
Abstract
Objectives:
Despite Canada’s universal health system, sex workers across the country face an alarmingly high number of barriers when they seek to healthcare services. This has resulted in unmet healthcare needs and substantially poorer health outcomes than the general Canadian population. The objective of this study was to use a systems thinking approach to gain an in-depth understanding of the barriers sex workers face and how access could be improved.
Methods:
The analysis was conducted using a systems thinking methodology, which incorporates systems tools and inquiry processes. The methodology comprised 2 domains of inquiry: (1) Problem Landscape, (2) Solutions Landscape. Systems tools and methods, such as causal loop diagrams, iceberg diagram, and systems mapping, investigated the problem landscape for understanding the interconnected nature of the issue, alongside review of both published and gray literature. An environmental scan explored the current solutions landscape. These methods connected through systemic inquiry processes, including ongoing review and application of diverse perspectives, boundary judgments, interrelationships; enabled gaps and levers of change to be determined.
Results:
The main barriers sex workers face are stigma, criminalization, accessibility, and cost of healthcare. The stigma of sex work stems from otherization, paternalism, and moralistic, faith-based beliefs. The barriers unique to sex work are stigma and criminalization; both of which surface as avoidance, dislike, and/or fear of medical professionals. Five gaps each with a lever of change to improve access were identified: (1) Stigma – Collectivization and external collaboration, (2) Criminal status of sex work – Decriminalization, (3) Lack of adequate education - Improved healthcare professional training and anti-discriminatory health policies, (4) Lack of support – Increased community-based healthcare services, (5) Cost of healthcare – Universal coverage of “secondary” healthcare components.
Conclusion:
Through reducing the stigma surrounding sex work, making changes that improve the healthcare services that sex workers receive, and collaboration between involved parties, sex workers can be prevented from falling through the cracks of the Canadian healthcare system; lessening the health inequities sex workers face and improving their health outcomes.
Keywords
Introduction
Despite Canada’s universal health system, sex workers across the country face an alarmingly high number of barriers when they seek to access healthcare.1,2 Access to care is a key determinant of health for all humans 1 and sex workers are almost 3 times more likely than the general Canadian population to not have access to the healthcare services they require. 2 This results in unmet healthcare needs and substantially poorer health outcomes for sex workers. 2
Healthcare should be accessible for all. The universal healthcare system in Canada holds the basic values of fairness and equity. 3 There is an expectation Canadians receive quality care when required from a team of knowledgeable healthcare professionals at little or no cost. This is not the experience of many sex workers when they attempt to receive care. Instead, in many circumstances they are met with judgment, profiling, and inadequate care. 4 Often, the true extent of harm that vulnerable populations experience is unseen or completely ignored. This is a reality for many sex workers when trying to access healthcare, as a vast majority of Canadians are rarely confronted with the realities of this preventable problem.
Background
What Is a Sex Worker?
Sex work is an umbrella term that defines those involved as adults who exchange sexual services for money or material benefit. 5 Sex workers encompass a diverse population, including people of all genders, races, and ages. This breadth is mirrored in the work environments that comprise the sex industry; including, but not limited to, indoor and outdoor spaces, brothels, commercial venues (eg, escorts, erotic massages, exotic dancers), and online (eg, porn, camming, phone sex operators). The sex industry is complex and ever evolving along with broader technological, legal, and socio-cultural changes.
While mainstream media often depicts sex workers as street-based, in Canada, outdoor sex work only makes up about 20% of all sex work, while the majority (over half) occurs in the indoor independent category. 4 The majority of the sex industry identifies as women, current research estimates around 75%. 4 In Canada, there is a disproportionate representation of Indigenous women in street-level sex work, an estimated 15% to 20%.5 -7 This is due to the effects of colonization that have marginalized Indigenous peoples socially and economically, as well as prevalent racist perceptions, it may be their only option for survival.5,6
The Canadian Healthcare System
Canada has a universal, publicly-funded healthcare system. The federal government creates the national principles for the system under the Canada Health Act: publicly administered, comprehensive, universal, accessible, and portable across provinces. 3 Each province/territory administers their own public healthcare system and determines which treatments are “medically necessary.” 3 Although many healthcare services and treatments come at little or no cost to the patient, services considered to be “secondary” are not covered by public health insurance, including prescription medications, dental care, physiotherapy, counseling/therapy, homecare, therapeutic massage, ambulance services, and optical care.
Methods
The objective of this study was to use a systems thinking approach to gain an in-depth understanding of the barriers sex workers face and how access could be improved. Systems thinking is a methodology used to analyze complex systems.8 -13 The methodology stems from the business sector and adapted for other disciplines. According to Arnold and Wade, systems thinking can be completed through identifying and understanding: (1) interconnections, (2) feedback loops, (3) system structure, (4) stocks, flows, and variables, (5) non-linear relationships, (6) dynamic behavior, and (7). systems at different scales; accompanied by modeling systems conceptually by reducing complexity. 8
The analysis comprised 2 domains of inquiry: (1) Problem Landscape, (2) Solutions Landscape. To deeply understand the problem and solutions, systems tools, and methods are used to define the landscape by providing the interrelationships between the problem and the solution. The systems tools and methods employed were causal loop diagrams, iceberg diagram, and systems mapping. Alongside the review of both published and gray literature and informal conversations with people knowledgeable on the issue, including academics and professionals in gender studies, healthcare, social work, physical sciences, and law enforcement; federal and provincial Ministers of Health; and representatives of sex work and community healthcare organizations. Causal loop diagrams enable a non-linear thinking process to how factors are connected and affect one another, either in a reinforcing or balancing manner. The iceberg diagram is a structural representation of observed events and underlying factors. Systems mapping involves bringing these aspects together into an overarching illustrative diagram to understand the extent of the problem. This methodology also included analysis of parties involved in the system, underlying structures, including federal, provincial, and municipal policy, and mental models. All these techniques were brought together in summary causal loop diagrams developed using Kumu software (Figures S1 and S2).
These methods connected through systemic inquiry processes, including ongoing review and application of diverse perspectives, boundary judgments, flow of resources and information, and interrelationships; and enabled the analysis of the solutions landscape. 10 An environmental scan was employed to understand solutions and innovations currently in place locally, nationally, and internationally. Using the understandings gained from the problem landscape and the environmental scan of the solutions landscape, gaps to access and levers of change were determined. Levers of change, a systems thinking tool, are leverage points within a system that have the potential to act as a catalyst for systemic change. 11
Reflexivity is key to the ongoing reevaluation of perspectives in systems thinking.12,13 This study employed a trauma-informed, human-first perspective. All researchers completed ethics trainings (TCPS 2: CORE-2022; CITI: GCP) and took into account feminist frameworks, cultural competency, and trauma-informed research practices.14,15
Boundaries of the Analysis
Important to the systems thinking methodology is defining boundaries as complex issues are large and vastly interconnected. 10 As an industry, sex workers face similar barriers to accessing healthcare services; although, it is important to recognize that as individuals they will experience these various barriers uniquely. Due to the complexity of the sex industry and the research available, this analysis focused on sex workers in Canada who engage in direct physical contact with clients (ie, street-based, indoor supervised or independent), as they are the sex worker population most susceptible to stigma and barriers to accessing services. 16
Problem Landscape
Sex workers face various social and physical barriers when trying to access healthcare. A study based in Vancouver, BC found that 70% of the sex workers surveyed experienced barriers to healthcare; 3 times higher than the estimated difficulty of accessing care among the general Canadian population. 1
Analysis of Parties Involved in the System
Outside of the central node, sex workers, the primary parties involved in their access to healthcare are: Canadian Government, healthcare professionals, provincial healthcare agencies, community organizations, and advocacy groups (Figure 1). Each has a role to play in the barriers that sex workers face when accessing healthcare, affecting them either positively or negatively.

Parties identified for their involvement in the healthcare access of sex workers.
Barriers to Healthcare
The main barriers sex workers face are (i) stigma, (ii) criminalization, (iii) accessibility, and (iv) cost. While cost and accessibility are similarly identified by other Canadians, they are significantly larger barriers for sex workers due to their additive effect when combined with other barriers. 2 The barriers unique to sex work are stigma and criminalization; both of which surface as avoidance, dislike, and/or fear of medical professionals.
Mental Model – Stigma
Stigma is multifaceted and the largest barrier that sex workers face. Stigma reduces an individual’s ability to be socially accepted and lessens them from a whole person to a tainted, discounted one. 17 Stigma is produced through perceived, enacted, and internalized forms. Perceived stigma is when a person’s fear of discrimination leads them to consciously or unconsciously change how they think and act. 18 For sex workers, this may lead to avoidance of social situations where they fear they will be treated differently if their occupation is revealed. Enacted stigma is when someone is actively treated poorly because of negative societal beliefs held about them. 18 This can involve labeling, stereotyping, separating, status loss, or discrimination. Internalized stigma is the acceptance and application of stigma to oneself. 19 Stigma influences the perceptions of sex workers that society holds and reinforces the discrimination they face in everyday life. 20
The consequences of stigma are far-reaching and apply to the whole industry at varying levels. Sex workers are often denied equal access to quality healthcare services due to stigma. The stigma of sex work stems from otherization, paternalism, and moralistic, faith-based beliefs. These mental models see those working in service roles as “second-class citizens” and associates sex work with 3 types of taint: physical from contact with bodily fluids and bodies, social from engaging in service work and association with other stigmatized groups, and moral from having their work perceived as “sinful.” 17 Together, these forms of taint contribute to the incorrect assumptions and blame placed on sex workers. Examples include: breakdown of the traditional family, vectors of disease, escalating crime, subversion of youth, transgression of gender norms, and entrenched beliefs of sexuality (Figure 2).4,21

The stigma of sex work is derived from various deeply rooted mental models and surfaces as 3 taints: physical, social, and moral, and often harmful assumptions.
Women and Indigenous peoples, the largest demographics of Canadian sex workers, have decreased access to healthcare before adding the barriers associated with sex work. 5 The healthcare needs of sex workers, Indigenous peoples, and women are often considered to be “secondary.”6,16,22 Women are less likely to be taken seriously by healthcare professionals, with the exception of pregnancy. 22 When sex workers seek care, regardless of their concern brought forth, often the focus becomes their sexual health. 16 The cultural preferences of care of Indigenous peoples are often ignored by Western medicine practitioners and met with discrimination. 5 Each of these identities when associated together lead to an exacerbation of health inequities. Furthermore, sex workers often have intersecting stigmas (eg, assumed substance use, gender identity, mental illness, HIV status, ethnicity, sexual orientation, socioeconomic status), meaning when a person falls into multiple of these categories, the barriers they face are significantly increased (Figure 3).20,21 Stigmatization is also linked to poor physical and mental health, and negatively associated with quality of life. 17

Feedback loop of intersecting stigmas, which have an additive effect resulting in worsened health outcomes.
Criminalization
In 2014, the Canadian federal government implemented the Protection of Communities and Exploited Persons Act (PCEPA) under the Criminal Code of Canada. It was introduced in response to Canada v Bedford (2013), wherein the Canadian Supreme Court ruled that the laws pertaining to the sex industry put workers at risk (Figure 4).
6
The PCEPA aimed to:
Protect those who sell their own sexual services; protect communities, and especially children, from the harms caused by prostitution; and reduce the demand for prostitution and its incidence.27,23

Interactions between sex work and levels of governance in Canada.
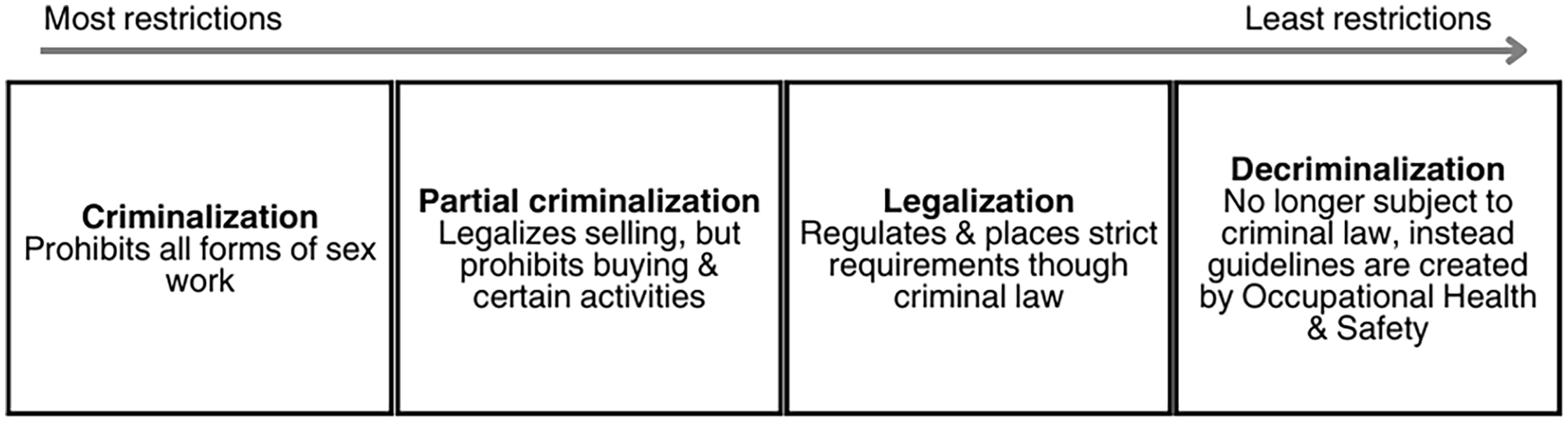
The PCEPA is categorized as partial criminalization (Figure 5). It legalizes the sale of sex, but criminalizes certain aspects of sex work, including purchasing services, receiving material benefits from another person’s sex work, and procuring clients (eg, publishing advertisements using newspapers or websites). 24 This is an “end demand” approach that criminalizes clientele and third parties (eg, managers).24,25 The legislation treats sex work as a form of sexual exploitation, frames sex workers as “victims,” and equates sex work with human trafficking. Criminalization has trapped sex workers in the dualities of both criminality and victimization. 25
The criminalization of sex work undermines the health and human rights of sex workers. It perpetuates stigma and marginalization; increases rates of drug use, violence, sexually transmitted infections (STIs), and human immunodeficiency virus (HIV); and decreases access to healthcare services (Figure 6). 25 Despite one of the legislation’s explicit goals being to increase access to services and supports for sex workers, a recent study found access significantly decreased by 41% for health services (86.2% in 2010-2013 to 45.2% in 2015-2018) and 21% for support services (88.7%-67.8%). 24 The PCEPA endangers the community it was created to protect. It is apparent that changing the law is not enough, when that law still holds the values associated with the stigma of sex work.
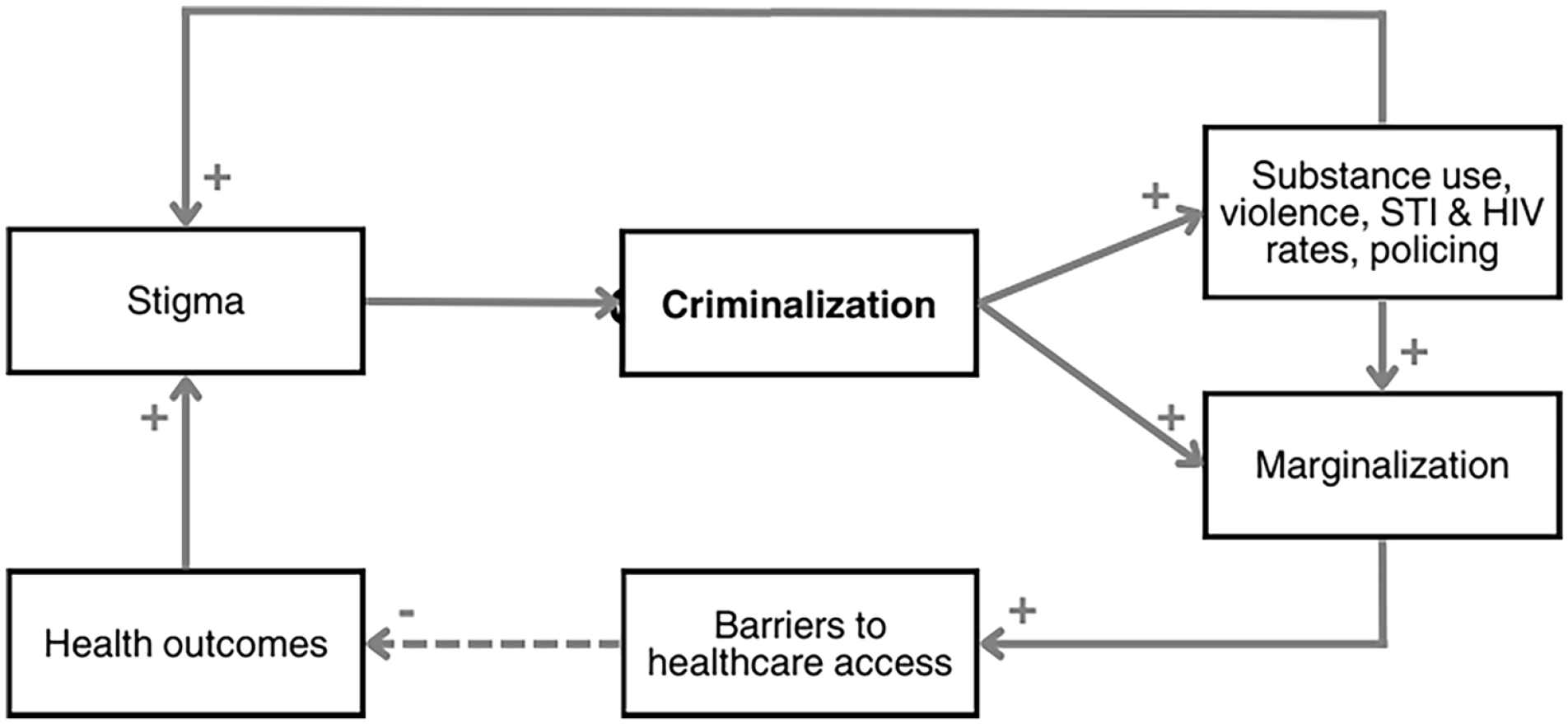
Feedback loop of the effects of criminalization on sex workers’ health.
Access to Care
Access to care includes the location of services and treatment, service availability, and personal considerations, such as transportation. The most prevalent accessibility barrier that sex workers face is service availability (eg, long wait times, limited hours of operation). 1 While this is a similar barrier identified by other Canadians, there are some aspects unique to sex workers. Such as work circumstances, particularly when working in an indoor supervised situation (ie, restrictions from management) and personal responsibilities may limit a sex worker’s ability to seek care when needed, especially if healthcare services are a distance from their home or place of work.
Outdoor-based sex workers often work on strolls, strips of road with regular solicitation of clientele, most often located in impoverished areas of cities.4,20 Such areas have serious health and safety concerns, as well as a lack of access to health services. 26 Furthermore, without a physical address, many medical centers will refuse to treat a patient, even if they are in possession of a provincial health insurance card. For example, in Calgary, Alberta community health services (eg, harm reduction and Indigenous health programs, Southern Alberta HIV clinic) are concentrated downtown, which is not easily accessible from the prominent outdoor sex work market (ie, 40-minutes on transit, 100-minute walk). The situation in Calgary is similar to many other Canadian cities, where the stigma of sex work, combined with a lack of accessible health services, has led to an environment that disallows sex workers to receive the healthcare they need.
Cost of Healthcare
On average, sex workers are more likely to identify cost as a barrier to healthcare than the general Canadian population (Figure 7). 2 A reason for this is that sex workers do not have access to secondary health insurance through work benefits like other professions and many cannot afford private insurance. 27 Without coverage, many treatments and services can be too expensive to receive. Another source of barriers is a result of the criminalization of sex work. The current legislation in Canada does not recognize sex work as a legitimate occupation, subsequently, sex workers have reduced access to credit. 2 They may earn a high wage, but without credit they are deterred from purchasing items, such as a house, bank loan, or accessing secondary insurance.

On average sex workers are more likely to identify cost as a barrier to healthcare than the general Canadian population, stemming from federal legislation.
Some services not covered by public insurance are available to low-income Canadians through provincial income assistance programs. For example, in Alberta, the government insurance aid program requires an individual to make less than $16,580 annually and not be the beneficiary of any other government program (eg, income support). Many sex workers are ineligible for such services meant to aid those in need of secondary insurance.4,27 While insurance coverage does not only affect sex workers, due to the criminal status of sex work and the other identified barriers, the lack of insurance coverage adds to the difficulty sex workers face when accessing healthcare.
Consequences of the Issue
These barriers to care have led to unmet healthcare needs and decreased quality of care. A study comparing Canadian Community Health Survey responses between sex workers and the general population and found that 46.2% of sex workers reported having poor general health (general population: 28%) and 60.6% reported poor mental health (general population: 23%). 2 As well, sex workers have significantly greater unmet healthcare needs than that of the general Canadian population, 40% versus 14.9%. 2
A reoccurring theme is that judgment and inadequate care is being received by sex workers from healthcare professionals.1,21,28,29 42% of sex workers in a cross-Canada study experienced a negative response after disclosing their occupation to a healthcare professional. 17 Sex workers report that healthcare providers use patronizing and dehumanizing behaviors, disrespectful and abusive language, humiliation, inferior service, denial of care, and blame when reporting sexual assault after disclosure of their occupation. 17 This forces them to spend excessive time and resources to find a healthcare provider or clinic where they feel valued and understood.
Often when seeking care, sex workers are not looked at as a whole patient. Instead, their care is led by healthcare providers’ preconceived notions of sex work, reducing treatment to sexual health only. 21 Sex workers have complex healthcare needs that greatly involve risk prevention and harm reduction.1,29 but there is a lack of healthcare providers knowledgeable about the needs of sex workers. 7 This is due to the limited formal diversity training healthcare providers receive. 30 While sexual health is an important issue for many sex workers, they are complete human beings and seek medical attention for more than just those issues.
Solutions Landscape
It is well established that sex workers have poorer health than the general Canadian population.4,28,29 The main attributing factor to sex workers’ worse health outcomes and high rates of unmet healthcare needs are the social and physical barriers that they face. In order for this to be lessened various changes, ranging from social structures to healthcare training, need to take place.
This issue has limited research available; likely due to the stigma surrounding sex work. This makes it more difficult to gain funding when compared to other less “tainted” topics (Figure 8). There is also a limited range of solutions currently being implemented. While most large cities have sex worker support organizations, there is a lack of collaboration between regions and between involved parties.

Feedback loop caused by the stigma surrounding sex work resulting in a lack of research and solutions.
Current Solutions in Place
On a community scale, advocacy and support organizations for sex workers should have a team focused on sex workers’ general health. This is important as many support services are instead oriented primarily toward human trafficking and sexual violence prevention. Organizations should take a harm reduction and humans rights-based approach to sex work; for example, Shift, a sex work-focused program in Calgary. 31
On a national scale, organizations should focus on cross-country collaboration to further research and advocacy efforts. For example, An Evaluation of Sex Workers Health Access, a community-based, sex worker-led project located in Vancouver, which conducts research, provides health visits, and documents the lived-experiences of sex workers and parties who provide services to sex workers. 32 Creating safe spaces for sex workers by sex workers will enable access to supportive healthcare services.
Internationally, New Zealand is a leader in sex workers’ human rights. New Zealand implemented the Prostitution Reform Act in 2003, 33 becoming the only country in the world to have decriminalized sex work. The Act provided a framework to safeguard sex worker human rights and promote welfare and occupational health and safety. 34 While developing the Prostitution Reform Act in 2003, sex workers were meaningfully included and consulted. 35 This was not the case during the development of the PCEPA. Instead of listening to the concerns raised by sex workers during the development of the legislation, they were ignored by the decision-making bodies involved. 36 While Canadian sex workers face decreased access to healthcare and worsened health outcomes, in New Zealand, sex workers gained greater control over their lives and increased occupational benefits; as well, condom use increased, rates of STIs decreased, and access to health services increased.34,35,37 Other countries can look to these successes to adapt their own policies and practices.
Gaps and Levers of Change
The deep understanding of the problem and solution landscapes allowed for the identification of 5 prominent gaps inhibiting sex workers’ access to care: stigma, criminalization, medical education, support services, and cost. Levers of change with the potential to deliver widespread positive change were identified for each (Table 1).
Impact Gaps and Levers of Change to Improve Sex Worker Access to Healthcare.

Conclusion
The issue of sex workers’ access to healthcare is complex. There are various systems, patterns, relationships, and mental models in place that hinder this occupational group’s access to a fundamental human right. Through the reduction of the stigma surrounding sex work, improvement of the healthcare services that sex workers receive, and collaboration between sex workers, government, healthcare bodies, and other parties involved, sex workers can be prevented from falling through the cracks of the Canadian healthcare system. Thus lessening the health inequities sex workers face and improving their health outcomes.
This problem not only exists in Canada, but persists around the world. While the barriers and recommendations explored in this paper pertain specifically to Canadian society, they may be applicable elsewhere.
Study Limitations
This study is limited by the lack of research available on sex workers’ access to healthcare. Much of the literature available is instead focused on sex workers and relations with other stigmatized topics (eg, HIV/STI rates, substance use). This gap in academic literature is due to the stigma surrounding sex work. The research conducted for this project aimed to address some of the gaps in information available.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241233173 – Supplemental material for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach
Supplemental material, sj-docx-1-jpc-10.1177_21501319241233173 for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach by Kaitlyn Squires in Journal of Primary Care & Community Health
Supplemental Material
sj-tiff-2-jpc-10.1177_21501319241233173 – Supplemental material for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach
Supplemental material, sj-tiff-2-jpc-10.1177_21501319241233173 for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach by Kaitlyn Squires in Journal of Primary Care & Community Health
Supplemental Material
sj-tiff-3-jpc-10.1177_21501319241233173 – Supplemental material for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach
Supplemental material, sj-tiff-3-jpc-10.1177_21501319241233173 for Sex Workers in Canada Face Unequal Access to Healthcare: A Systems Thinking Approach by Kaitlyn Squires in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The author thanks all those who contributed their time and expertise to this project, particularly: Carol Armstrong, Nick Strzalkowski, Katharine McGowan, Peter Choate, James Stauch, and those who shared their perspectives and experiences during the stakeholder conversations.
Author Contributions
All authors contributed to the study conception, design, material preparation, and data collection and analysis. All authors contributed to writing the first draft of the manuscript and commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by Mount Royal University. This study does not involve any human or animals subjects, thus approval from the ethics committee is not required. For the conversations held with stakeholders, informed consent was obtained verbally and all identifying information was anonymized.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.