
Abstract
Objective:
The objective of this pilot study was to explore the impact of interpreter format (virtual vs in person) on clinical outcomes in patients with non-English language preference (NELP) and type 2 diabetes mellitus (T2DM) in a primary care setting. We hypothesized that NELP patients utilizing in person interpreters would have improved HbA1c values, better follow-up rate, and more complex care plans compared to patients utilizing virtual interpreters.
Methods:
We completed a retrospective chart review of 137 NELP patients with T2DM who required a medical interpreter (February to June 2021). We calculated univariate and bivariate statistics to characterize the sample and assess the extent to which measures of continuity (follow-up visit rate and time to follow-up visit), quality (change in HbA1c), and complexity (medication intervention complexity) were associated with interpreter type.
Results:
There was no statistically significant difference in follow-up rate or average days to follow-up visit for NELP patients with in person as opposed to virtual interpreters. Patients with virtual interpreters demonstrated a non-statistically significant decrease in HbA1c compared to those with in person interpreters. Finally, there was no statistically significant association between interpreter format and intervention complexity.
Conclusions:
Quality medical interpretation contributes to optimal health outcomes in NELP patients with diabetes. Our study suggests that both in person and virtual interpreters can be effective in providing care for NELP patients, especially for chronic disease management in the context of a primary care relationship. It also highlights the importance of pursuing additional qualitative and mixed method studies to better understand the benefits of various interpreter formats across different visit types.
Introduction
Significant health disparities exist in chronic disease outcomes among ethnically and racially diverse patients in the United States, including those with type 2 diabetes mellitus (T2DM). 1 Refugees, immigrants, and patients with non-English language preference (NELP) often develop diabetes at earlier ages and at rates that far exceed their country of origin.2,3 Ethnically diverse patients with diabetes in the United States demonstrate disproportionate morbidity and mortality outcomes compared to non-minority groups, even when controlling for other risk factors. 4 NELP patients experience higher hemoglobin A1c (HbA1c) values, poorer glycemic control, and increased T2DM complications, such as retinopathy and end stage renal disease.4,5
NELP is an independent social determinant of health faced by patients of diverse racial and ethnic minority groups when accessing healthcare. 6 NELP exacerbates other drivers of health disparities, including limited healthcare access, insurance coverage and utilization, and increases barriers to health, such as access to employment, living wage, healthy food, and transportation.7 -9 Additionally, NELP patients face cultural barriers, such as varied perceptions of health, limited health literacy, lack of trust, and fear of racism and discrimination.7,10 Linguistic barriers are also associated with worse health outcomes. Disparities have been attributed to multiple factors, including suboptimal patient-provider interactions.9,11 NELP patients experience higher rates of inappropriate diagnoses and medication complications, longer hospitalizations, and lower patient satisfaction scores and follow-up rates. 12
US federal laws require health care professionals to utilize interpreter services for NELP patients, 13 but it is unclear which modality is most effective. Professional medical interpreter services can be provided in person or virtually, via telephone or video. Multiple benefits have been noted with the use of professional in person interpreters. 14 In person interpretation improves understanding and integration of cultural nuances 15 and increases patient comfort. 16 In person interpreters are better able to assess patient needs, interpret body language and facial expressions, navigate the flow and pace of the visit, and improve patient understanding.17,18 In person interpretation is particularly important in scenarios involving rapport building, or with increased educational, cultural, or psychosocial complexity.16,19 In person interpreters decrease overall visit time across multiple settings.20 -22
In comparison, virtual interpreters have been shown to decrease patient wait times, 23 decrease healthcare costs and increase interpreter access and availability. 24 Virtual options improve access for patients with less common languages, in less centralized geographic locations, and during evening and weekend hours. 25 Easily accessible virtual interpretation increases rates of interpreter use by care teams and clinicians overall versus in person interpreters.26,27 Virtual interpretation provides increased flexibility for providers and patients, including preservation of patient anonymity and safety.28,29 Previous work suggests that while providers prefer in person interpreters, patients may not have a preference.28,30
Despite the prevailing literature on medical interpreters outlined above, we know less about how interpreter type influences clinical quality or disease outcomes. In attempt to address this gap, we undertook a pilot study to evaluate the impact of interpreter format (in person vs virtual) on clinical diabetes outcomes in NELP patients. Diabetes quality outcomes, including regular HbA1c monitoring and 3 months follow up visits are clearly defined, important measures of quality chronic disease management.31,32 We hypothesized that NELP patients who received in person interpretation would have higher rates of follow up, greater improvements in HbA1c score, and increased medication regimen complexity than NELP patients who utilized virtual interpretation.
Methods
We conducted an observational retrospective cohort study using medical chart review within a single family medicine clinic. Prior to the COVID-19 pandemic, the clinic utilized in person interpreters for the majority of NELP visits. Beginning in March 2020, interpreter services transitioned to virtual format, via telephone (primarily) and video. In response to fluctuating COVID positivity rates and changes in public health and health system guidance, the clinic transitioned between in person and virtual interpretation, leading to a mix of interpreter formats between February 1st and June 30th 2021. In person interpreters were contracted from 1 of 2 external translation agencies, and have completed at minimum a 40 hour interpreter certificate training, as well as an oral and written exam. Virtual interpreters were a combination of the previous mentioned translation services, internal, system-level interpreters, or through a phone interpretive service.
Setting
This research was conducted at an urban primary care clinic in a Midwestern state that serves an ethnically, culturally, and linguistically diverse population.26,33 A large proportion of patients were immigrants and refugees from Southeast Asia, East Africa, and Latin America. Based on 2021 statistics, 42% of clinic visits required an interpreter. The clinic is affiliated with a large state university and includes an interdisciplinary care team model. The clinic serves as a teaching site for undergraduate and graduate health professionals, including medical, pharmacy, and behavioral health trainees.
Study Sample
We employed inclusion and exclusion criteria to identify a study sample appropriate for our research question. Patients were eligible for inclusion if their record indicated: a diagnosis of T2DM; requirement of a medical interpreter; a hemoglobin A1c (HbA1c) laboratory value collected between January 1st, 2021 and January 1st, 2022; and at least 1 in person clinic visit between February 1st, 2021, and June 30th, 2021 with a diagnostic code for T2DM. Patients under age 18 years, those with type 1 diabetes, and pregnant patients were excluded.
Measures
Once the study sample was identified, we extracted multiple variables including patient demographics, language spoken, duration of diabetes diagnosis, HbA1c values, physician, presence of a clinical pharmacist visit, and the qualifying and the next subsequent diabetes visit dates and HbA1c value. In addition, certain variables required manual data extraction, including interpreter format and intervention complexity. One investigator manually reviewed visit notes in the electronic health record to determine interpreter format (in person vs virtual) present via nursing documentation.
To determine intervention complexity, we used an approach conceptually informed by the Medication Regimen Complexity Index (MRCI), a validated measure used to systematically classify the demands of medication regimens and previously used in adults with diabetes.27,34 The complexity of diabetes intervention was classified within the clinic visit based on MRCI items as well as the author team’s clinical perception of patient burden. Clinic visits were manually coded from 0 to +6, as follows: no medication change (0), dose increase or decrease of 1 existing medication (+1), dose increase or decrease in ≥2 existing medications (+2), initiating a new oral medication (+3), starting ≥2 new oral medications (+4), starting a new glucose monitoring device (+5), or starting a new injectable medication (ie, insulin; +6; Figure 1). These visit scores were subsequently collapsed into 3 complexity categories: low (score of 0), moderate (scores of 1-3), and high (score of >3).
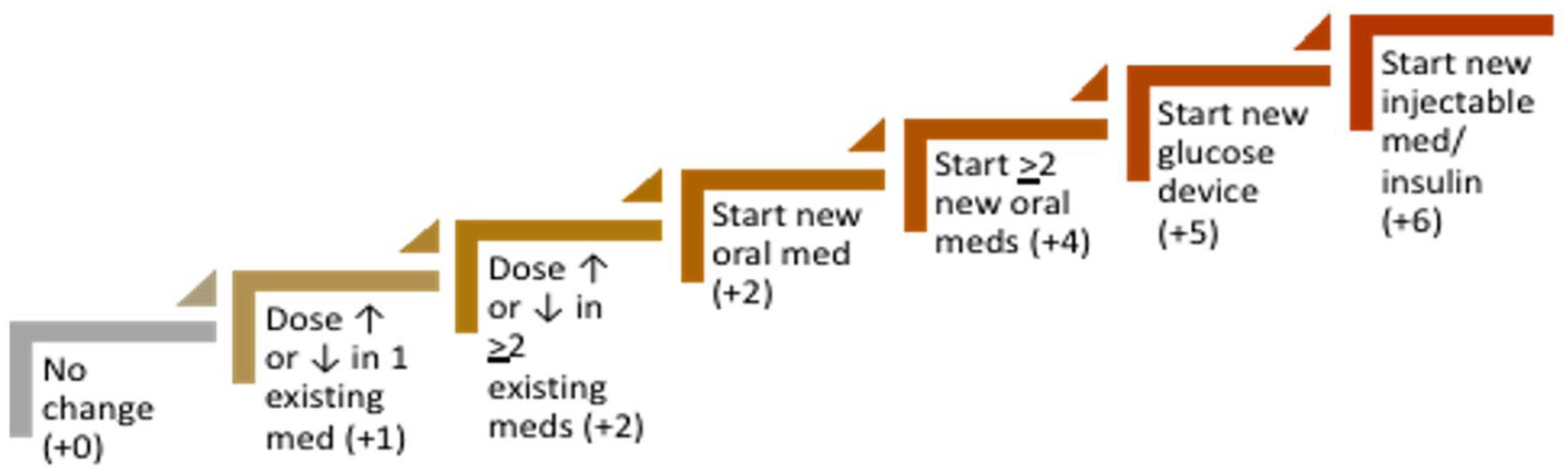
Coding scale employed to classify complexity of interventions at clinic visits among a sample of limited English proficiency patients of an outpatient clinic with Type 2 Diabetes mellitus, 2021.
Data Analysis
We calculated univariate and bivariate statistics to characterize the sample and assess the extent to which measures of continuity (follow-up visit rate and time to follow-up visit), quality (change in HbA1c), and complexity (intervention complexity) were associated with interpreter type. We employed available-case analysis given sample size differences across variables. For example, in order to calculate the average time to follow-up visit, those without a follow-up visit were necessarily excluded. Pearson chi-square tests were used to compare categorical variables by interpreter type and independent samples t-tests were used for continuous variables. To account for non-normal distributions for certain variables, we also replicated analyses applying logarithmic transformation for time to follow-up visit and HbA1c. We conducted 2-tailed analyses in IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY), and set a significance level of 0.05. This study was exempt from human subjects review by the University Institutional Review Board.
Results
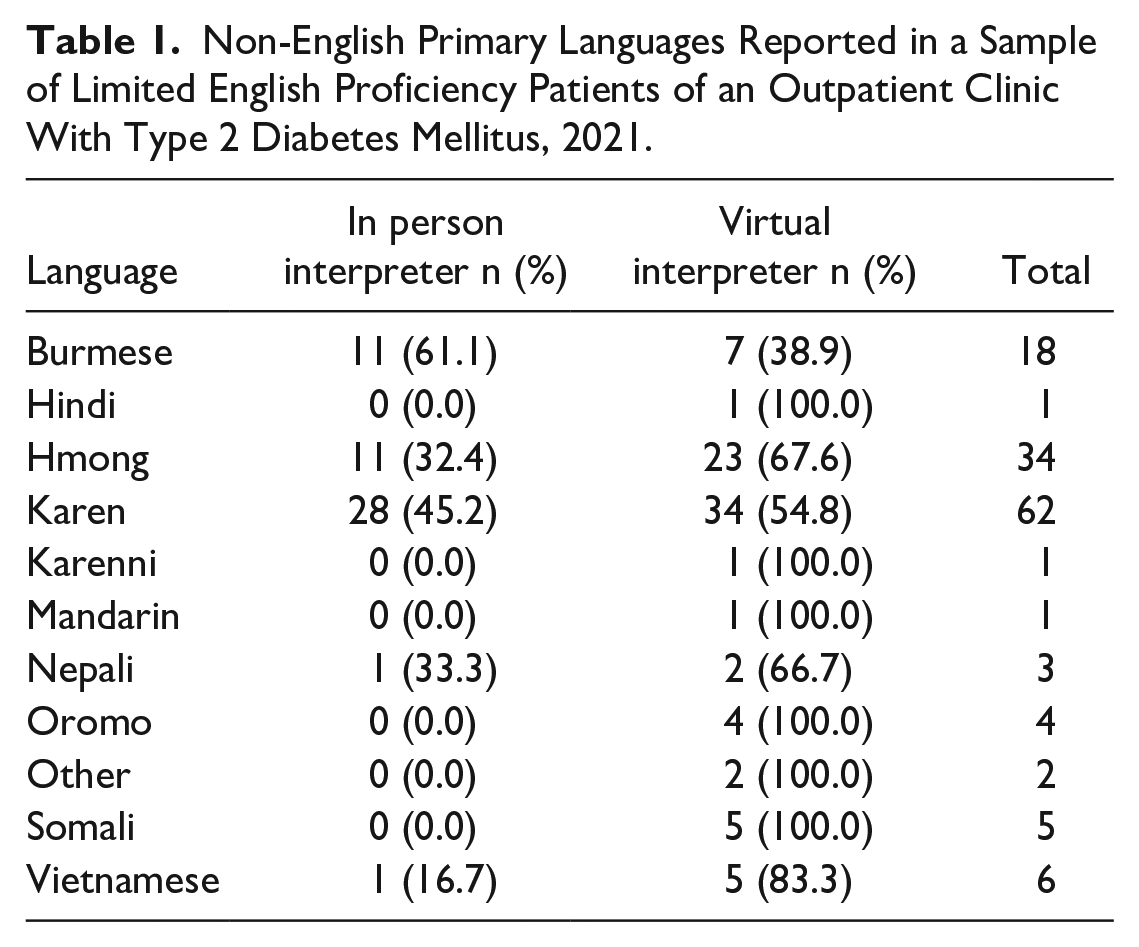
A total of 137 patients met inclusion and exclusion criteria and were included in analyses. In person interpreters were utilized for 38% of individuals and virtual interpreters were utilized for 62% of individuals. The sample was 62% female, with a mean age of 56.1 years and mean baseline HbA1c of 8.3. Interpreter format was not significantly associated with sex (χ2 = 0.72, df = 1, P = .79), age (t = 0.51, P = .61), or baseline HbA1c (t = -0.71, P = .48). The sample demonstrated a range of non-English preferred languages, with Karen, Hmong, and Burmese being the most common (Table 1).
Non-English Primary Languages Reported in a Sample of Limited English Proficiency Patients of an Outpatient Clinic With Type 2 Diabetes Mellitus, 2021.
Relationships between interpreter format and diabetes care measures are reported in Table 2. We observed a higher absolute follow-up rate for patients with in person (73.1%) as opposed to virtual (64.7%) interpreters, though this difference did not reach statistical significance (χ2 = 0.14, df = 1, P = .31). Similarly, patients with in person interpreters evidenced slightly fewer average days to follow-up visit (mean = 33.9, SD = 26.2) compared to those with virtual interpreters (mean = 34.7, SD = 33.2); again, this was not statistically significant (t = -0.12, P = .90). Patients with virtual interpreters demonstrated a greater, but not statistically significantly different, decline in HbA1c (-0.6, SD = 1.7) compared to those with in person interpreters (-0.3, SD = 1.5; t = 1.0, P = .32).
Diabetes Care Measures by Interpreter Type in a Sample of Limited English Proficiency Patients of an Outpatient Clinic With Type 2 Diabetes Mellitus, 2021.

Pearson chi-square test.
Independent samples t-test.
P-value remained greater than .05 when replicating analysis using log-transformed data.
For intervention complexity, the majority of visits were classified as low complexity, followed by moderate and high complexity. There were greater proportions of low and high complexity patients among the in person interpreter visits, and higher numeric representation of moderate complexity patients among virtual interpreter visits. However, there was no statistically significant association between interpreter type and intervention complexity.
Discussion
The ability of patients and providers to communicate effectively is essential to providing timely, safe, appropriate, and patient-centered care. In this study, we found no significant difference in diabetes continuity, quality, or complexity between virtual and in person interpreter formats, indicating both can be used effectively in providing care for NELP patients with diabetes. Patients across both in person and virtual interpretation groups on average improved HbA1c values, started or titrated medications, and returned for diabetes follow-up. This study has practical implications to how we provide care in an increasingly technology-based healthcare environment and suggests that virtual interpretation is an effective tool for specific clinical situations and populations.
Interpreter Type and Follow-Up Rate
Rates of follow-up and time to follow-up visit were similar between patients utilizing in person and virtual interpreters, though follow-up was more frequent when in person interpreters were used. Follow-up scheduling and visit attendance reflects multiple factors, including patient understanding of the care plan and follow-up recommendations, ability to easily schedule follow-up, and willingness to continue care with that clinic and clinician. In person interpreters, who may be able to assist with follow-up scheduling during the initial visit, likely improve follow-up scheduling and return rates.
Interpreter Type and Glucose Control
HbA1c values and change in HbA1c values were also similar between groups, with greater HbA1c improvement in the virtual group. This suggests that virtual interpretation is an effective means to evaluate patient diabetes control and implement changes to improve HbA1c. Patients with virtual interpreters were more likely to have visits with moderate complexity, versus low or high complexity, suggesting that gradual, step-wise changes in the care plan are an effective means to improve HbA1c, especially when using a virtual interpreter to communicate with patients.
Patients build experience and understanding of diabetes over time, including knowledge of diet, medications, and blood sugar monitoring techniques. Medical decision making in patients with diabetes often includes small adjustments based on objective lab and self-monitoring values versus subjective patient-reported symptoms. T2DM treatment involves titration of medications along evidence-based guidelines and is effective in English-speaking patients when provided virtually.35,36 Previous work also indicates the value of in person interpreters in both developing relationships16,37,38 and providing patient education. 16 Comparing the time of diabetes diagnosis and duration of clinician-patient relationship could further evaluate this impact. In person interpreters may have greater impact in patients with newly diagnosed diabetes, or new to a clinic or clinician, where significant education about the disease, monitoring, diet, and treatment options is needed.
Limitations and Future Directions
Our results provide preliminary evidence from a single urban primary care clinic with a family medicine training program. They reflect the impact of interpreter format at a single visit in the context of long-term chronic disease management. Our study focused on the presence and timing of a patient’s next follow-up visit but did not look at the total number of patient contacts during the time period, nor interpreter format utilized at follow-up visits.
Although in person and virtual groups in this study were similar in age, sex, and baseline HbA1c, other factors may have contributed to differences between groups. Virtual versus in person groups were not random; health system policy during the study period required providers to submit written requests, indicating a patient met criteria for use of an in person interpreter. Common indications include communication challenges, such as limited hearing, cognitive deficits such as dementia, severe mental health diagnoses, or limited health literacy. Our study did not compare overall medical complexity, social complexity, or cognitive function variability between patients in virtual and in person groups, which affects the challenge and complexity of interpreting work 37 These patients may have additional challenges with taking medications, especially incorporating new medications or medication changes, and/or have higher target HbA1c goals.
Our study did not measure social determinants of health or health literacy levels between groups nor assess its impact on interpreter format or diabetes outcomes. Effective diabetes care plans are multifactorial, including blood sugar monitoring, diet, and exercise and heavily impacted by patient social determinants of health and health literacy. Access to income supports, healthy food, exercise facilities, transportation, and neighborhood safety all impact a patient’s ability to follow up and their A1c levels. Relatedly, we did not evaluate the influence of care coordination or interdisciplinary interventions on study outcomes, which could be valuable in future research. For example, at this clinic most patient education around glucometers and injectable diabetes medications was provided by clinical pharmacists, while diet and lifestyle education were provided by nurses, dieticians, and behavioral health specialists.
75% of in person interpreter visits included Karen or Burmese speaking patients, an ethnic group newer to the United States, and with increased barriers to accessing healthcare services and knowledge of Western medicine.39,40 The majority of these visits utilized 3 well-known, frequently-used in person interpreters of the clinic. These interpreters often serve patients with limited health literacy, mental health diagnoses, and cognitive or memory concerns, often with looser HbA1c goals, and increased barriers to tight glycemic control. It is likely that the in person group reflected those with greater complexity and lower health literacy compared to the virtual group, although baseline HbA1c was similar across groups. When set up effectively, even dementia assessments can be conducted via telemedicine, but in person is preferred. 19 A randomized study would help ensure similar study groups and better assess the impact of interpreter modality, as well as clarify which patients benefit most from specific formats. Further research should focus on elucidating which patient factors, medical or social needs might predict a favorable response to each format.
Clinical Implications
Study results should be interpreted thoughtfully, as they may not be generalizable across communities, clinics, language, specialty, or clinical situation. Diabetes visits, like many chronic diseases, include minimal diagnostic ambiguity, a limited scope of physical exam maneuvers, and rarely require procedural intervention, situations where the use of an in person interpretation may have additional benefits. Primarily discussion-based visits with a defined diagnosis simplifies communication between patient, clinician, and interpreter as compared to other visit types and diagnoses.
Chronic disease management, such as in T2DM, may be an effective model for the use of virtual interpreters. This care is often provided in the context of a longstanding patient-clinician relationship, where rapport already exists. Primary care providers (PCP) often have a pre-existing knowledge of a patient’s cultural background, health literacy level, social context, and views on medication and interventions. This established rapport likely improves communication effectiveness in the virtual environment.
Patients presenting with new complaints, or requiring more complex history taking and physical exam maneuvers, may benefit from the use of an in person interpreter. More complex diagnostic work, include ED visits may further benefit from in person interpretation.18,20 Patients with new or high complexity diagnoses, when initiating high risk medications and treatments, or visits with a large educational component may benefit from in person interpretation. Visits with interdisciplinary team members, such as nutritionists, clinical pharmacists, and behavioral health specialists may also benefit from in person interpreters.
Conclusions
This initial study suggests that in person and virtual interpreters can be equally effective in providing high quality diabetes care in a sample of NELP patients primarily from Southeast Asia. Further exploration is needed to determine for which patients each modality is most appropriate. Virtual interpretation may be particularly useful in the context of chronic disease management and an established patient-clinician relationship. Access to interpreters, timeliness, cost, and patient preference are other important factors to determine the overall impact of interpreter format on patient outcomes. Further studies are needed, including exploration of patient experience and preference, to more fully understand the benefits of various interpreter formats, and prioritize and best utilize these essential members of the healthcare team.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.