
Abstract
Introduction/Objectives:
Companion animals (CAs) may benefit human health, but few studies have examined their impact on stroke survivors. This study examines participation, quality of life (QoL), attachment, cognition, and executive function differences between stroke survivors living with and without CAs.
Methods:
In this cross-sectional, community-setting study, 25 stroke survivors with a CA and a matched group of 27 without a CA completed standard tools.
Results:
Stroke survivors with a CA scored significantly higher in participation and 1 cognitive performance test. No significant differences were found in other cognitive measures or QoL, and attachment to a CA was not correlated with participation or QoL within the research group. However, lower attachment avoidance correlated with better participation in survivors living with dogs.
Conclusion:
Living with CAs, especially dogs, might be associated with some cognitive function and participation benefits among stroke survivors. The link between CAs and cognitive function is unclear: Survivors with higher cognitive functioning might be more capable of caring for a CA, or having and caring for a CA might promote better cognitive function. Attachment patterns also might explain stroke survivors’ participation levels. Further study is warranted.
Introduction
Stroke is a significant public health concern characterized by various functional limitations, including motor, sensory, and cognitive limitations affecting various daily functional tasks (eg, the ability to independently dress, eat, walk, or work). 1 Investigating factors that might mitigate long-term disability by promoting participation and quality of life (QoL) among stroke survivors is essential, especially in their natural environment and daily routines. 2 One key aspect affecting functional disabilities in stroke is cognitive deficits, 3 especially impaired executive functions (EF). Critical for independent performance, EF are vital to assess in people with stroke returning to their premorbid activity in the participation. 4
Many older adults in the Western world live with a companion animal (CA), such as a dog, cat, bird, or small mammal, 5 and therapists have shown interest in involving animals in therapeutic processes. 6 However, few studies have addressed the benefits of CAs for stroke survivors. Johansson et al 7 examined the effects of living with a CA on the physical, psychological, and social aspects of stroke recovery. They identified a general theme with 4 categories: motivation for physical and psychosocial recovery, someone to care for who cares for you, animals as family members, and providers of safety and protection. They concluded that stroke survivors experience CAs as contributing to their physical and psychosocial health and meaningful life.
Possibly, these results stem from occupations involved in caring for a CA, classified as instrumental activities of daily living (IADL). 8 These occupations provide personal and social significance and require performing multiple activities 9 to arrange and care for the animal. The IADL often include interactions among complex activities within various environments, with EF as a key element. 10 Thus, caring for a CA may promote cognition, EF, and participation.
Despite the common belief that living with a CA improves human health and well-being, 11 scientific evidence of this “pet effect” concept is not well established. 12 Individual differences in attachment style may explain the contradictory evidence. 13 Attachment theory observes these differences 14 and promotes an understanding of the relationship’s nature. Zilcha-Mano et al 15 demonstrated that CAs can be attachment figures, as in human attachments. In a human–animal attachment bond, the animal provides a “sense of safe haven in times of need and a secure base for exploration.” 16 (p. 571). Zilcha-Mano et al 16 showed that individual differences in CA attachment predict the owner’s benefits from the relationship.
Because no previous studies have been conducted with diagnostic samples, there remains a need to investigate the impact of human–animal relationships in clinical populations. This study aimed to examine differences in participation, QoL, CA attachment, cognition, and EF between stroke survivors living with and without CAs to address this gap and its possible mechanisms. We hypothesized that significant between-group differences would be found in the measures of participation, QoL, cognition, and EF and that CA attachment would correlate with participation and QoL for stroke survivors living with animals. Information from this study bears theoretical and clinical potential for understanding CAs’ contributions to stroke survivors’ rehabilitation.
Methods
The Faculty of Welfare and Health Sciences, University of Haifa, Ethical Committee (005/15) and the “HaEmek”, Medical Institute Human Rights Helsinki Committee (0018-14) provided ethical approval for this community-based, cross-sectional study with matched controls. Participants signed informed consent, and trained occupational therapists administrated 2-h assessments in participants’ homes.
Participants were recruited through a stroke community association. No incentives were offered, and there was no relationship between the researchers and the participants. Inclusion criteria for the research and control groups were aged 50 years or older, at least 6 months post-stroke, living in the community, able to write and read, and a Montreal Cognitive Assessment (MoCA) 17 score of ≥19. Although the MoCA cutoff for normal cognitive function is 26, we used 19 to include a broader range of stroke survivors, among whom cognitive disabilities are common. 18 Half of the participants (research group) lived with CAs at home. Exclusion criteria were other central nervous system disorders or addiction to drugs/alcohol. Participants who could or would not provide informed consent were excluded.
A demographic questionnaire obtained personal data, stroke characteristics, and (research group only) data regarding the CA.
The Activity Card Sort (ACS) recovering version 19 is a reliable, valid measure comprising labeled photographs of adults participating in categories of real-life activities: IADL (eg, cooking meals), social-cultural (eg, visiting family), and low- (eg, reading books) and high-demand (eg, walking) leisure. The version for this study consisted of 88 pictures in culturally relevant settings. 20 For each activity card, respondents indicate their status since stroke onset as doing now (1), doing less (0.5), or gave up (0). Scores are the sum of the current and previous activity and a percentage of the current activity level. The ACS total score represents the participant’s current activity score divided by the previous (retained) activity score. Higher scores indicate that the respondents returned to higher participation levels than before stroke onset.
The World Health Organization QoL Questionnaire 21 is a reliable, valid measure containing 26 items scored for 4 QoL-related domains—physical health, psychological health, social relationships, and environment—and 1 component on overall QoL and general health. The participant scores each item from 1 (not at all) to 5 (absolutely). Higher scores indicate better QoL levels. In our study, the internal reliability range was α = .67 to .86. The overall QoL score represented QoL in this study.
The Color Trail Test (CTT) is a reliable, valid measure assessing visual attention, graphomotor sequencing, and effortful executive processing abilities (ability to alternate between 2 colors). 22 In CTT1, the participant follows a numeric sequence; in CTT2, they divide their attention and simultaneously follow the alternating color and number sequence. Lower completion times for each task represents better performance.
The Kettle Test is a reliable, valid brief performance-based measure that assists in clinical decision-making about daily living skills assistance for adults with suspected cognitive disabilities. 23 It assesses basic and higher-level cognitive processes based on a complex everyday task (IADL) in a clinical setting or at home. The task involves preparing 2 hot beverages that differ by 2 ingredients (an additional load on working memory). The test challenges problem-solving skills using familiar objects and settings, targeting cognitive skills underlying complex ADLs. The rater scores the degree of cueing for step completion (0-4) on each of the task’s 13 steps. Higher total scores (0-52) indicate the need for more assistance.
The Pet Attachment Questionnaire (PAQ) is a reliable, valid, 26-item self-report identifying individual differences in attachment orientation toward a pet. 15 It includes 2 subscales of attachment insecurity in human–pet relationships: Avoidance considers how much people feel discomfort with physical and emotional closeness with, and strive to maintain emotional distance from, their pets. Anxiety considers how much people have intense, intrusive worries that something bad might happen to their pet, a strong desire for closeness with the pet, or seriously doubt their value in their pets’ eyes. Participants rate the extent to which each item describes their feelings about their current pet from 1 (not at all) to 7 (very much). Higher scores indicate higher attachment anxiety or avoidance. Only stroke survivors with CAs completed the PAQ.
Data analysis
Data were analyzed with IBM SPSS (Version 27). Descriptive statistics described participants’ demographics and outcome measures. Group differences were examined using chi-square (χ2) tests for nominal variables (gender, years of education, socioeconomic status, side of brain injury) and t-tests for continuous variables (age). Mann-Whitney tests examined variables with abnormal distribution (time since injury), and Pearson tests examined correlations between attachment measures and participation/QoL in the research group. Post hoc analyses included comparing stroke survivors living with dogs (n = 15) to other CAs (n = 10) relative to total scores. Results were considered significant with P < .05.
Results
We screened 120 potential participants: 13 did not provide consent, 2 died before the study, 40 did not meet inclusion criteria (age/time since stroke), and 13 had MoCA scores under the cutoff. Figure 1 shows that we enrolled 52 stroke survivors: 25 in the research group (with CAs) and 27 in the control group (without CAs).

Participant enrollment flow diagram.
Table 1 describes the sample’s demographic and descriptive characteristics. On average, participants were 68.60 years old (SD = 7.66) and had experienced right hemisphere (61.5%) ischemic (75%) stroke. Most (64%) research group participants lived with only 1 CA.
Participants’ Characteristics.

Abbreviation: MoCA, Montreal Cognitive Assessment.
N = 44.
The study groups were matched by mean age, gender, socioeconomics, brain injury hemisphere, and time-since-injury variables. We followed these demographic-medical variables during recruitment to verify the matching.
Per post hoc power analyses, a sample size of 52, a 2-tailed t-test, and alpha at .05 provided 42% power to detect a medium (d = 0.50) and 81% power to detect a large (d = 0.80) effect size.
Based on data showing that living with dogs requires higher physical activity levels, 24 we divided the research group into stroke survivors living with dogs (n = 15) and living with any other CA (n = 10). A Pearson chi-square test to determine significant differences between those groups found none in gender, χ2(1, n = 25) = 1.42, P = .23; education, χ2(1, n = 25) = 2.68, P = .10; socioeconomic status, χ2(2, n = 25) = 1.45, P = .4; or side of stroke χ2(2, n = 25) = 2.78, P = .25. T tests showed no significant differences in age (t(23) = 1.67, P = .11).
However, a t test revealed a significant between-group difference in participation levels per the ACS total score (t(50) = 2.58, P = .013, d = 0.72). Stroke survivors living with CAs had higher participation levels than their matched controls without CAs. Table 2 shows that no differences were found between research groups in the total QOL score (P = .79).
Participation and Quality of Life Score Statistics.
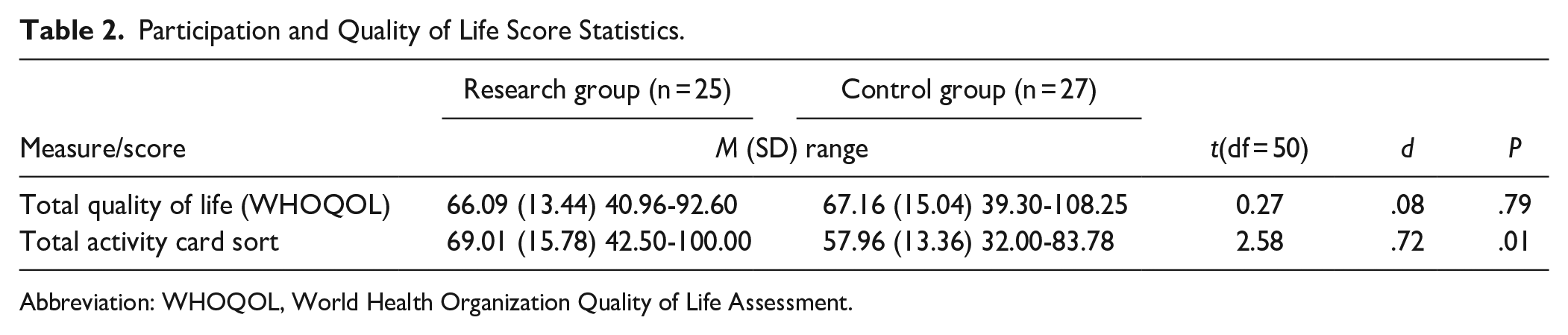
Abbreviation: WHOQOL, World Health Organization Quality of Life Assessment.
Another t test for differences between CA types within the research group showed a significant difference in participation levels per the ACS total score (t(23) = 2.12, P = .04, d = 0.89). Stroke survivors with dogs (M = 74.23, SD = 16.69) had higher participation levels than those with other CAs (M = 61.18, SD = 10.83).
A t test showed no significant between-group differences in the general QoL score (t(50) = 0.27, P = .79, d = 0.08), meaning stroke survivors with or without CAs had similar QoL levels (Table 2). However, a t test comparing by animal type showed a significant within-group difference in the general QoL score (t(23) = 2.53, P = .02, d = 1.03). Stroke survivors with dogs (M = 71.11, SD = 11.93) had higher QoL than stroke survivors with other CAs (M = 58.56, SD = 12.47).
The Mann-Whitney test revealed a significant between-group difference in participants’ CTT1 performance. Table 3 shows that stroke survivors with CAs performed significantly faster (Z = −2.27, P = .02, r = −.45) than those without CAs. No significant between-group differences were found in CTT2 performance (Z = −1.69, P = .09) or the Kettle Test final score (Z = −1.08, P = .28).
Cognitive Test Statistics: Between-Group Differences.
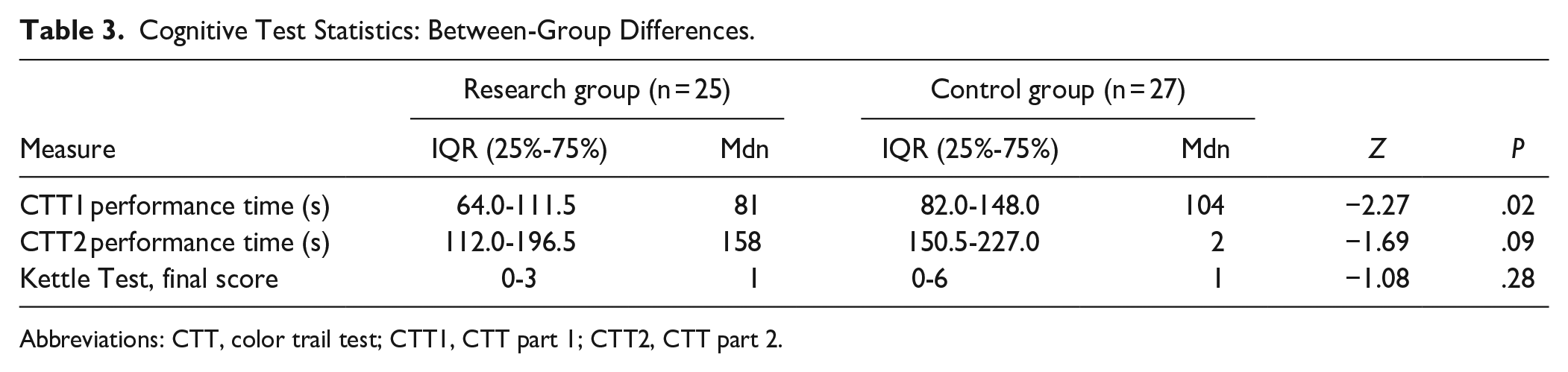
Abbreviations: CTT, color trail test; CTT1, CTT part 1; CTT2, CTT part 2.
Stroke survivors with dogs performed did not perform better (faster) on the CTT2 or Kettle Test. Mann-Whitney tests revealed no significant differences in the Kettle Test final scores between the stroke survivors with a dog (Mdn = 1) and the group with other CAs (Mdn = 1, Z = -0.38, P = .71) or between the group with a dog (Mdn = 137) and the group with other animals (Mdn = 188) in CTT2 performance time (Z = −1.03, P = .31). However, it showed significant between-group differences (with dog: Mdn = 67; with other animals: Mdn = 109.50) in CTT1 performance time (Z = −2.52, P = .01).
No significant correlations were found between the research group (n = 25) PAQ avoidance and ACS (rp = .32, P = .881) or WHOQOL (rp = −.13, P = .536) scores or between PAQ anxiety and ACS (rp = −.10, P = .627) or WHOQOL (rp = −.07, P = .734) scores.
When examining correlations between participation, QoL, and attachment scores in the CA-type groups (dogs/other), we found a significant strong negative correlation between the PAQ avoidance and ACS (rs = −.64, P = .01) scores only in the dogs group. The lower the PAQ avoidance score, the higher the ACS participation score. No other correlations were found.
Discussion
The present study aimed to examine differences in participation, QoL, cognition, EF, and CA attachment between stroke survivors living with or without CAs. The main results were that living with a CA is associated with higher post-stroke participation and cognitive function in selected domains. In addition, attachment to CAs was associated with participation (not QoL) only for stroke survivors living with dogs.
Participation levels of people living with CAs was previously reported,25,26 showing Inconsistency. Toohey et al 25 found that CA owners less likely than nonowners to participate frequently in social, recreational, or cultural activities or report life satisfaction. 25 However, nonowners were as satisfied with their social participation levels as owners were. Other studies showed that CA owners had higher activity levels for example, Headey et al 26 Our study’s results are consistent with this latter evidence, showing significantly higher participation for stroke survivors living with CAs, which are meaningful in many older adults’ lives. 5 Possibly, living and interacting with CAs, especially physical activities with dogs, could promote post-stroke participation. Involving CAs in rehabilitative interventions may affect stroke survivor’s health and well-being.
Quality of life is important for older adults experiencing life transitions, and their interactions with CAs can reduce associated stressors. 27 Based on that, we assumed that stroke survivors living with Cas will have higher QoL levels in comparison with stroke survivors without Cas. Interestingly, the present study didn’t find significant differences in general QoL scores between stroke survivors with or without CAs. Our hypothesis was not supported, adding to the contradictions in the literature. It may be more useful to measure QoL a while after the stroke survivors resume living with their Cas, since after returning to community life, stroke survivors need time to readjust—and a participation increase may take time to affect QoL. Specifically, the present study found higher QoL levels among stroke survivors living with dogs. Because stroke survivors’ QoL has been associated with greater community participation, 28 activities conducted with and for dog companions may affect QoL. Activities with dogs occur in more community-based contexts (eg, outside walks or social meetings with other dog owners) than activities with other CAs.
The present study also highlighted significant cognitive differences in cognitive performance between stroke survivors with and without CAs per the CTT1 but not the CTT2 or Kettle Test. Only a few studies for example, Gee et al 29 have examined the benefits of CA ownership, companionship, or therapy on human cognitive function in non-stroke samples, and those findings were inconsistent. Pet therapy has benefited cognitive function in older adults with mental health conditions, with increased Mini-Mental State Examination cognitive scores among pet owners. 30 Similarly, homebound older adult pet owners had significantly higher EF than nonowners, 31 as assessed using CLOX1, a clock-drawing task. 32 However, cognitive functioning has not been significantly associated with cat ownership. 33 Our results align with these earlier findings.
Although both CTT and Kettle Test are clinical cognitive tests, these different results may be explained with relation to the test type might explain. The CTT is a neuropsychological test examining cognitive components in a concrete, pen-and-paper, but unfamiliar task. The Kettle Test is a daily routine task performed in a natural environment and relies on clinicians’ observations. Previous reviews highlighted the need to evaluate cognition at the performance level, for example, Wesson et al 34 as the Kettle Test does. Performance-based cognitive assessments are vital because they measure real-life occupations through direct observation. 35
However, the Kettle Test did not identify cognitive function differences between the groups in our study. Possibly, objective pen-and-paper cognitive tests are more sensitive to cognitive decline than tests relying on more-subjective clinician reports. Another explanation could be that the Kettle Test’s IADL task does not reflect an appropriate functioning level for community-dwelling stroke survivors. Because it involves a routine task, it possibly led to automatic functioning.
Our study results show the participants’ cognitive disabilities in the CTT1 and CTT2 tasks according to CTT age-based norms 22 but no significant between-group differences in the CTT2 task. The CTT1 measures perceptual tracking, sustained attention, and graphomotor skills, whereas the CTT2 adds divided attention and sequencing skills (EF) to those skills. The lack of between-group differences in EF is congruent with findings from the Kettle Test, which also assesses EF.
The link between CA ownership and EF is unclear. Older adults with higher cognitive function might be more capable of caring for a CA. Conversely, having and caring for a CA might promote better EF. Given the scarce research, further longitudinal studies (eg, CA adoption) are needed to confirm the direction of the effect between CA ownership, cognition, and EF.
Another interesting finding was that attachment orientation to a CA was significantly associated with participation measures only in stroke survivors with a dog and only relative to their avoidance (not anxiety) score. It was not associated with QoL. These findings add to the literature on attachment orientation’s ability to explain the benefits of animal ownership in older adults. Teo and Thomas’s study comparing QoL and psychopathology between animal owners and nonowners 36 partly supports our study’s results. Teo and Thomas explored human–pet relationships according to 2 theories: Bowlby’s attachment theory and Rogers’ core conditions. 36 Their findings showed no significant between-group differences. However, secure pet attachments have been associated with less psychological distress and psychopathology. People who perceived higher levels of Rogers’ core conditions from their pets had higher QoL. Bowlby’s pet attachment insecurity predicted psychological distress and psychopathology, whereas Rogers’ total core conditions significantly predicted pet owners’ QOL. Our study participants’ low mean attachment avoidance and anxiety scores indicate secure attachments with their CAs.
Larger and more widely representative samples are needed to improve the evidence regarding relationships between living with CAs and stroke survivors’ participation, QOL, cognition, and EF performance. A more comprehensive exploration of potential mechanisms could establish stronger conclusions and support implementing interventions in community and rehabilitation settings.
Future studies to evaluate community-dwelling stroke survivors living with CAs could use other performance-based cognitive tests to incorporate more activities (the Kettle Test focuses on 1 IADL). Lastly, mixed methods, including quantitative interviews, can be used to explore the stroke survivors’ experience of living with CAs, and those findings can inform the selection of assessment tools for quantitative studies.
Because our sample of stroke survivors is relatively small and not representative, generalizing the findings to a broader population is limited. Further studies will need larger samples and representation to examine CAs’ contributions after stroke more deeply. In addition, the study’s cross-sectional design limits its ability to establish causal relationships between living with a CA and observed outcomes. Longitudinal studies would provide more robust evidence of the effects over time.
The results should be interpreted cautiously because some demographic variables (stroke onset, years of education, and age) correlated with participation and cognitive variables. Other potential confounding factors that may have influenced the results (eg, socioeconomics, social support, and previous experiences with animals) should be considered. Another confounding factor is that some participants owned a CA before their stroke, and some adopted the animal afterward.
Finally, different CA types may have different effects on human health. However, because the study sample was small, it was impossible to conduct suitable statistical tests to investigate the effects of each animal type. Potential mechanisms underlying the observed effects should be further explored. Future studies could also explore differences in activities conducted with Cas before and after the stroke, to further understand the impact of stroke on daily lives with CAs.
Conclusion
CAs may contribute to the cognition and participation of stroke survivors living in a community. However, no benefits were found relative to QoL, and attachment to a CA was not associated with participation or QoL. The presence of a CA in human life is an environmental factor that does not involve medical or invasive intervention, and when adjusted to the individual it may offer potential benefits. Future research should explore the benefits of integrating animals in rehabilitative interventions for stroke survivors.
Footnotes
Acknowledgements
We acknowledge Prof. Elizabeth R. Skidmore, from the Department of Occupational Therapy, University of Pittsburgh for her help with editing and part of statistical analysis, and her Cognitive performance laboratory team for their input. We acknowledge Prof. Avi Avital, from the Department of Occupational Therapy, University of Haifa, for his input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.