
Abstract
Introduction/Objective:
Venous Leg Ulcers (VLU) present a challenging healing process. Attaining healing is a primary treatment objective, commonly pursued in Primary Health Care (PHC) or Specialist Wound Management Clinics. Our objective was to examine the association and interplay between sociodemographic, health, clinical, and care factors with the outcomes of VLU treatment in patients undergoing care at a Specialist Wound Management Clinic.
Methods:
Longitudinal, observational study took place in a center for the treatment of chronic injuries linked to PHC. The sociodemographic aspects, health status and habits, clinical and care aspects of patients with VLU were scrutinized over a 1-year period.
Results:
The sample comprised 103 participants, with some still under treatment (Treatment Group—TG/ n = 60) and others having achieved VLU healing (Healing Group—HG/ n = 43). An association between sociodemographic, health, clinical, and care factors and the healing outcome (HG) was identified. A moderate correlation was observed between factors predisposing to healing in the sociodemographic group and health habits. Notably, among sociodemographic factors, the older age group and improvements in health, particularly the reduced use of alcohol/smoking, appeared to exert the most significant influence on healing. Additionally, specialized service monitoring and the application of compression therapy were contributory factors.
Conclusions:
These findings substantiate the hypothesis that sociodemographic, health, clinical, and care-related aspects are intertwined with VLU healing. Protective factors associated with healing interacted synergistically, fostering a positive outcome over one year of treatment.
Introduction
Venous Leg Ulcers (VLU) challenging wounds to heal, predominantly affecting the lower limbs and stemming from chronic venous insufficiency. Recognized risk factors include obesity, genetic predisposition, a history of deep vein thrombosis, and advanced age. 1 Approximately 70.0% of skin wounds are estimated to be VLU, requiring specialized care and often persisting for years until complete healing. 2 This condition poses a global public health concern, evident in various regions such as the United States of America, Europe, the United Kingdom, and Africa.3,4 A population study revealed a higher incidence of superficial venous disease among Hispanics (3.6%), followed by Asians (1.5%), and African Americans (0.9%). 5 In Brazil, the profile of VLU patients mirrors that of other global scenarios, predominantly affecting women and the elderly, with considerable potential to impact quality of life across biological, social, and economic dimensions.6,7
In 2002, the Brazilian Ministry of Health released the Manual of Conduct for Neurotrophic and Traumatic Ulcers, advocating for a comprehensive treatment approach that encompasses continuous evaluation of clinical, biopsychosocial, health, and nutritional status. 8 Internationally, the Clinical Etiology Anatomy Pathophysiology (CEAP), updated in 2020, establishes criteria for assessing vascular disease severity, considering clinical signs, venous disease etiology, depth, and pathological conditions related to obstruction or reflux. 9
Despite previous evidence highlighting the influence of sociodemographic, cultural, clinical, and care-related factors on VLU prevalence in Brazil and other countries,6,10 -13 there has been limited recent research on how these factors impact healing. Therefore, it is crucial to revisit and analyze this relationship to propose effective measures favoring improved outcomes. An evaluation within a specialized service can shed light on key factors influencing treatment outcomes. To address this gap, this study aims to examine the association and interplay between sociodemographic, health, clinical, and care factors with the outcomes of VLU treatment in patients undergoing care at a Specialist Wound Management Clinic. Our study hypotheses posit that (1) these factors are associated with VLU healing and (2) protective factors related to VLU healing interact synergistically, contributing to positive outcomes.
Methods
This is an observational, longitudinal study utilizing the cluster analysis method with a quantitative approach, conducted with patients with VLU who received follow-up care in a service specialized in the treatment of chronic wounds. The service was affiliated with 29 Brazilian Primary Health Care (PHC) units and took place between August 2020 and November 2021. Adhering to the principles outlined in the Declaration of Helsinki on good scientific practices, this research was submitted and approved by the Research Ethics Committee of the Federal University of Rio Grande do Norte, under opinion No. 2156068. Prior to the administration of any instruments, the study’s purpose, risks and benefits were explained to the participants, who then provided by signing a written form to signify their acceptance of participation in the study.
The target population encompassed individuals with active chronic VLU receiving care in PHC. In this context, active VLU were defined as those wounds that had remained open for at least 3 months without healing. A non-probabilistic sample was obtained for convenience. Before data collection, the study region recorded 157 patients with VLU under treatment. Based on this population count, the sample calculation was performed, adopting a confidence level of 95% and a margin of error of 5%, which resulted in an estimate of 112 participants. However, a total of n = 103 subjects completed the study. The calculation employed an online formula of quantitative variables for finite populations using an online calculator accessible at: https://calculareconverter.com.br/calculo-amostral/. Inclusion criteria for participation in the study stipulated that participants should be 18 years of age or older, registered in any PHC unit covered by the service, and present with at least one active VLU. Exclusion criteria encompassed individuals with completely healed VLU (prior to the study initiation), those who missed consultations for more than 1 month, those who passed away, or those who changed their residence to an area outside the coverage region following the first data collection. Patients with leg wounds of mixed or non-venous origin were also excluded; for this study, leg wounds of mixed or non-venous origin were defined as arterial ulcers or those that, in addition to venous etiology, presented arterial impairment. 14 The determination of the wound etiology was carried out with the assistance of the CEAP. 9
Data collection occurred through face-to-face interviews format, at 2 times within the specialized service office. The initial collection (T1) took place between August and October 2020, and the second (T2) between September and November 2021, by a team composed of master’s and PhD graduate students in health sciences, one physician and 2 nurses who were previously trained. The follow-up consultations took place at most every 7 days by prior appointment, in which the primary dressing of the VLU was changed by a nurse, who evaluated the change of the wound with the general practitioner. It was mainly the compression therapy with Unna boot, considered the gold standard for VLU treatment. The product consists of a bandage that measures 10.2 cm in width and 9.14 m in length, which can be cut depending on the desired size. It is had a visual gradation that allow the measurement of the compression level applied to the VLU at the time of boot application. The compression level was determined by the medical professional overseeing the treatment. Its composition is zinc oxide, glycerin, distilled water, and gelatin. 8 A vascular specialist from the department conducted a comprehensive assessment of the patient before commencing treatment. This assessment included the measurement of the Ankle-Brachial Index, an internationally validated calculation for assessing obstructive diseases. In the context of the research, it served as an aid to rule out obstructive arterial disease and, consequently, provide greater security for the indication of compression therapy. 15 The clinical aspects of the wound were assessed according to the measurement of its extent, depth, and characteristics of the edge and lesion bed, as recommended by the protocol used in Brazil, 8 akin to internationally accepted scales. 16
A sociodemographic, health, clinical, and care aspects characterization form was applied structured with closed questions and divided into response categories. This instrument was prepared by the researchers themselves and resulted in the evaluation of 4 aspects: “Sociodemographic Aspect,” “State and Health Habits,” “Clinical Aspect of VLU,” and “Assistance Aspect of VLU.” From the characterization of each of the aspects, we divided the sample into 2 groups according to their outcomes after a minimum interval of one year (T1-T2): the group of those who were still undergoing VLU treatment, called the Treatment Group (TG) and the group composed of those who had healed VLU: Healing Group (HG). All study variables were analyzed following this division. Some information collected in the initial assessment (T1) was solely based on patient reports. Therefore, the diagnosis of diseases in some participants was only confirmed during the second assessment (T2) following medical evaluation.
Additionally, we created a group of scalar variables called Predisposing Factors for VLU Healing (PFH). This group of variables involved those specific characteristics that, according to the theoretical framework adopted, favored the healing of VLU. Thus, the number of characteristics of each aspect was converted to a scale from 0 to 100. For example: if an aspect was composed of 10 characteristics, an individual who presented 7 of them would have a scalar score of 70), followed by the same proportionality for all aspects. The characteristics of each aspect are listed below:
Sociodemographic Aspects
Group of male individuals, with partner, without profession, own housing, age group up to 59 years, high education (university education), income above a minimum wage (7 characteristics). For education level, we considered: low: high school or less; hight: higher education or higher. The minimum wage in Brazil in the year 2021 (T2) was BRL 1 100.00 (approximately USD 205.00).
Health State and Habits
Participants with no history of Systemic Arterial Hypertension (SAH), Diabetes Mellitus (DM) or neoplasia, no use of alcohol/smoking, no allergies, no use of medications, normal eliminations (without constipation or incontinence), adequate body hygiene (one or more baths per day), normal mobility (without any difficulty in mobility) and no mental problems noted (10 characteristics).
Clinical Aspects of VLU
Patients without recurrence (in the last 6 months), without edema (no hyperemia and increased volume in the wound region), without odor, wound site in the middle/upper third of the leg, little exudate or lymphedema (dirt visible only on the primary bandage) and serous type or lymphedema, smooth and hydrated skin, and edge and bed of the wound without conditions such as the presence of fibrin and/or liquefactive or ischemic necrosis or non-viable granulation (9 characteristics).
Assistance Aspect of VLU
Place of treatment (residential or health service), people with an open wound for less than 6 months, treatment in a specialized service, change of dressing by trained people, use of compression therapy and blood, urine and imaging tests with Doppler (8 characteristics). As a theoretical framework for the definition of these factors as predisposing to healing, we adopted the Manual of Conduct for Neurotrophic from Brazil. 8
Data Analysis
The collected data were tabulated in a database, using the Microsoft Excel 2019 software (Microsoft Corporation, Washington, WA, USA). Then, they were transferred and analyzed in the Statistical Package for the Social Science (SPSS) version 21.0 (IBM, Armonk, NY, USA). We performed the Kolmogorov-Smirnov normality test, which identified the non-normality of the sample. Pearson’s Chi-square test was used for the variables of Sociodemographic Aspect, State and Health Habits, Clinical Aspects of VLU and Assistance Aspect of VLU, in T1 and T2, data from which absolute and relative frequencies were extracted. The Mann–Whitney U test was used for the descriptive analyses of mean, Standard Deviation (SD ±) and percentiles of the PFH. The Signal Test was performed to compare the scores between the 2 moments of data collection for the PFH, classified as “improvement,” “worsening,” and “equal.” We also calculated the correlation between the PFH variables, using the Spearman correlation test (r). Therefore, we adopted as a parameter for the correlation strength: r < .29 (weak); 0.29 > r < .49 (moderate); r > .50 (strong). After the analyses, the data were organized into tables, with their percentage distributions and significance of the tests. A significance level of 5%, confidence intervals of 95% was considered and a P-value < .05 was considered statistically significant. 17 The data that support the findings of this study are openly available in the Mendeley Data repository at https://data.mendeley.com/datasets/7gcj3z46pc/1, reference 10.17632/7gcj3z46pc.1.
Results
Of the 157 patients registered in the PHC of the study site, 45 were not found in their registration addresses in the unit (before T1). Thus, the initial study sample was 112 participants. During the follow-up, 6 were excluded due to death and 3 due to change of address outside the service coverage region. The final sample was n = 103 individuals, of whom n = 43 (43.7%) evolved to healing after one year of treatment (HG). The complete sample recruitment and selection process is described in Figure 1.

Sample recruitment and selection process flowchart.
Table 1 shows the sociodemographic characterization according to the study groups in both moments (T1–T2). The most significant difference between the groups was found in the age group variable, in which the older participants (>60 years) were the majority in the HG in T1 (n = 31/72.1%/ P = .004) and T2 (n = 32/74.4%/ P < .001). In the other variables, both groups showed similarity in their profiles.
Characterization of the Sociodemographic Aspects of the Participants According to the Study Groups.
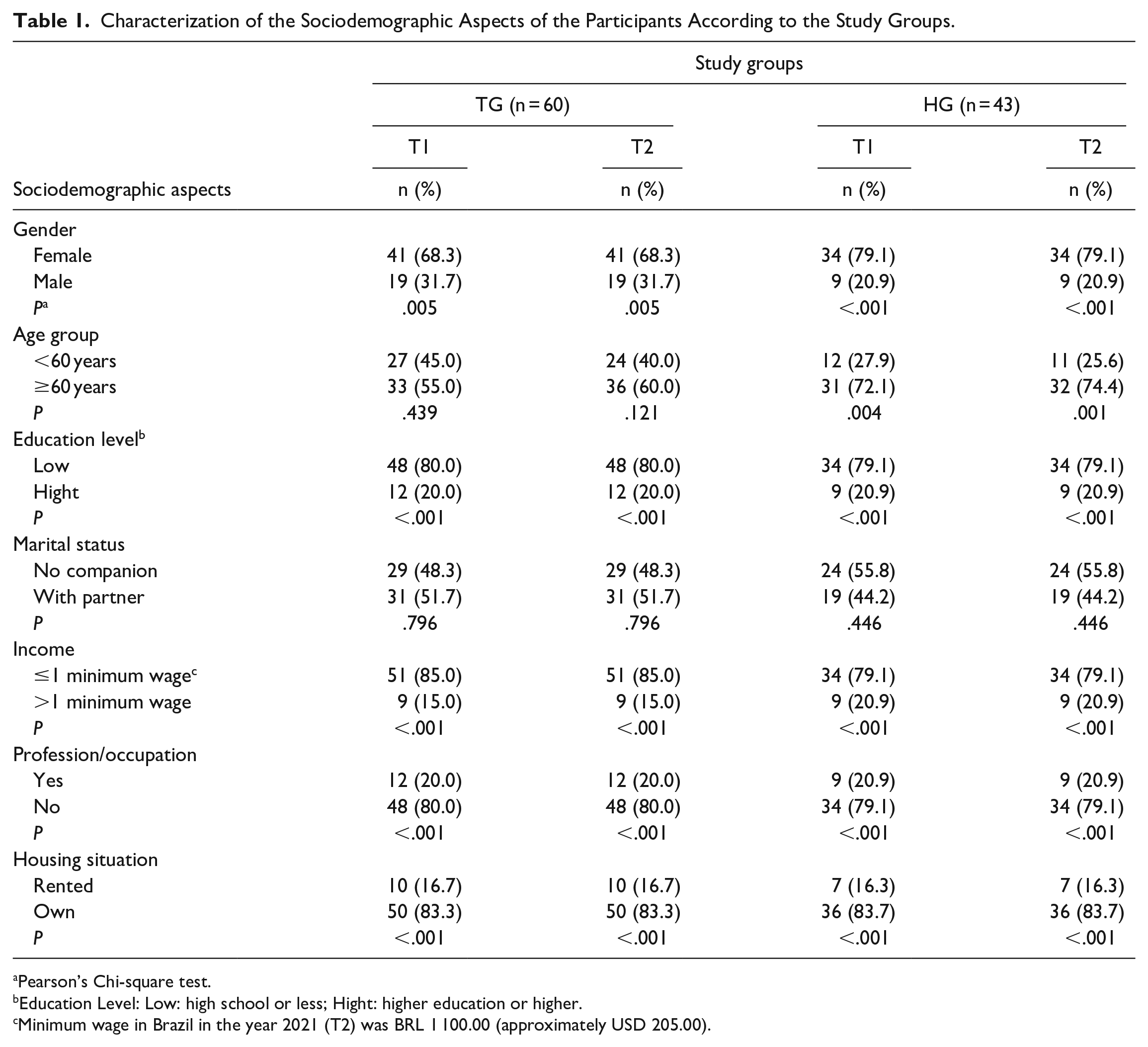
Pearson’s Chi-square test.
Education Level: Low: high school or less; Hight: higher education or higher.
Minimum wage in Brazil in the year 2021 (T2) was BRL 1 100.00 (approximately USD 205.00).
Table 2 shows differences in the behavior of both groups regarding health status and habits. In general, it is clear that the TG exhibited a greater predominance of diseases and habits considered predisposing to a worse outcome, according to the theoretical framework we adopted. Arterial hypertension, for example, was predominant in this group, in which we found an increase in the diagnosis at the time T2 (n = 45/75.0%/ P < 0.001). We also observed a reduction in use of alcohol/smoking in both groups. However, the reduction was more intense in the HG, in which there was a frequency variation from T1 (n = 14/ 32.6%/P = .022) to T2 (n = 3/7.0%/p < 0.001).
Characterization of the Health Status and Habits of Patients With Venous Ulcers According to the Study Groups.

Pearson’s Chi-square test.
Consume alcohol or tobacco twice a week or more.
Constipation or incontinence.
Regular.
Not bathing regularly.
One or more baths per day.
Any mobility difficulties.
Without any difficulty in mobility.
Any medical diagnosis of mental change.
No mental problems noted.
When analyzing the outcome of clinical aspects in the study groups, we highlighted those that indicated an increase in clinical signs related to the worsening of VLU in the TG, such as the presence of purulent or bloody exudate, while there was a reduction in the HG. Similar behavior was observed in the Odor variable. As for the edge and bed of the wound, both groups showed increased signs of worsening between T1 and T2. However, the increase was substantial in the TG (Table 3).
Characterization of the Clinical Aspects of Patients With Venous Ulcers According to the Study Groups.

Wound reopening in the last 6 months.
Pearson’s chi-square test.
Apparent dirt on the secondary bandage.
Dirt visible only on the primary bandage.
Hyperemia and increased volume in the wound region.
Area around the wound with scaling, hyperemia or deformities.
Presented conditions that hindered healing, such as hyperemia, elevated edges, presence of scaling/maceration, and keratosis.
Without elevation and without alterations.
Conditions such as the presence of fibrin and/or liquefactive or ischemic necrosis; non-viable granulation
Viable granulation and/or epithelialization.
In Table 4, in relation to care aspects, it is possible to highlight that all patients started to have follow-up in health services. Attention is drawn to the changes in relation to who changes the dressing. In both groups, many of the patients themselves underwent the procedure or it was done by an untrained person. The use of compression therapy also exhibited an increase in its adherence between T1 and T2.
Characterization of the Care Aspects of Patients With Venous Ulcers According to the Study Groups.

PHC or Hospital.
Pearson’s Chi-square test.
When analyzing the intergroup association considering the presence of PFH (Table 5), we observed that the variable of clinical aspects exhibited a change in the profiles of both groups between T1 and T2, being significant at the last moment (P < .001). In this variable, we found a slight increase in the TG score and a significant increase in the HG. Regarding care aspects, we found that in T1 the groups had significantly different aspects (P = .006), but that after attracting PHC patients to the specialized service, the profiles were similar (P = .682).
Characterization of the Study Groups in View of the Factors Predisposing to the Healing of Venous Ulcers.

U of Mann-Whitney Test.
Table 6 shows the change related to the improvement, worsening or maintenance of the amount of PFH. When comparing both groups, we noticed that the HG showed a significant improvement in the Health, Clinical and Care aspects. Despite the predominance of improvement in the TG in all aspects, this did not occur significantly, with the exception of the Health PFH (p<0.001). The summary of these findings is depicted in Figure 2.
Change of Venous Ulcers Considering the Factors That Predispose to Wound Healing, According to the Study Groups.

Signal test.
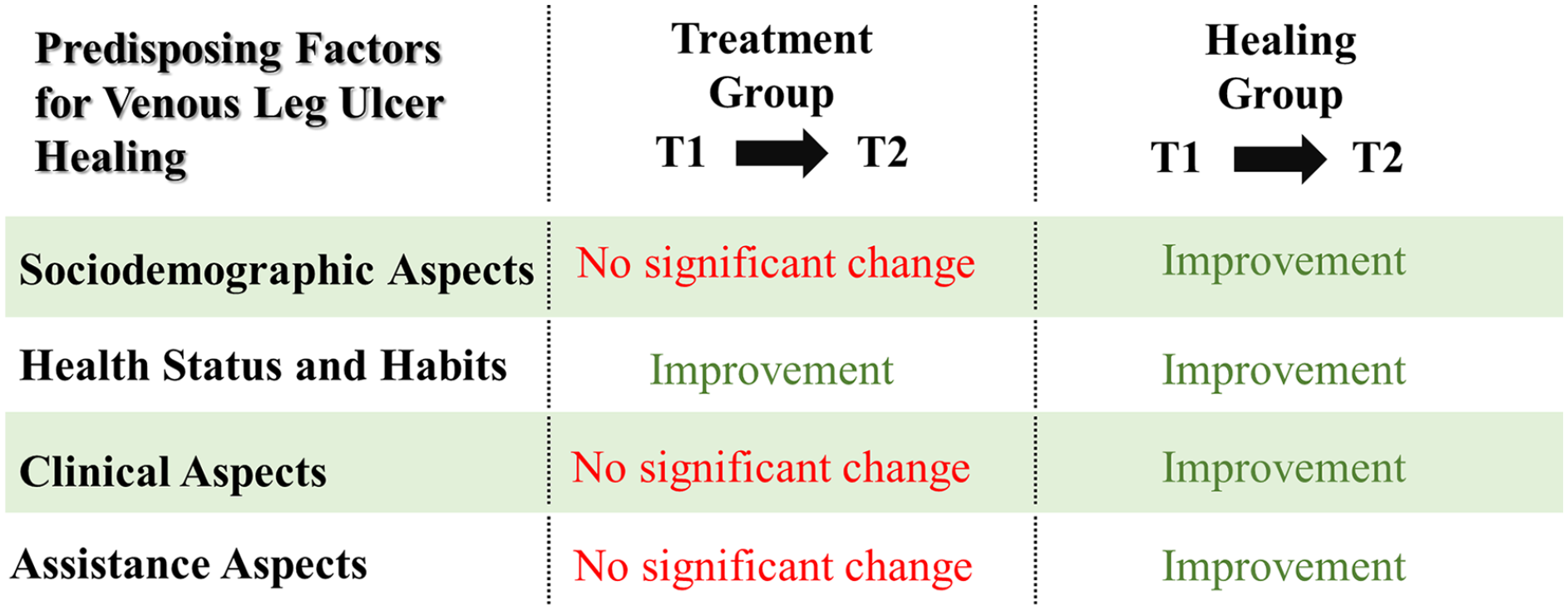
Summary of the changes identified in the Predisposing Factors for VLU Healing (T1-T2).
Additionally, we calculated the correlation (r) between all PFH variables to ascertain any interaction between them. We found a moderate and significant correlation between sociodemographic and health aspects only in the HG (r = 0.36/P = .017). The other crosses did not demonstrate any relevant correlation.
Discussion
We found in our study that the sociodemographic, health, clinical, and care aspects of patients with VLU were associated with wound healing after one year of treatment in a specialized service. We also showed that sociodemographic PFH and aspects of health and life habits were correlated in the outcome of healing. Specifically among the sociodemographic factors, the age group of people over 60 stood out the most. As for health status and habits, the reduction of use of alcohol/smoking seems to have been the most decisive for healing. Follow-up in a specialized service along with the use of compression therapy with Unna boots were the aspects that most stood out within the care criteria.
Concerning the sociodemographic profile, our findings indicated a stronger correlation between healing and age group over 60 years of age stood out, with a higher predominance of individuals in this age group in the HG, while the TG did not show a predominance of any of the age groups. Although clinical guidelines on VLU point to increasing age as a factor that can impair the closure and healing of the wound, 18 this result can support the thesis that treatment in a specialized service with the use of compression therapy was effective, even with the presence of this important risk factor. In Brazil, individuals aged 60 years or older are considered elderly people, who experience physiological changes in this age group that can also negatively interfere with the treatment of several diseases. 19 Added to this context is the evidence in our studies that sociodemographic aspects correlated with those related to health status and habits.
Regarding these health aspects, most participants in our sample reported the presence of SAH and DM in both groups. However, we observed that the HG showed lower proportions, which may have disadvantaged an outcome for the TG when comparing them. We also found a behavior that seemed controversial, since between T1 and T2 there was an increase in patients with SAH in both groups, while the presence of DM decreased, even though they were diseases presumably without cure. Regarding these findings, it should be noted that the information was given by the patient himself and that many of them did not have a formal medical diagnosis of these diseases at the time T1, but that after being followed up in the specialized service they were able to perform tests that confirmed or discarded this diagnosis. We noticed more prominently that there was a reduction in use of alcohol and smoking among the participants of both groups between T1 and T2, being more noticeable in the HG. The reduction of use of alcohol and smoking is already known in the literature as an important factor for the improvement of several clinical conditions, including venous insufficiency, which causes VLU. 20 However, it should be noted that changing other habits such as better diet and physical activity are equally relevant for a better outcome in VLU treatment 21 and data on diet and physical activity were not investigated in our study.
Mobility was also an element of the health aspect that showed significant improvement in the HG. However, it should be noted that this group was the one that most adhered to the treatment with Unna’s boot. Regarding this therapy, clinical studies indicate efficacy in the treatment of VLU, specifically favoring a better mobility of the affected limb, helping to protect against infections and resulting in a venous return closer to the physiological one,22,23 since that the properties of the compressive are maintained, estimated at up to 7 days for each application. 24 Individually, adherence to this treatment in the HG between T1 and T2 seems to be one of the most decisive factors for healing in our study. A literature review identified that a thorough diagnosis followed by appropriate treatment of compression therapy can result in substantial improvement in outcome, with a cure rate of up to 67.0% at 12 weeks and up to 81.0% at 24 weeks. 25 However, those who had healed their VLU in our study represented less than half of the sample studied.
Although there is no correlation between the PFH variables of the clinical and care aspects, it is noteworthy that for this analysis, we considered a set of care characteristics, and not only that of compression therapy. In addition, it is important to clarify that the Unna boot should be used in VLU in its earliest stage, when the VLU is smaller and dry. 18 However, most of the individuals in our sample from both groups had already been on the treatment for more than 6 months. In this regard, the authors indicate that the time of wound greater than 3 months is an important predictor of poor prognosis 18 and even so, the HG showed good results, which makes us believe that a more active PHC screening could have improved these results. Both groups were predominantly located in the malleolar region, data similar to a study carried out with Colombian patients, in which 41.2% of those involved had an wound located in this region, considered as a risk factor due to the proximity to limb joints, which, in turn, makes it difficult to immobilize the tissue adjacent to the VLU and favors its recurrence, 26 which was quite frequent in the TG.
Despite this, we observed improvement of VLU in almost all clinical aspects evaluated between T1 and T2, in both groups. However, we recognize that the treatment previously initiated by some participants in the sample, to the detriment of others who were not accompanied by the service, may have hindered more reliable evidence about it. Study highlighted that the performance of trained and qualified professionals in the monitoring, performance and guidance of the VLU dressing was decisive for a greater possibility of healing. 26 In our results, we observed an increase in patients who changed their own dressing or received help from a family member or a person not qualified to do so, in both groups. This seems to support the thesis that, even if there is no technical training for the procedure, patients can be well oriented regarding basic care in changing the dressing. However, it is noteworthy that the exchange performed by untrained people was limited to the secondary dressing. That is, the one that covers Unna’s boot that does not require greater knowledge of who performs the procedure. Even with favorable results for the HG, we observed that many participants in the TG did not experience improvement or maintained the same health and care aspects between T1 and T2. This observation might elucidate the reason why, despite the implementation of compression therapy, the TG did not attain the same positive outcome as the HG. Moreover, it is explained in the literature that the exclusive reliance on treatment alone does not ensure the healing of VLU unless individuals embrace behavioral and self-care changes. 7
As a limitation, we point out the fact that some patients were already on treatment before the start of the study. This may have interfered with the evaluation of the outcome, as some started to be treated only after T1. Furthermore, the predominantly used treatment with the Unna boot alone cannot explain the success in the healing of the HG, as several aspects may have influenced the outcome. The information regarding diagnoses of chronic diseases was only confirmed during the second assessment (T2). This had a detrimental impact on certain outcomes. We also did not reach the number of participants indicated by the sample test, which may have compromised the replication of the study in other scenarios.
Conclusions
It was possible to emphasize the association between the sociodemographic, health, clinical and care aspects of patients with VLU with the outcome of wound healing after one year of treatment in a specialized service. These results allowed us to support our primary hypotheses but suggest an improvement in the literature of randomized trials and clinical trials in which the efficacy of other therapies recommended for VLU can be compared. Particularly in developing countries like Brazil, it becomes crucial to understand the cost-benefit analysis of investing in promising treatments. This knowledge can guide the formulation of public policies targeted at individuals at risk of developing VLU.
Footnotes
Acknowledgements
We especially thank all the patients who agreed to participate in the study, as well as the professionals working in the services involved that made up the study services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Council for Scientific and Technological Development (CNPq), Brazil. Funding was obtained through CNPq/MCTI/FNDCT Call No. 18/2021 – Range B – Consolidated Groups, under grant number 0257801662000850. The grant was directed to the general coordinator of the research PhD. Gilson de Vasconcelos Tores to enable the execution of the research.