
Abstract
Objective:
Individuals with an abnormal fecal immunochemical test (FIT) result have an elevated risk of colorectal cancer, and the risk increases if the follow-up colonoscopy is delayed. Of note, rates of follow-up colonoscopy are alarmingly low in federally qualified health centers (FQHCs), US health care settings that serve a majority racial and ethnic minority patient population. We assessed factors associated with colonoscopy after an abnormal FIT result and used chart-abstracted data to assess reasons (including process measures) for lack of follow-up as part of an annual, mailed-FIT outreach program within a large, Latino-serving FQHC.
Methods:
As part of the National Institutes of Health-funded PROMPT study, we identified patients with an abnormal FIT result and used logistic regression to assess associations between patient demographics and receipt of follow-up colonoscopy, controlling for patients’ preferred language. We report on time (days) to referral and time to colonoscopy. For charts with an abnormal FIT result but no evidence of colonoscopy, we performed a manual abstraction and obtained the reason for the absence of colonoscopy. When there was no evidence of colonoscopy in a patient’s electronic health record (EHR), we performed an automated query of the administrative claims database to identify colonoscopy outcomes.
Results:
We identified 324 patients with abnormal FIT results from July to October 2018. These patients were mostly publicly insured (Medicaid 53.1%, Medicare 14.5%), 81.8% were aged 50 to 64 years, 55.3% were female, 80.3% were Hispanic/Latino, and 67.3% preferred to speak Spanish. We found that 108/324 (33.3%) patients completed colonoscopy within 12 months, and the median time to colonoscopy was 94 days (IQR: 68-176). Common barriers to colonoscopy completion, obtained from chart-abstracted data, were: no documentation following referral to gastrointestinal (GI) specialist or GI consultation (41.6%), no referral to GI specialist following abnormal fecal test (34.2%), and absence of a valid insurance authorization (6.5%).
Conclusions:
Multi-level strategies are needed to provide optimal care across the cancer continuum for FQHC patients. In order to reduce the risk of CRC and realize the return on fecal testing investment, concerted system-level efforts are urgently needed to improve rates of follow-up colonoscopy among FQHC patients and redress racial and ethnic disparities in CRC screening outcomes.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common cancer and the second leading cause of cancer death for men and women in the United States. 1 For individuals aged 50 and over, 2020 projections included 130 020 colorectum cancer cases and 49 560 deaths. 2 Due to increased screening, CRC incidence and mortality have declined considerably over the past 4 decades in the United States; however, many of those eligible are still not screened.3,4 National data from 2018 show that nearly 70% of eligible adults are up to date with screening recommendations, but screening rates remain low for uninsured individuals (24.8%), those covered by Medicaid (47%), and members of racial/ethnic subgroups (49.9%, Latinos; 54.3%, American Indians; and 61.8%, African Americans). 5 Federally qualified health centers (FQHCs) are the largest provider of care to under- and uninsured groups in the US and serve a majority racial and ethnic minority patient population, thus are well positioned to deliver recommended cancer screening and support for adherence to follow-up services in populations with disproportionately low CRC screening rates.6-10 There are no national guidelines for time to follow-up colonoscopy (after an abnormal fecal screening test); however, the National Cancer Institute-funded Population-Based Research Optimizing Screening Through Personalized Regimens (PROSPR) Consortium tracks follow-up at 90 days, while other health systems report 60 day follow-up rates. 11
Follow-up colonoscopy proportions range from 18% to 57%—among the lowest in US health care settings6,12-16 and far below national targets. 17 This is due in part to the challenges FQHCs face in coordinating care with colonoscopy providers outside of their system, in contrast to health systems with integrated specialty care services. Such challenges include colonoscopy appointment scheduling and the transfer of patient information and colonoscopy reports. 13 FQHCs must complete several steps, including placing a referral to a gastrointestinal (GI) specialist, obtaining its approval, and communicating this approval to the patient along with the name of a specialist (selected from a list of contracted physicians) sited nearest the patient’s home address. Patient-level barriers include lack of knowledge about the need for colonoscopy, difficulty arranging transportation to and from the procedure, and fear of discomfort.18-21 Moreover, patients may lack health care coverage and face financial barriers to care.22,23
As part of the Participatory Research to Advance Colon Cancer Prevention (PROMPT) study, we sought to explore follow-up colonoscopy patterns among FQHC patients who participated in an annual mailed fecal immunochemical test (FIT) outreach program and whose test results were abnormal. We report patient characteristics associated with colonoscopy completion and the reason a colonoscopy (including process measures) was not completed.7,24,25 We validated electronic health record (EHR) data on colonoscopy receipt using International Classification of Diseases (ICD) codes by comparing it with data obtained from both manual chart abstractions and an administrative database. Prior efforts to explore the lack of a follow-up colonoscopy in community clinic settings have not included EHR review in combination with claims data query; thus, our report represents status of CRC screening in 1 FQHC contracting with multiple GI specialists.12-14 Within a majority Latino-serving FQHC setting, we report unique follow up colonoscopy information for a population disproportionately represented in poor CRC screening outcomes. We identify key process and system-level factors to be improved with the potential to redress racial and ethnic screening disparities in this and other FQHCs around the nation. 26
Our team previously reported a chart abstraction-verified 43% follow-up colonoscopy completion rate in a large FQHC headquartered in Seattle. 27 However, data for the analysis did not incorporate Medicaid claims, which represents a reliable source of data on colonoscopy completion. Here, we report chart abstraction- and Medicaid claims-verified data on follow-up colonoscopy receipt from the largest independent FQHC in the US, which serves a patient population that is 83% Latino—44% of which is best served in a language other than English. 28
Methods
A detailed description of the PROMPT study has been published previously. 7 In brief, PROMPT was a pragmatic, stepped-wedge effectiveness-implementation study that tested enhanced prompts and reminders about a centralized mailed-FIT outreach program in 15 clinics operated by a nonprofit FQHC serving more than 210 000 predominantly Latino patients in California. 7
The FQHC implemented an annual mailed-FIT program in summer 2015, using EHR data to identify age-eligible, average-risk adults not up to date for CRC screening. The FQHC’s CRC screening rate was 63% in 2018, 56% in 2019, and 43% in 2020. Program materials were created in English and Spanish. The FQHC contracts with a vendor to send FIT kits (Insure, Clinical Genomics [Bridgewater, NJ]) to patients’ home addresses. As part of the PROMPT trial, the 2018 and 2019 program included a “primer” text message or live call to patients 2 weeks before the FIT mailing, with the text message being sent the day before the live-call period finished. The mailing included (1) an introductory personalized letter from the patients’ care team, including messaging about the importance of family in completing CRC screening,7,25 and (2) the FIT kit, wordless FIT instructions, and a postage-paid return envelope. 25 The mailing was followed by 2 automated calls (the first call occurred a little less than a week after the patient received the FIT and the second call was about 1.5 week after the first), and 2 weeks after that by live reminder calls delivered at the discretion of each clinic by a member of the care team (usually a medical assistant). 24 The ordering provider/primary care provider (PCP) communicated abnormal FIT results to patients via phone or an in-person clinical encounter and submitted a referral for a consult with a GI specialist. To generate the referral, the provider entered an order for an office visit with the GI specialist indicating the abnormal FIT result as justification for the referral. A clinic-level referral coordinator entered the referral into a portal that automatically obtains authorization for the procedure from patients’ insurance. For patients enrolled in Medicaid, a follow-up colonoscopy is provided free with out-of-pocket costs. During this study, these costs to patients with commercial insurance or Medicaid could vary; however, recently policy was changed to eliminate these costs irrespective of insurance type.29,30 For uninsured patients, a referral was generated, printed, and given to the patient, but not entered into the referral portal. All patients were instructed to call the specialist’s office and schedule their GI consultation. Typically, at the GI consultation, the GI specialist reviewed the patient’s medical history, confirmed their clinical eligibility for the colonoscopy procedure, and instructed the patient on the bowel preparation needed for the procedure. The GI practice then generated a referral for the colonoscopy procedure and scheduled the colonoscopy.
Measures
We obtained 2018 mailed FIT results through programmer query of the FQHC’s Healthcare Effectiveness Data and Information Set (HEDIS®) database while patient characteristics (age, gender, race, ethnicity, preferred language, and insurance type), referral to GI, and colonoscopy completion date were obtained through programmer query of the FQHC’s EHR (Figure 1; Supplemental Table 1). 31 This information included normal or abnormal result and result date from the 7/2/2018 to 10/16/2018 centralized mailing, as well as clinic-based mailing and handing of FIT kits to patients because the EHR did not distinguish how kits got to patients. Alternative procedures satisfying HEDIS criteria for CRC screening completion, such as computed tomographic-colonography, were also included. Our outcome measures were colonoscopy referral rates (3, 6, and 12 months after abnormal FIT result); colonoscopy completion rates (3, 6, and 12 months after FIT return date); and time to colonoscopy completion. The full term of the lookback period was up to 34 months. For the subset of patients with an abnormal FIT result but no colonoscopy, we performed a manual chart abstraction and gathered information on colonoscopy referral, colonoscopy procedure, pathology findings (eg, presence of adenoma), and cancer (Supplemental Figure 1). To describe the reason for no follow up colonoscopy documented in the chart, we categorized chart abstraction findings into: no documentation following referral to GI or GI consultation, no referral to GI following abnormal fecal test, problem with referral, completed colonoscopy within 10 years of abnormal fecal test, patient not found, recent prior colonoscopy, given second FIT, deceased, patient declined, unable to be notified, no-show, patient is a poor candidate, inadequate prep or tolerance, or GI visit canceled. Manual chart abstraction took place between September 2020 and May 2021.

Data query flow including colonoscopy completion >12 months after abnormal FIT from July 2018 centralized mailing in an urban FQHC. Data sources are depicted. The claims data query was conducted on a subset of member patients (n = 125) that were still members at the time of the query (July & August 2021).
Last, we performed an automated query of the administrative database for the subset of patients (ie, managed care program enrollees) to find evidence for additional colonoscopies not identified through prior methods (Supplemental Table 2).
Analysis
Patient demographic summary statistics were generated in Stata 16.0 (College Station, TX). We used logistic regression to assess the association between patient demographics and receipt of follow-up colonoscopy, controlling for patients’ preferred language. We report odds ratios and 95% confidence interval from logistic regression models.
Results
FIT kits (n = 11 599) were mailed to patients due for CRC screening in July 2018; of the 4638 tests returned, 7.0% (n = 324) had abnormal results at 12 months (Supplemental Table 3). Patients (n = 11 599) were mostly publicly insured (Medicaid 53%, Medicare 12%), 82% were aged 50 to 64 years, 55% were female, 80% were Hispanic/Latino, and 63% preferred speaking Spanish. A majority of the patients with abnormal FIT results were female, aged 50 to 64 years, Latino, covered via Medicaid and Spanish-speaking, and had previously completed CRC screening (Table 1). Of those with an abnormal FIT result, the majority (80.9%) received a referral to a GI specialist for a follow-up colonoscopy; however, the automated EHR query revealed that only one-quarter (28.7%) completed a colonoscopy within 12 months, leaving 231 patients with an abnormal FIT result and no colonoscopy.
Patient Demographics for Those with an Abnormal Fecal Immunochemical Test (FIT) Result.
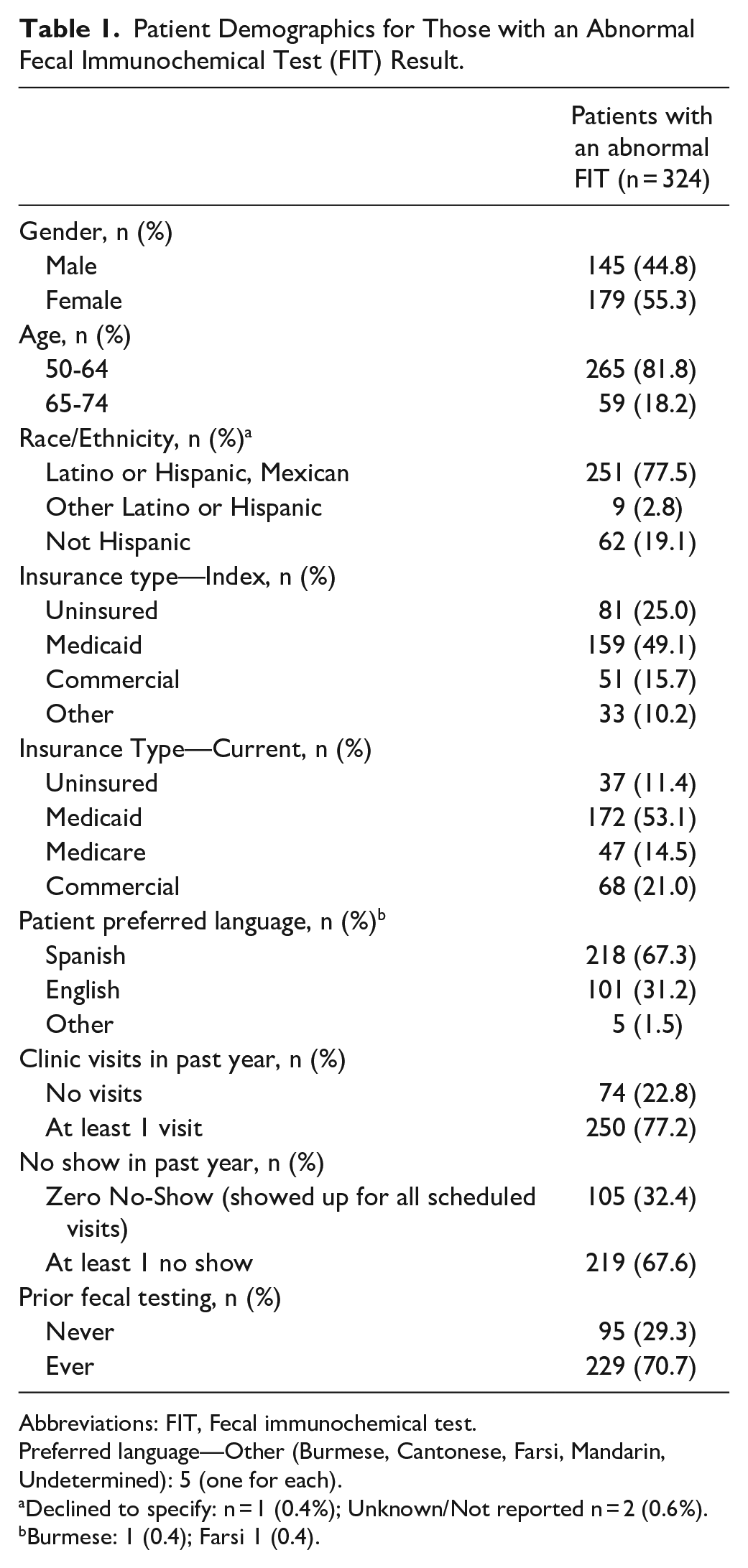
Abbreviations: FIT, Fecal immunochemical test.
Preferred language—Other (Burmese, Cantonese, Farsi, Mandarin, Undetermined): 5 (one for each).
Declined to specify: n = 1 (0.4%); Unknown/Not reported n = 2 (0.6%).
Burmese: 1 (0.4); Farsi 1 (0.4).
When we compared colonoscopy-receipt information obtained from manual chart abstraction and programmer query (n = 93) for the 231 patients with abnormal FIT but no colonoscopy, we identified 6 additional colonoscopies during chart abstraction (Figure 1). Following the automated query of administrative (Medicaid claims) data for the member patient subpopulation (n = 125), 23 additional colonoscopies were identified. Data from these 3 sources revealed that 108/324 (33.3%) patients completed colonoscopy within 12 months while 122/324 (37.7%) patients completed colonoscopy >12 months. Among these, 87% of colonoscopies were completed within 6 months (Figure 2). Among those who obtained a colonoscopy, the median time to the procedure was 94 days (IQR: 64-143).

Referral and abnormal fecal test time to colonoscopy completion within 12 months for patients (n = 108 of 324 with an abnormal fecal test result) with colonoscopy date identified through electronic health record programmer query, manual chart abstraction, and programmer query of administrative data.
After adjusting for preferred language, the odds of females completing a colonoscopy within 1 year of a positive fecal test result were 1.82 times those of males. Patients with a prior fecal testing history had odds of completing a colonoscopy that were 1.69 times higher than those without a prior FIT. Insurance coverage was associated with increased odds of completing a colonoscopy, although the effect appears larger for those covered by Medicaid. Compared with those who did not have insurance, those with Medicaid had odds of completing a colonoscopy that were 6.58 times higher and those with commercial insurance had odds of completing a colonoscopy that were 4.10 times higher (Table 2). Of note, patients 65 to 74 years old had odds of completing a colonoscopy within 1 year of an abnormal FIT result that were 0.80 times those of patients aged 50 to 64 years.
Predictors of Colonoscopy Completion within 1 year after Positive Fecal Test Result (n = 324) by Patient Characteristics (Adjusted for Preferred Language).

Based on the findings from the chart abstraction, the 2 most common barriers to colonoscopy completion observed in the EHR were no documentation following referral to GI or GI consultation (41.6%) and no referral to GI specialist following an abnormal fecal test (34.2%; Table 3). The absence of valid insurance authorization was noted in 6.5% of charts due to a problem with referral: pending referral from insurance change/expiration, a request for new GI, or multiple referrals. Of the 10 cases in which patients self-reported colonoscopy completion (4.3%; not picked up through the automated query), only 6 of 10 patient charts included a report validating the colonoscopy procedure logged by staff.
Colonoscopy Non-Completion Reason Obtained Through Manual Chart Abstraction for Community Health Center Patients with an Abnormal Fecal Test Result (n = 231).
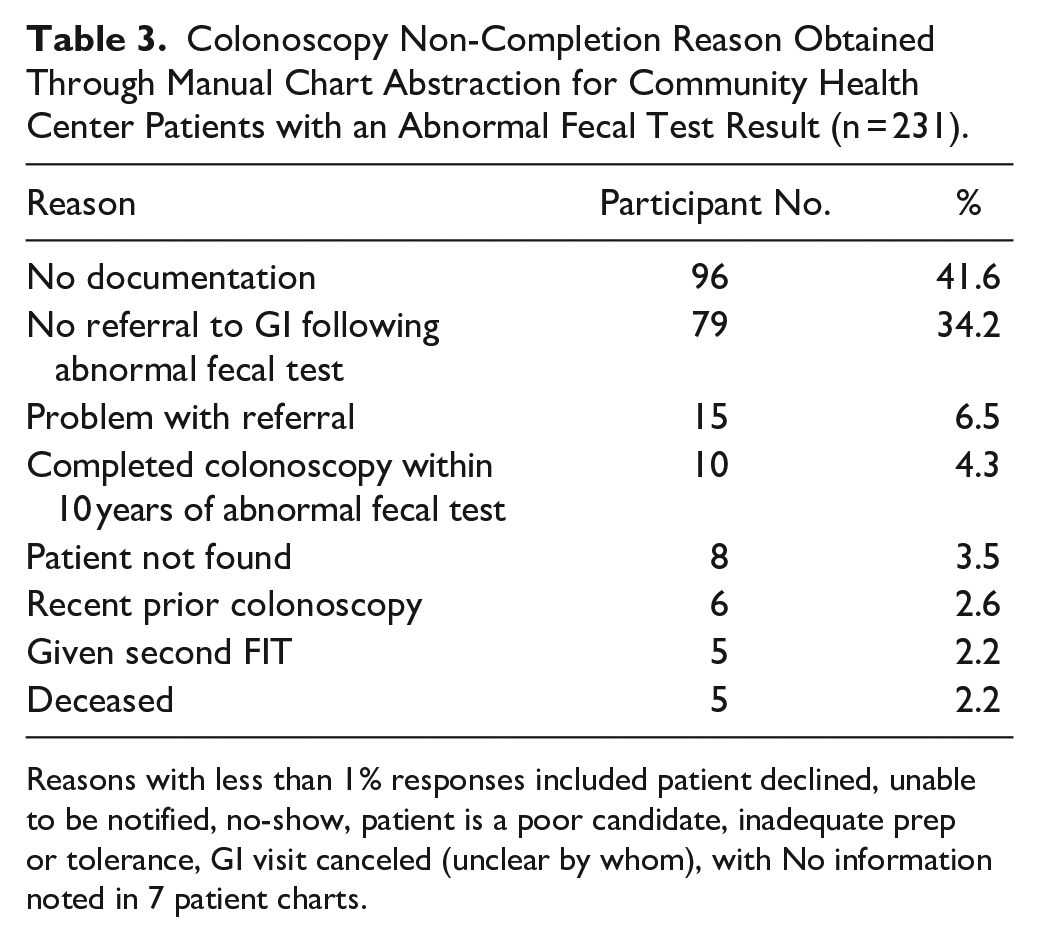
Reasons with less than 1% responses included patient declined, unable to be notified, no-show, patient is a poor candidate, inadequate prep or tolerance, GI visit canceled (unclear by whom), with No information noted in 7 patient charts.
Discussion
Our manual chart-abstraction finding that one-third of charts had no evidence of a referral to GI after abnormal fecal result and that 42% of charts had no indication of an outcome following referral to GI or GI consultation aligns with a San Francisco-based chart abstraction study conducted in a similar community clinic setting. These findings suggest that system-level administrative steps taken by clinic and other staff may be inconsistently documented in the FQHC’s EHR.12,14 In the San Francisco study, when chart abstraction was completed for a sample of 100 patients with an abnormal FIT result who were never referred to GI, 49% had no documentation of counseling about the recommended follow-up. Furthermore, 62% of those who were referred but missed their appointment lacked documentation regarding the abnormal result or their increased CRC risk. 14 Of note, Issaka et al is the only other report describing a high proportion of no documentation and is within a community- and hospital-based primary care clinic system with integrated GI office; thus no other groups have previously reported such a profound lack of documentation in the chart of patients with an abnormal result but no follow-up colonoscopy. In the studies where chart abstraction was conducted to identify the reason for no colonoscopy only 2 of 4 were in FQHCs with a lower proportion of Latino patients (15% and 37%).27,32 Moreover, diverging from the current study where the most common explanation for lack of colonoscopy was system-level factors, earlier reports indicate patient-level factors (declination or appointment no-show 19%-57%) and provider inability to reach patients among the most common reasons for lack of follow-up colonoscopy.14,27,32,33 Taken together, these findings suggest that FQHC clinical workflows bridging primary care and GI specialists as well as the information technology (IT) infrastructure undergirding them are underdeveloped and fall into a “provider ownership gap.” 14 As 1 possible explanation for this lack of documentation, during the study period, the FQHC migrated to a new EHR, which likely impacted standardized processes regarding abnormal FIT results. The absence of a referral to GI specialist or indication of outcomes following a referral underscores the need to ensure that EHR documentation is routinely taking place and must be given additional consideration through dedicated resources in order to complete the CRC screening continuum. Proposed interventions include reliance on patient navigators, provider reminders and/or performance data reports, automated referrals to a GI, and multicomponent quality-improvement efforts. 34 Once these clinical workflows, IT infrastructure (including reminders and/or notifications), and teams are in place, staff training might be needed that emphasizes the risk of late cancer detection among patients for whom the screening continuum of care is interrupted.35-37 Policy approaches including addition of a health system- and insurer-required quality metric capturing colonoscopy completion after abnormal fecal test represent additional areas in which to boost screening completion. 12
Inappropriate CRC screening has been reported in prior studies and was observed in the current study. While Issaka et al 14 report 10% of patients completed FIT in error (ie, returned second FIT after the initial 1 with an abnormal result) and FQHCs report 4% of patients given a second FIT, we observed 2% of patients completed a second FIT.27,32 This overutilization of screening tests in an already strained safety-net system wastes scarce resources and conflicts with medical guidelines, both of which threaten care quality. 37 Integrating prior lab results into panel management and outreach to proactively, accurately screen patients represents 1 EHR strategy to address inappropriate screening and incomplete follow-up.
Manual chart abstraction in addition to an automated query of administrative claims data resulted in a 4%-point increase in follow-up colonoscopy completion <12 months following an abnormal FIT result (29% vs 33%) compared with an automated EHR query alone. We observed a larger increase when colonoscopies completed >12 months were included (29% vs 38%). Moreover, we found that female, insured, and Spanish-speaking patients, as well as those with at least 1 medical visit or who had obtained prior CRC screening, were more likely to complete the recommended colonoscopy.
We observed a 33% colonoscopy completion rate within 12 months comparable to that reported in 6 prior studies conducted since 2017. These prior reports found 1 year follow-up colonoscopy rates of 18% to 56%.12,14,16,27,32,33 Patients in these studies, similar to those in the current study, were referred to 1 of several contracted GI specialists complicating successful colonoscopy completion—with the exception of Issaka et al 14 and Martin et al 33 ,where patients were referred to a single network hospital.
We observed 94 days median time from abnormal FIT to follow-up colonoscopy, which was comparable to data in 5 prior reports conducted since 2017 (range: 72-300 days).14,16,27,32,33 Moreover 14 colonoscopies were completed >12 months. Our observed time to colonoscopy fell just outside the 90 day benchmark set by the PROSPR initiative, suggesting that additional strategies may be needed to support FQHC patients in successfully accessing GI services in a timely manner. 11
Additional supports are needed for male patients, older patients, and those who lack health insurance or who have disengaged from clinical care. These health disparities have been previously reported and underscore the importance of tailoring educational materials and clinical workflows to address these hard to reach patients for which reminders and prompts may be insufficient and where intensive interventions addressing overlapping complex medical conditions and social needs may be warranted.13,14,27,32,38,39 These findings fall within the broader context of health disparities whereby Latino adults have considerably lower CRC-screening uptake than their non-Latino White counterparts (56% vs 71%), which is concerning given that as few as 18% of FQHC patients with an abnormal screening result complete the recommended follow-up colonoscopy within 12 months. Here, too, disparities are reported: follow-up colonoscopy rates are substantially lower among Latino than non-Latino White patients.14,32,33,40
Given that 1-in-11 to 1-in-28 people with an abnormal fecal test result has CRC, urgent action is needed to catch potential cancers earlier in their progression.12,35,36 This situation, all too common in underserved community clinic-populations with under- and uninsured patients, often culminates in later-stage cancer diagnoses. Within the FQHC setting, specialty care occurs outside of primary care, and these systems are rarely interoperable, requiring proactive, systematic efforts to exchange patient information and colonoscopy findings including screening interval. 12
This interruption in the continuum of care among FQHC patients is particularly alarming given that access to GI visits has been restricted because of the COVID-19 pandemic.41-46 Community clinics report a 5% point decrease—from 45% in 2019 to 40% in 2020—in CRC screening rates. 41 The pandemic-related backlog, combined with recent changes to US Preventive Services Task Force guidelines recommending initiation of screening at age 45 rather than age 50 (impacting roughly 20 million adults aged 45-49), has increased demand for screening and follow-up services at a time when community clinics are struggling with colonoscopy backlog for those aged 50 and older.37,43
Strengths and limitations
The strengths of this study include our large retrospective sample from a non-integrated FQHC, health record abstraction of 231 patients with abnormal FIT, and query of the claims database for those without evidence of follow-up colonoscopy in the EHR. Nevertheless, our study has several limitations. While we relied on programmer queries, manual chart abstraction, and claims data queries, it is likely that not all records of completed colonoscopies were in the EHR; thus, our colonoscopy completion results may underestimate true rates. Although codes for the GI pre-consult were queried, we were unable to identify any of these intermediary steps in the EHR or the claims database, so we likely underreport this intermediary step. We did not include variables such as underlying diseases. Moreover, reasons for non-completion recorded in the EHR are likely incomplete.21,38,47 Finally, our findings are from a single, large FQHC and may not be generalizable to other settings.
Conclusions
Despite widely reported positive health outcomes, rates of follow-up colonoscopy for individuals with abnormal FIT results who receive care in FQHCs remain far below the 80% target. 17 In order to reduce the risk of CRC and realize the return on fecal testing investment, concerted efforts are urgently needed to redress racial and ethnic disparities in rates of follow-up colonoscopy among FQHC patients. They must include system-level strategies such as relevant EHR infrastructure (ie, report repositories, reminders, and notifications) and staff training on utilizing these IT resources; staff dedicated to patients’ transition from primary to specialty GI care; and novel outreach approaches.39,48 Investing in system-wide cancer screening resources may be integral to redressing racial and ethnic prevention inequities.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221138423 – Supplemental material for Colonoscopy Following an Abnormal Fecal Test Result from an Annual Colorectal Cancer Screening Program in a Federally Qualified Health Center
Supplemental material, sj-docx-1-jpc-10.1177_21501319221138423 for Colonoscopy Following an Abnormal Fecal Test Result from an Annual Colorectal Cancer Screening Program in a Federally Qualified Health Center by Anne L. Escaron, Joanna Garcia, Amanda F. Petrik, Esmeralda Ruiz, Denis B. Nyongesa, Jamie H. Thompson and Gloria D. Coronado in Journal of Primary Care & Community Health
Supplemental Material
sj-xlsx-2-jpc-10.1177_21501319221138423 – Supplemental material for Colonoscopy Following an Abnormal Fecal Test Result from an Annual Colorectal Cancer Screening Program in a Federally Qualified Health Center
Supplemental material, sj-xlsx-2-jpc-10.1177_21501319221138423 for Colonoscopy Following an Abnormal Fecal Test Result from an Annual Colorectal Cancer Screening Program in a Federally Qualified Health Center by Anne L. Escaron, Joanna Garcia, Amanda F. Petrik, Esmeralda Ruiz, Denis B. Nyongesa, Jamie H. Thompson and Gloria D. Coronado in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number 3U01MD010665-05S1. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Data may be accessed through communication with the first author.
Ethical Statement
The study was reviewed and approved by the Kaiser Permanente Northwest Institutional Review Board (IRB), with ceding agreements from the FQHC. The IRB provided a waiver of consent given minimal risk to patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.