-component strategies tested in randomized trials for promoting colonoscopy completion after an abnormal CRC screening test. Multi-level interventions focus on addressing patient, provider, and the various social factors influencing completion rates, whereas multi-component interventions focus on addressing 1 or multiple barriers at 1 level of the care process. They can both be integrated together, thereby addressing multiple stakeholders in healthcare delivery and the individual barriers within a particular level of care delivery. 15 For example, a multi-level study utilized mailed letters to patients and systems modifications to increase colonoscopy completion rates from 65.1% to 76.6%. 16 As a complimentary example, a systematic review found multi-component programs, including screening test outreach with patient navigation, could increase CRC screening. Patient navigation often includes multi-level interventions operating at patient, clinician, and health system levels delivering multi-component interventions, for example with multiple strategies for promoting abnormal test follow up among patients, such as reminders, standing orders, and identifying and facilitating resolution of barriers to completion. One review identified patient navigation as a promising strategy for increasing colonoscopy completion, with a pooled absolute increase in colonoscopy completion of 14% over usual care (95% CI: 0.2%-29%), though the estimated increase was not statistically significant.17 -19 Another review found moderate evidence supporting patient navigators and provider reminders or performance data reporting as effective strategies for improving colonoscopy completion after an abnormal stool test. 20
More evidence is needed to understand the potential impact of patient navigation, provider reminders, performance data reporting, and other interventions on colonoscopy follow-up after an abnormal screening test. Current gaps are particularly salient for community health center (CHCs) systems, where unique challenges, including constrained resources, a requirement to refer to specialists outside the primary care CHC practice, and a lack of standardized workflows and procedures might challenge successful implementation.
Our aim was to develop and conduct a quality improvement project to increase colonoscopy completion after an abnormal FIT, utilizing a multicomponent, multilevel strategy including patient navigation, and a checklist to promote results review, results communication, and other follow-up steps required for colonoscopy completion at a large CHC system. 8
Methods
Study Setting and Design
From 2015 to 2019, we conducted a quality improvement project at Family Health Centers of San Diego, the fourth largest CHC system in the United States. In 2022, Family Health Centers of San Diego saw 161 436 patients, of whom 96% were low income and 32% were uninsured. Family Health Centers of San Diego is the largest health care safety-net provider, school-based health care provider, and comprehensive HIV/AIDS services provider in the San Diego region—operating 75 sites across San Diego County. The project took place at 2 Family Health Centers of San Diego clinic sites that primarily serve Hispanic/Latinx patients.
We used the Plan-Do-Study-Act (PDSA) approach to develop and implement strategies that promote colonoscopy completion after abnormal FIT in 2 cycles. The first cycle was based on the initial patient navigation intervention, with outcomes assessed 6-months post initiation. The second cycle was based on updates to the patient navigation intervention strategies following the 6-month assessment.
Patient Selection, Data Sources, and Baseline Follow-Up Completion Rates
We identified patients ages 50 -75 years with an abnormal FIT through electronic health record (EHR) queries. In the baseline assessment phase (Phase 1), a combination of EHR queries and manual chart reviews were used to characterize data on key steps in the colonoscopy follow-up process. In the intervention phase (Phase 2), EHR queries and manual chart reviews were complemented by information recorded in a patient navigation log and registry. We first characterized usual care processes for promoting colonoscopy completion after abnormal FIT, rates of completion of key steps in the follow-up process (i.e., results communication, colonoscopy orders, scheduling, and completion) among all individuals ages 50 to 75 years with an abnormal FIT over a 6-month pre-intervention period from October 2015 through March 2016. This analysis demonstrated that out of 156 individuals with an abnormal FIT in the pre-intervention period, 85% (132/156) had a colonoscopy ordered, and 21% (33/156) had a colonoscopy completed.
Interventions
A patient navigation intervention was assessed over a period of 21 months from April 2017 to December 2019. We utilized 2 PDSA cycles during the study period to evaluate the intervention, and address key challenges identified. Through a review of best practices from published literature and interactive dialogue with CHC representatives, a multi-component, multi-level intervention was developed to promote completion of key steps required to promote colonoscopy follow-up. A patient navigator followed up with participants with an abnormal FIT result. The patient navigator was provided with a weekly list of individuals with an abnormal FIT and asked to use a checklist to ensure completion of key steps in the follow-up process, and to implement specific interventions for any incomplete steps (Table 1). The patient navigator was an employee at Family Health Centers of San Diego with 5 years experience as a care coordinator. In addition to extensive prior navigation training and experience, the navigator received study-specific training on CRC, CRC screening, research ethics, motivational interviewing techniques, and tracking patient data using a pre-formatted Excel spreadsheet and subsequently an EHR-based patient registry of individuals with an abnormal FIT.
Checklist and Interventions to Promote Follow-up Colonoscopy After Abnormal FIT.

Patient navigation activities were conducted through review of EHR data, phone call interactions with patients and clinic staff, and electronic communications with providers. Monitoring completion of each step was facilitated initially by a spreadsheet-based tracking log that measured checklist elements in Table 1, and subsequently by an abnormal FIT registry created within the EHR. Additionally, the navigator recorded narrative details of barriers and challenges to FIT completion using an Excel spreadsheet tracking log.
Results of the initial PDSA cycle were assessed through review of quantitative data and interactive dialogues with the patient navigation and care coordination teams and Family Health Centers of San Diego leaders. Between cycles several changes were made to streamline the process and address challenges. Challenges were identified at the first cycle at data collection, systems, and patient levels. In the first cycle, data on whether the patient navigator had attempted to facilitate colonoscopy completion, and information on missed and cancelled colonoscopy appointments were not available in the EHR. These elements were included in the EHR-based registry of abnormal FIT patients that was created. Additional challenges identified included: delays in results reporting to patients by providers; ability to reach patients with abnormal FIT during regular working hours; only having a single phone number to reach patients. To address these challenges, we modified the initial intervention to standardize the timeframe and delivery of patient results. We also standardized protocols for what to do if patients were not reachable or there was loss to follow-up. For example, the proportion of patients notified of abnormal FIT results within the target period was modified and standardized to 4 weeks. We utilized scripts approved by leadership for the patient navigator to report abnormal results, created a handout given to patients to explain the steps required for colonoscopy completion after an abnormal FIT, and allowed for outgoing calls to be made in the evenings/after normal business hours. System level changes included emphasizing the importance of obtaining an alternate phone number at every visit.
Data Analysis
The primary outcome of interest was the proportion of patients with abnormal FIT completing colonoscopy within 6 months of abnormal test results compared to the pre-intervention completion rate. This was assessed via a chi-squared test of proportions, designating a 2-sided P < .05 as statistically significant. Secondary outcomes of interest included proportion of patients with abnormal FIT completing each of the following steps: colonoscopy referral; pre-colonoscopy specialty visit scheduling; pre-colonoscopy specialty visit completion; colonoscopy scheduling, and colonoscopy completion. The study was approved by the Institutional Review Board Administration of Family Health Centers of San Diego and University of California San Diego.
Results
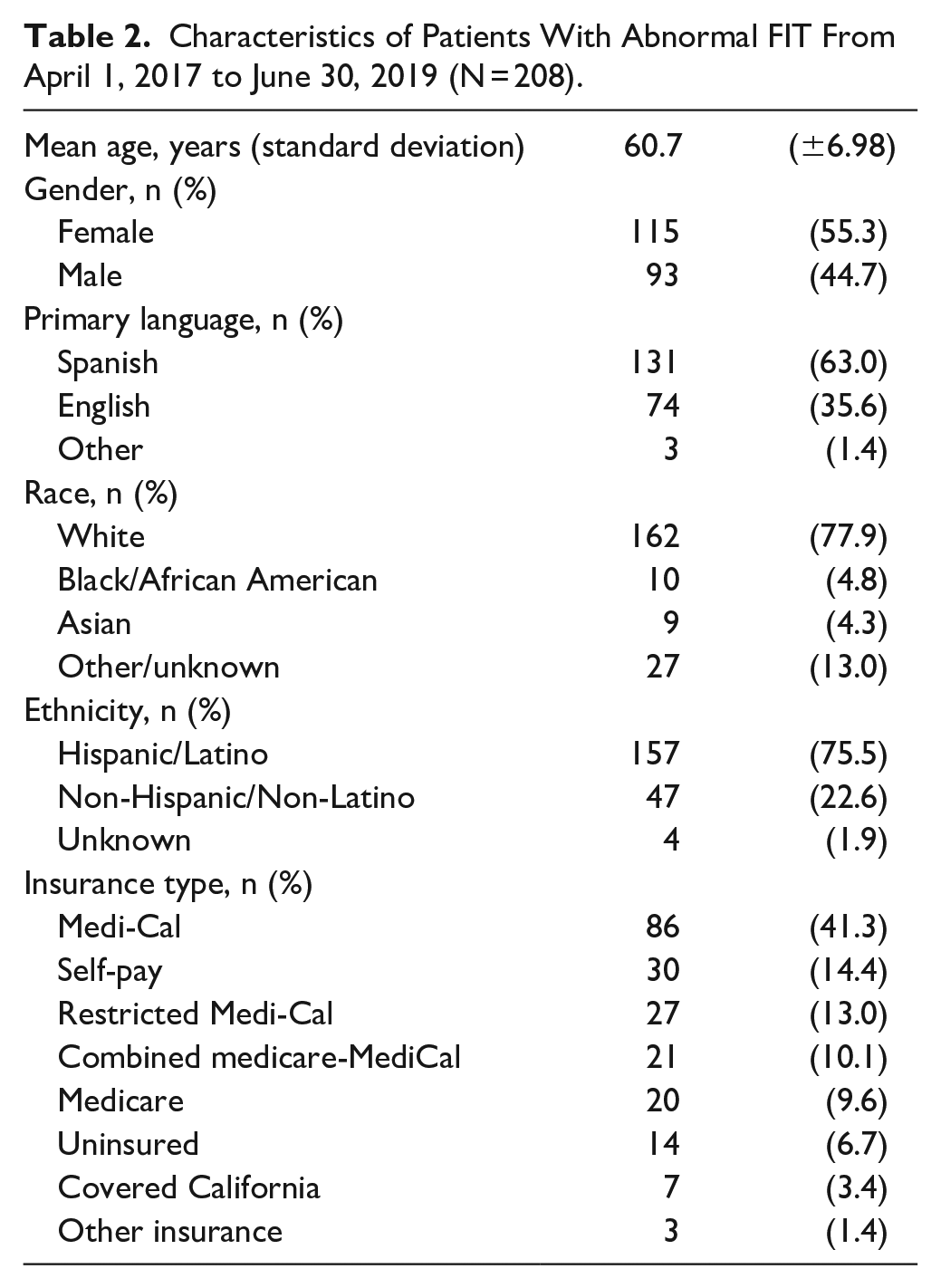
Across the entire intervention observation period April 2nd, 2017, through June 30th, 2019, encompassing the 2 PDSA cycles, we identified 208 individuals with an abnormal FIT. These individuals were age 50 to 75 years and had at least a 6-month follow-up to assess colonoscopy completion. Mean age of patients with an abnormal FIT was 61 years; 55% were women; 63% identified Spanish as their primary language; 76% self-identified as having Hispanic/Latinx; the majority were covered by Medi-Cal insurance; and 9.6% were uninsured (Table 2).
Characteristics of Patients With Abnormal FIT From April 1, 2017 to June 30, 2019 (N = 208).
Among the 208 individuals with abnormal FIT, 95% were referred for colonoscopy (198/208), 50% scheduled a pre-colonoscopy consultation visit (105/208); 49% completed a pre-colonoscopy consultation visit (102/208); 43% scheduled a colonoscopy (90/208); and 38% ultimately completed colonoscopy within 6 months of having an abnormal FIT (78/208; Figure 1). Compared to the previously assessed baseline completion estimate of 21%, this represented a 17% absolute increase in the proportion completing colonoscopy (21% vs 38%, P < .001, 95% CI surrounding difference: 6.9%-25.2%).

Completion of abnormal FIT follow up steps among all patients with an abnormal FIT during the intervention period. Proportion of patients with abnormal FIT completing key steps in the colonoscopy completion process is depicted.
Among the 130 individuals who did not complete colonoscopy, the largest drop in the colonoscopy completion process occurred between referral for colonoscopy and scheduling of a pre-colonoscopy visit, accounting for 71.5% of non- completion (93/130). Lack of referral for colonoscopy (7.7%; 10/130), non-completion of a scheduled pre-colonoscopy visit (2.3%; 3/130), non-completion of colonoscopy scheduling after pre-colonoscopy visit (9.2%; 12/130), and non-completion of colonoscopy after scheduling (9.2%; 12/130) were less frequent reasons for drop offs in the colonoscopy follow-up process following an abnormal FIT (Figure 2). Across all patients with abnormal FIT, reasons documented in navigation logs for non-completion of colonoscopy included: lack of funding; leaving the state or country; report of prior colonoscopy; and refusal without stating a reason. Some patients had more than 1 reason documented, and many had no reason documented, most often because of inability to contact the patient. Specific to the 10 patients who were not referred for colonoscopy by their primary care clinician after abnormal FIT, reasons for non-referral included patient refusal (n = 2); request for repeat FIT with refusal after second result was normal (n = 1); and provider report that patient was already up to date with colonoscopy (n = 7).

Distribution of drop-offs in the abnormal FIT follow up process among colonoscopy non-completers. Among the 130 individuals who did not complete colonoscopy after abnormal FIT, the process step accounting for the largest proportion was failure to schedule a pre-colonoscopy clinic evaluation after referral for a colonoscopy.
Discussion
This quality improvement study applied a PDSA model and patient navigation to increase colonoscopy completion within 6 months after an abnormal FIT in a large, predominantly Hispanic/Latinx servicing CHC system in San Diego County. We observed a 17% absolute increase in the proportion of individuals with an abnormal FIT completing colonoscopy after intervention implementation, from 21% at baseline to 38% across all individuals with abnormal FIT across the intervention observation period. Across critical steps in the abnormal FIT follow-up process, 95% were referred for colonoscopy. Still, significant drop offs were noted after referral, underscoring challenges with pre-colonoscopy visit scheduling, pre-colonoscopy visit completion, and colonoscopy scheduling and completion. Taken together, our results suggest that our approach appeared to increase colonoscopy completion after abnormal FIT, but that multiple challenges to achieving high rates of completion remain.
Our results inform findings from prior studies examining interventions for improving abnormal FIT to colonoscopy completion. With respect to patient navigation for abnormal colorectal cancer screening test follow-up, randomized trial results have been mixed. One systematic review identified 2 adequate randomized trials comparing patient navigation versus usual care and reported a non-statistically significant absolute increase in colonoscopy completion of 14% over usual care (95% CI: 0.2%-29%).17 -19 A recent randomized controlled trial at a large integrated commercial health system found that colonoscopy rates were 76% among navigated patients versus 65% among non-navigated patients (hazard ratio = 1.35, 95% CI: 1.07-1.72). 21 Additionally, a randomized controlled trial of clinician-directed education and audit/feedback on performance has been shown to increase colonoscopy completion after an abnormal stool test. 22 Observational studies suggest patient navigation, 23 including within safety-net populations, 24 structured workflows, 25 as well as a package of system-level strategies within an integrated healthcare system (setting a time goal for colonoscopy completion, establishing a registry, assigning responsibility for follow-up to the GI specialty team, care coordination) 12 can help to improve completion rates. Another centralized navigation program in North Carolina achieved a completion rate of 92% among 26 individuals accepting navigation. 26 Our intervention drew from previously reported promising strategies, including patient navigation from a navigator trained in eliciting and addressing barriers; a checklist that included ensuring providers received reminders when abnormal FIT results were not reviewed or a colonoscopy was not ordered, patients received results and understood importance of follow-up, and that patients received reminders on steps required for colonoscopy completion, including appointment scheduling and bowel preparation. Our study advances knowledge in this area by demonstrating that a combination of interventions that included patient navigation, and a structured checklist to facilitate steps in the follow up colonoscopy process, may substantially increase colonoscopy completion.
The distribution of drop offs in the follow-up process observed in this study may offer insights into the best target points to consider for future interventions. Specifically, we observed that over 70% of drop offs in the colonoscopy follow-up process occurred between the point of colonoscopy referral and the scheduling of a pre-colonoscopy office visit. We postulate that contributors to these drop offs could include lack of patient understanding of the importance of follow-up; transportation challenges; accessibility of specialty gastroenterology offices (including willingness to schedule patients with lower paying insurance such as MediCal)—barriers to scheduling are the subject of ongoing research by our group and others. Notably, in many private practice settings, it is common practice to allow for “direct access” scheduling, where a pre-colonoscopy visit is not required prior to scheduling a colonoscopy test date. Implementing direct access scheduling was part of a colonoscopy screening promotion program in New York City that eliminated racial ethnic disparities in colorectal cancer screening participation. 27 This suggests that building partnerships between CHCs and gastroenterology specialty offices that allow for direct access scheduling might be one strategy for increasing colonoscopy completion after an abnormal FIT.
Reasons for non-completion of colonoscopy were not able to be consistently documented in our patient navigation logs, often because of inability to contact the patient. Reported reasons for non-completion included patient refusal, insufficient funds, report that the patient was already up to date with colonoscopy, and inappropriate management such as repeating a FIT. Future interventions should also address these and other patient-, provider-, and system-related barriers to colonoscopy completion after an abnormal CRC screening test. These include: addressing awareness of results; health literacy; implications of an abnormal test result, insurance challenges such as coverage, authorization, and patient cost sharing; patient fears regarding the procedure and potential results; competing health issues; incorrect management by clinicians (repeating FIT, misattributing an abnormal result to another condition); lack of transportation; lack of social support (including an escort for the procedure); lack of coordination care between primary care and GI specialists; inconsistent workflows for follow up.23,25,28 -32 From a policy standpoint, establishing a quality metric for health insurers and health systems, defined as the proportion of patients with an abnormal non-invasive CRC screening test completing colonoscopy, could help increase appropriate follow up. Such a quality metric is increasingly relevant, as the range of non-invasive stool and blood-based options for CRC screening is expected to increase substantially in the near future. Indeed, the benefits of increased participation in screening promised by non-invasive tests will not result in reduced CRC incidence or mortality without optimizing colonoscopy completion after an abnormal CRC screening test.
Several strengths and limitations may be considered in interpreting our report. The study is one of a few to examine an intervention for increasing abnormal test follow-up in CHCs serving traditionally underserved patients. We also have demonstrated that the package of interventions delivered was feasible to implement. Limitations include the fact that the study had a pre-post intervention design limiting the ability to make causal inferences regarding impact of the interventions described. Accordingly, we recognize the potential that study findings, including improvement in colonoscopy completion, could have been due to unmeasured factors other than the study interventions. Further, we were not able to tease apart which components of our interventions were most important for promoting colonoscopy completion. Further research should specifically explore patient challenges to completion of pre-colonoscopy office visits.
In summary, we found that a quality improvement initiative consisting of patient navigation plus a structured checklist to promote steps required for colonoscopy completion may have the potential to improve abnormal FIT follow-up in a CHC system setting. While colonoscopy completion rates appeared to improve, rates were still suboptimal, largely due to a drop off between colonoscopy referral and pre-colonoscopy specialist visit completion. More patient, provider, system, and policy level strategies are needed to optimize follow-up after abnormal non-invasive CRC screening tests and early detection and prevention of CRC.
Footnotes
Author Contributions
All authors whose names appear on this submission:
(1) made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data; or the creation of new software used in the work; (2) drafted the work or revised it critically for important intellectual content; (3) approved the version to be published; and (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers U54 CA13238406/U54 CA132384 and UG3/ UH3CA233314.