
Abstract
This paper examines empathetic behavior in the United States, a strongly individualistic country, as contrasted with Hungary and Ethiopia, which are moderately individualistic and strongly collectivistic respectively. It suggests that empathy may have a wider than originally perceived application in diverse settings to combat factors of ethnic bias and discrimination that adversely impact health. Models that distinctly focus on the development of healthcare provider empathic care are needed to enable the needs of resource scarce regions of the world to be met, including pockets of the U.S. More investigation is warranted on how empathic behavior can positively impact health outcomes and disparities.
Keywords
Introduction
This paper is narrowly focused on a comparison of health care related empathic care behaviors in 3 culturally different countries: Hungary, Ethiopia, and the United States. The paper considers that there is value in research scientists conducting broader research on how the attribute of empathic care may be effectively employed in social work and nursing school settings as a tool for health promotion—particularly to abate health disparities among minorities and vulnerable populations.
Empathy is the ability to actively identify with and understand the suffering of others, thereby enabling that person to express care. As such, it is an integral component of Alfred Bandura’s social learning theory 1 and social cognitive theory, 2 which posit that social behaviors are intrinsically tied to a person’s identification with another’s beliefs and values. According to the World Health Organization (WHO), 3 “The right to health for all people means that everyone should have access to the health services they need, when and where they need them, without suffering financial hardship.” Sadly, despite the WHO’s statement’s empathic intent to address aspirational goals, widening health care disparities show no sign of waning, nor is there any coordinated international effort to improve the conditions of vulnerable people around the world. 4 When countries seem unable to implement the WHOs guidelines, that is when other avenues for humanistic, patient-centered care pathways must be explored—including educational strategies for health providers in clinical environments everywhere.
Training of health care providers (eg, nursing and social work) in empathetic behavior has the potential to be a complementary and a powerful tool to address patient misperceptions and increase access to care. It could also help tackle discrimination in health care, which the WHO states is “widespread across the world and takes many forms.” 4 Cultural competency is a vital concept that is needed by health care providers to work within multicultural societies, particularly in light of increased marginalization, regional conflict, and entrenched educational and income disparities. However, despite expanding multiethnic populations in the United States (who now constitute a major proportion of consumers of health care), there is still no uniformly accepted cultural education program to reflect these demographic changes. 5 Social, as well as economic factors, can adversely impact the quality of care afforded to vulnerable populations in clinical environments. Social advantage “refers more generally to someone’s relative position in a social pecking order—an order in which individuals or groups can be stratified by their economic resources, as well as by race, ethnicity, religion, gender, sexual orientation, and disability. These characteristics can influence how people are treated in a society.” 6
The cultural differences highlighted in this paper about empathic care and the barriers to affording patient-centered care illuminates a common theme centered on a conscious need to improve cultural sensitivity methods of training to incorporate empathic care into health care settings—not only in the U.S. but also in countries that do not have the same level of material resources, yet suffer, like the U.S. from health inequities, driven by ethnocentrism and bias. There is scarce research on predictive power of providers working in clinical environments that prioritize empathic, compassionate care, versus those that emphasize purely allopathic support. This paper addresses whether or not future research should more fully explore the prioritization of empathic care by social work and nursing providers, as a novel gateway to improved patient-centered health, particularly in resource scarce, multicultural settings.
We pose the following question: Is greater consideration of the significance of health provider empathic behaviors in nursing and social work settings warranted, in order to more fully address the unmet healthcare needs of diverse populations?
Rationale for the Selection of 3 Countries in the study on Empathy
Recent global trends (including climate driven demographic shifts in migration and refugee status, combined with the adverse impact of COVID-19 around the world, and expanding child poverty) highlight an urgent need for culturally diverse ideas about how health care providers can be empowered and better prepared to show more empathy in light of increasingly vulnerable populations. The current state of worldwide resource scarcity demands new constructs by which provider empathic care can be expressed.
Countries included in this exploratory cross-cultural paper on how empathic care is employed in nursing and social work settings include: the United States, Hungary, and Ethiopia. Country selection was based on the following criteria: they had to be culturally distinct, and they had to represent either an individualistic or collectivistic culture. Hungary, with a Hofstede Insights individualism score of 80 is an individualistic society, Ethiopia, with a score of 20 is considered collectivistic, and the United States, with a score of 91 is highly individualistic. 7
The purpose of comparing the application of empathic care in a strongly individualistic society such as the United States, to Ethiopia (collectivist) and Hungary (less individualistic than the United States) is to explore the notion of whether knowledge of or experiences of health care practitioner empathic care may be influenced by the country’s specific cultural characteristics. If there are common theme then there emerges an impetus to incorporate empathy more substantively into cultural competency constructs.
Empathy: A Review of the Literature
Empathetic care is an important tool in health care delivery that providers are expected to incorporate into their practice. That said, while the importance of empathy is implied in the National Council Licensure Examination (NCLEX) for Registered Nurses in the U.S., knowledge of how to demonstrate empathic behaviors is not a required competency. 8 However, research has shown that compassionate and respectful care creates a pleasant environment for the health workforce, patients, and families. 9 According to Kerasidou et al 10 the development of empathy constitutes the development of prerequisite skills set for quality health care delivery.
While research has shown that nursing and social worker health professionals recognize the utilitarian value of empathy as an instructive tool in health care settings, it is clear that is has a more accepted place at the table in the field of social work. 11 As King states, “Empathy’s essential nature in the practice of social work is rarely disputed, and empirical study has repeatedly demonstrated its prominence as a significant agent of change in psychosocial intervention efforts.” 12
In a 2000 study of patient clues and physician responses in care settings, the authors concluded that physicians could develop better behavioral attributes to respond to patients’ emotional clues. 13 The study suggests that the utility of empathy has a prioritized functional value, versus a personal, transformative value that is sought to improve one’s caring nature.
Empathy is an active component of cultural competency, which is an umbrella term that delineates the necessity of individuals in caring professions to demonstrate empathic behaviors. As noted by Spector, “It is now imperative, according to the most recent policies of the Joint Commission of Hospital Accreditation and the Centers for Medicare and Medicaid Services, that all health care providers be ‘culturally competent.’” 14 (p. 5). The integration of cultural competency learning objectives into nursing school curriculum is a prioritized component of nursing education. It includes the requirement that nursing students develop cultural awareness traits through the study of transcultural models such as Leininger and Campinha-Bacote. 5
The development of personal empathy and showing humility in the face of the suffering of another person, while an ingredient of cultural competency, is not cultural competency itself. 15 Cultural humility as an active component of cultural competence, cannot take place without the ability to empathize with another human being’s condition. Endemic inequities characterize the U.S. health system and because of that quality care afforded to racial and ethnic minorities requires health care providers to not only have cultural competency but to show cultural humility by “entering a relationship with another person with the intention of honoring their beliefs, customs and values.” 16
It is helpful to consider that while cultural competency requires adeptness in understanding the values and beliefs of another group (a certain educational readiness), empathy requires a level of forgiveness that exceeds the bare practical utility of the value. 17 That is why the minimum standard of understanding patient perceptions or clues to foster improved patient care is not sufficient for a transformative process to address barriers to improved health outcomes.
Empathic behavior is symbiotic with cultural humility. Camphinha-Bacote even proposed a new term for researchers to understand the synergistic dynamic between cultural competency and cultural humility: “cultural competemility.” 15
Review of Bias, Ethnocentrism and Empathy in the U.S., Hungary and Ethiopia
Multicultural societies are interested in the equitable delivery of health care services and resources in patient care. Spector explains that cultural competency implies that “professional health care must be developed to be culturally sensitive, culturally appropriate, and culturally component.” 14 (p. 8) And, as Campinha-Bacote explains, it is a process that continues over a lifetime. 18
Empathy is the antithesis of behaviors associated with cultural insensitivity, which includes bias and ethnocentrism. The concept of ethnocentrism was first coined by Sumner in 1906. 19 He claimed that it was “. . .the viewpoint that one’s ethnic group is the center of everything, against which all other are judged. . .” Other definitions include that of Spector, “The belief that one’s own cultural, ethnic, professional, or social group is superior to that of others.” 14 (p. 268) Implicit biases occur when a specific group or subcultures, such as Black or African American is assigned an (unconscious) negative attribute—such as showing violent tendencies. 20 Implicit bias and ethnocentrism are not mutually exclusive; implicit bias can be the driver of ethnocentric actions that can cause harm in many different contexts, including health care settings, where the risks for the lack of compassionate empathy are higher.
Examples of how bias and ethnocentrism characterize social work and nursing clinical environments in Ethiopia, Hungary and the U.S. follow, specific to those 2 traits. It is followed by a side-by-side country specific table of how empathetic care is viewed.
Ethnocentrism and Implicit Bias in Ethiopia: Ethnic and rural domicile discrimination
In Ethiopia, ethnocentrism is reflected by entrenched political and ethnic loyalties. Since, 1991, Ethiopia has adopted ethnic-based federalism as a constitutional method of governance. It is a “unique form of ethnic federalism that allows ethnically organized states to exercise self-determination, up to and including secession.” 21 The impact of ethnic favoritism, which includes the assignment of key governmental leadership positions and inequitable resource allocation to some degree 21 and a protracted series of large-scale ethnic conflict resulting in civilian deaths, all highlight strong ethnocentric patterns of behavior of the land-locked country, which is located in the horn of Africa. Because of institutionalized patterns of ethnocentrism, members of ethnically labeled unfavored groups can anticipate inferior health care. These factors, particularly the recent genocidal pattern, have become alarming among political scientists, who view the country as suffering from ethnocentrism. Nonetheless, there is insufficient evidence to cull from numerous health care environments where providers interact daily with patients or clients in major cities, and where several ethnic groups may reside at 1 time.
As is the case in many African countries, much of the country’s wealth resides in urban areas (where modernized health centers exist). The disproportionate spread of resources forces rural dwellers to journey to urban areas for better treatment. Research shows discrepancies in patient perception of the quality of care between rural and urban dwellers with urban patients reporting a higher satisfaction level than patients in rural areas, who report biased treatment. 22 Urban patients, it is noted, have a greater abundance of wealth, and are better educated, which fuels instances of implicit bias.
Research shows inequities in rural versus urban health service utilization 23 and discrepancies associated with rural/urban members access to care.24,25 In addition to urban/rural bias, there is bias associated with lifestyle. One study revealed that medical professionals display both explicit and implicit bias against people living with HIV, which has led to higher levels of stigma and discrimination. 26
Examples of Ethnocentrism and Implicit Bias in Hungary: Ethnic and Racial Discrimination
There are various specific examples of ethnocentrism and explicit bias in Hungary, which are largely associated with societal treatment of the Roma people.
In 2 Hungarian towns, ethnocentrism against Roma people was measured with a general ethnocentrism scale that consisted of 14 items with questions rating how sympathetic or antagonistic they find a specific racial (eg, Gypsies, Poles, Austrians), cultural (skinheads, homosexuals), or political (either extreme leftists or extreme rightists) group to be. 27 The study found that negative attitude toward Gypsies correlates with a general ethnocentric orientation. Among the youth, parental prejudice and authoritarianism were significant direct predictors of anti-Gypsy prejudice negative attitudes toward Gypsies.
Other examples of ethnocentrism in Hungary include the fact that a larger proportion of Roma children are placed in schools for the mentally disabled, suggesting that the ethnicity of the individual is a factor in cognitive competency. There is an underreporting of racially motivated crimes; roughly 40% of trafficked people in Hungary are Roma and there are higher than average gender-based domestic violence incidents involving Roma Hungarian people. 28
Whereas ethnocentrism characterizes the examples above (where an explicit belief in the superiority of a specific ethnic group (non-Roma Hungarians) is the driver of harm toward others), implicit biases are associations that are learned, which may even be unconsciously applied in some situations. Examples of implicit bias in Hungary include underlying negative factors associated with housing discrimination against the Roma people. This could take the form of separated villages or “ghettoized” neighborhoods in cities. 28 Additional examples include instances of unconscious bias against the cognitive capabilities of Roma children and Roma perceptions of inferior health care, leading them to avoid medical care, unless their condition is serious.
Examples of Ethnocentrism and Implicit Bias in the United States
While it can be perpetrated against any group in the United States, ethnocentrism is most closely tied to the historical institution of slavery, which not only cruelly dehumanized a subpopulation of individuals, but which also, post-slavery, systematically denied a group of people educational, civil, and social rights and status. Research shows that many white Americans are substantially influenced about their viewpoint on race on the basis of some level of ethnocentrism and prejudice. 29 More recent research on U.S. ethnocentrism explores how its tentacles are more adversely far reaching than originally understood. For example, Kuey 30 examines how social group allegiances gone rogue can have damaging psychological impact and how an acceptance of dominant social power is the catalyst to individuals committing dehumanizing actions.
How power is inappropriately used to erect barriers to empathic behaviors is applicable to all 3 countries, particularly with respect to the adverse impact of ethnocentrism. If ethnocentrism were a hammer, implicit bias would be a nail. In the U.S., racially tinged ethnocentrism has historically had deleterious mental and physical health on specific populations, particularly those who are black and brown.
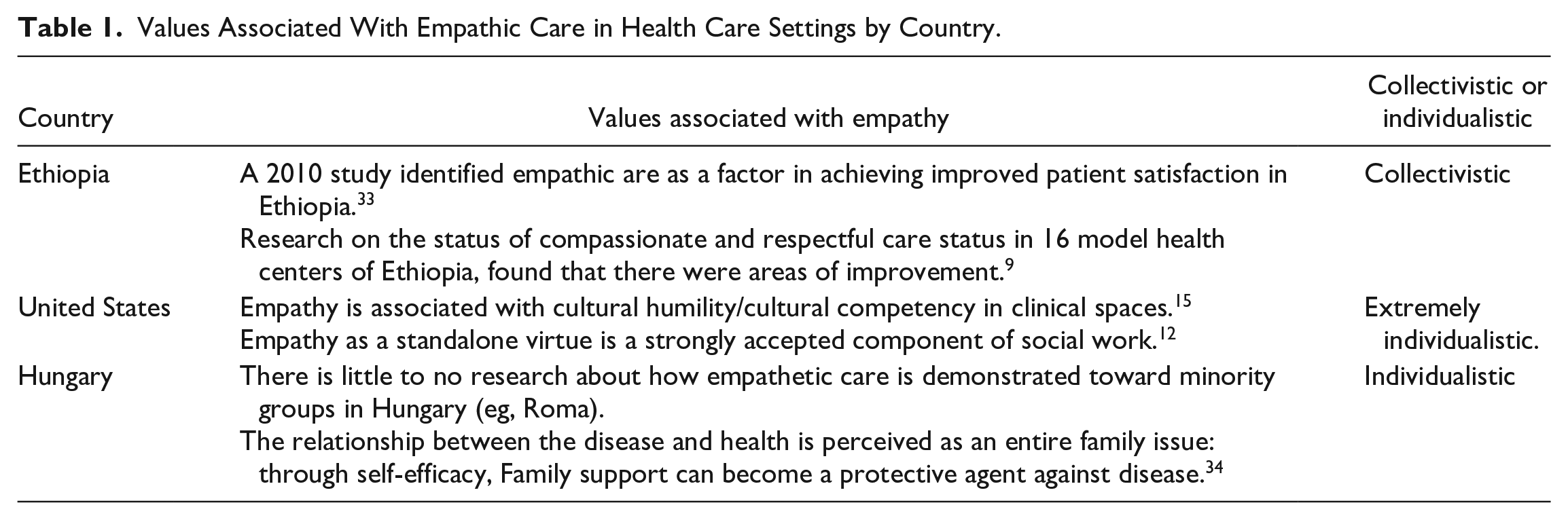
Black American men have most notably been the most negatively impacted by implicit bias. They have—as a result of bias and ethnocentrism—incurred stress-related illnesses, related to persistent fears of police brutality or police related dehumanization, resulting from bias (Table 1).31,32
Values Associated With Empathic Care in Health Care Settings by Country.
Conclusions
A common theme that prevents countries from providing health care support to the vulnerable and oppressed is the lack of empathy toward those people. It should be a wake-up call to us all. In all 3 countries there are lessons to be learned.
Hungary is an individualistic culture. However, there is still a strong bond among family members. Traditionally, people are expected to put the interest of their family or group where they belong before their own interests. Those Hungarian ethnocentric attitudes made toward the Roma subpopulation is similar to those racial and microaggressions shown toward ethnic minorities, particularly Black and Hispanic people, in the United States.
Ethiopia, which is a multiethnic collectivistic nation, aspires to fulfilling the country’s group obligations, but is held captive by the unequal distributive allocation of health delivery, based on ethnic conflict and income disparities. The existential threat of a protracted war in Ethiopia, given its current model of skewed resource allocation based on ethnicity, would only further divide individuals based on their membership in a specific “group,” rather than prioritize the group over the individual, which would be the norm in a collectivistic society.
The fluid nature of characteristics related to the cultural dimensions of these 3 countries—collectivistic versus individualistic—underscores the complexity of identifying countries that are either more or less inclined to adopt and incorporate greater empathic behavioral care models in professional nursing and social work environments.
This paper has shown that many of the barriers that prevent a full expression of empathy among health care providers are common across cultures and, in the United States, that is a lesson that must be heeded. The prejudicial nature of housing discrimination toward the Roma in Hungary, for instance, is very similar to the redistricting process to create new voting districts that are detrimental to Black voter freedom. Empathy can be employed as a key to unlock those doors. Similarly, the lack of access to and quality of care available to rural Ethiopians mirrors inequities faced by low-income minorities and rural dwellers, regardless of ethnicity, in the U.S.
A new paradigm that squarely positions empathy as a trainable competency for nursing and social work students is called for. Moreover, it should be one that takes into account shared cultural themes related to barriers to care and concepts for greater expressions of cultural sensitivity and empathic, humanistic care.
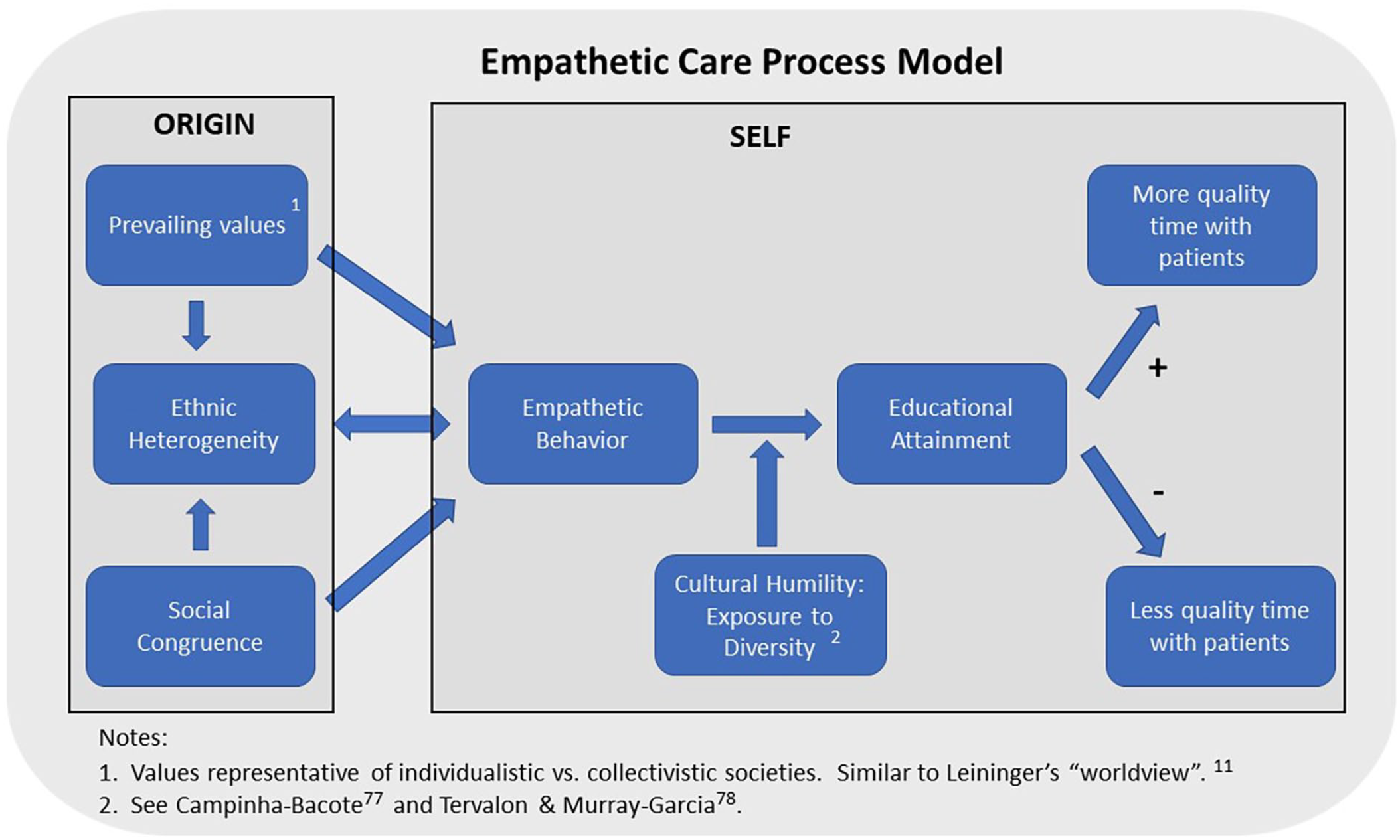
A unique model (The Empathetic Care Process Model) is introduced in this paper as a conceptual tool to explore the process of the development of empathy in a provider. This model is not meant to replace former theoretical models that have been foundational in articulating a framework for nursing research, such as Reifsnider et al. and Bronfenbrenner.35,36 Its purpose is to present a cultural competence conceptual framework that explains the process by which a health care provider’s active identification with the suffering of individuals who are marginalized will, combined with health knowledge, result in improved quality of care and improved health outcomes.
The empathetic care process model.
This paper set out to examine whether a comparison of culturally distinct countries can illuminate the role of empathy as a neglected but vital component of cultural competency and, if so, whether there is value in highlighting empathic behavioral training as a required competency in nursing and social work educational institutions. A specific limitation of this study is that it was confined to an analysis of 3 countries, all democratic.
The authors believe that greater investigation of the value of healthcare provider training in empathic behaviors is urgently called for, as a tool to bridge pervasive unmet gaps of care within culturally diverse environments.
It is believed that, given increasing global health threats, greater focus on health care provider training in empathy will complement the current toolbox for the promotion of culturally competent care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.