
Abstract
Introduction/Objectives:
The COVID-19 pandemic has long-term implications for adult health and function, whether or not people were infected with the disease. Although cognitive disruptions are among the major symptoms of COVID-19, most research focused on managing medical symptoms, such as respiratory symptoms or pain. Thus, less is known about the pandemic’s long-term implications for assessing functional cognition. This study aimed to examine COVID-19’s effects on community-dwelling adults’ functional cognition and health, comparing gender differences.
Methods:
This cross-sectional study divided 118 community-dwelling adults (25 previously infected with COVID-19) into gender groups. Primary outcome measures included the Daily Living Questionnaire (DLQ) and short form health status survey, SF-12.
Results:
No significant differences were found in functional cognition or health between participants who had contracted COVID-19 and those who remained healthy, but men had better functional cognition and health measures in comparison with women.
Conclusions:
Gender differences in functional cognition and health state may relate to gender-based family roles. It is essential to assess functional cognition of young adults who were exposed to a pandemic, such as COVID-19, because it may significantly affect their health and functional status. The DLQ is a reliable, valid assessment of functional cognition that may suit individuals who previously contracted COVID-19.
Introduction
COVID-19 severely affected the health of millions of people globally. 1 Lockdowns and societal disruption from the pandemic upset social norms and affected physical and mental health worldwide. Although the mandatory restrictions slowed the virus’s spread, 2 they had serious implications for human functioning 3 —requiring immediate, significantly changed life routines and restructured daily activities. 4 Long-COVID syndrome 5 refers to COVID-19’s long-term effects. The most common Long-COVID symptoms include fatigue (58%), headache (44%), neurocognitive symptoms like attention and memory disorders (27%-40%), hair loss (25%), and dyspnea (24%). 6 About 50% of individuals with long-COVID experience symptoms affecting their ability to return to previous occupations and their quality of life for at least 6 months after acute infection onset. 7 Although Long-COVID is defined as symptoms appearing after acute COVID-19 infection, it may also have a social construct, not emerging out of pathological impact of the virus but as response to public health management of COVID-19 pandemic (ie, lockdowns, daily life restrictions, and job losses).
This study focuses on functional cognition and health during the COVID-19 pandemic. Functional cognition is a relatively new term for the cognitive ability to complete complex everyday tasks. 8 Regardless of their illness severity, people who recovered from COVID-19 widely reported cognitive disruption, such as fatigue, memory loss, multitasking impairments, brain “fog,” and difficulty recalling words.5,9,10 Although more studies are required to understand COVID-19’s full impact, lessons from other viruses and conditions indicated that severe respiratory conditions, such as acute respiratory, acute respiratory distress, or Middle East respiratory syndromes, lead to changes in functional cognition. 11
These cognitive effects can substantially constrain a person’s ability to perform complex tasks involving functional cognition, such as instrumental activities of daily living (IADL).9,10 In Jaywant et al’s 12 acute rehabilitation study, 81% of severely unwell patients had mild to severe cognitive impairments, most in attention and executive functions post-COVID-19. Zhu et al’s 13 sample of young adults discharged after acute hospitalization, 36.81% manifested difficulties in at least 1 IADL, and 16.44% needed at least moderate support in basic daily activities. Walle-Hansen et al 14 showed evidence of decreased ADL and mobility functions, negative cognitive-functional changes, and higher pain levels among a population of older adults 6 months after hospitalization for COVID-19.
The World Health Organization 15 defined health as a perfect state of physical, mental, and social well-being and not merely the absence of disease. They based human functioning on body functions and structure, activities, and participation. 16 According to the international classification of functioning and disability (ICF), a key taxonomy for health professions, health is the dynamic interaction between an individual’s functioning and their restrictions and limitations in each context. 17 This taxonomy can help identify features that explain the activities and participation of individuals exposed to the COVID-19 pandemic since its outbreak and environmental factors that enable or restrict their return to participation in life. 18
This taxonomy categorizes cognition—the mental process involved in knowledge, learning, and applying information to everyday tasks—under body functions and structures and describes it as necessary for human functioning. 19 The best way to evaluate functional cognition is to assess an individual’s overall abilities, including their use of strategies, routines, habits, and contextual and environmental resources, in actual task performance, 20 considering their capacity to perform those tasks.20,21 Although several assessment tools have been developed to evaluate functional cognition, they require further validation for COVID-19.
The Daily Living Questionnaire (DLQ)22,23 is based on the dynamic interactional model, a highly efficient perspective for examining daily functional cognition. The DLQ assesses challenges that people with cognitive disabilities face in everyday functioning. Its 2 parts reflect key dimensions affecting an individual’s state of health as defined by the ICF: body functioning and activity/participation. For the assessment of health status, which is defined by the ICF under personal factors we used the SF-12 health status survey (Figure 1).

COVID-19 assessment based on the international classification of functioning, disability, and health. 16
This study also focuses on gender differences in functional cognition and health during the COVID-19 pandemic. Many recent studies showed evidence of COVID-19’s negative impact on emotional states, such as exacerbating stress symptoms and heightening anxiety, depression, loneliness, and social functioning difficulties (eg, Pieh et al 3 and Pfefferbaum and North 24 ). Fiorenzato et al 25 reported the issue’s gender differences, showing that women, especially those under 45 years and underemployed or working from home, were at greater risk for than men deterioration in cognition and mental health. Women also experienced more difficulties in everyday tasks involving attention and concentration, executive functions, and temporal orientation. The women in Rosenblum and Cohen Elimelech’s 26 study of older adults (60+ years) reported significantly more cognitive symptoms and difficulties with self-actualization and performing daily functions throughout the pandemic than the men. Otherwise, there is little evidence regarding COVID-19’s effects on functional cognition.
Most studies showed that more women than men had depressive and anxiety symptoms during the lockdown (eg, Fiorenzato et al 25 and Vloo et al 27 ). However, although their anxiety and stress levels were the same, the men’s depression levels were higher. 28 Huang and Zhao 29 found no gender differences in anxiety and depressive symptoms in a younger (M = 35.3 year, SD = 5.6) Chinese population during the outbreak.
Our research continues this line of inquiry, uniquely focusing on younger adults. The COVID-19 pandemic appeared suddenly and aggressively, forcing healthcare systems to cope with multiple challenges without sufficient research or medical information. Examining assessment tools that health providers might use to evaluate people during COVID-19 could promote functional-cognition and health-focused interventions. Therefore, this study aimed to assess functional cognition and health during the COVID-19 pandemic and examine gender-related differences.
Methods
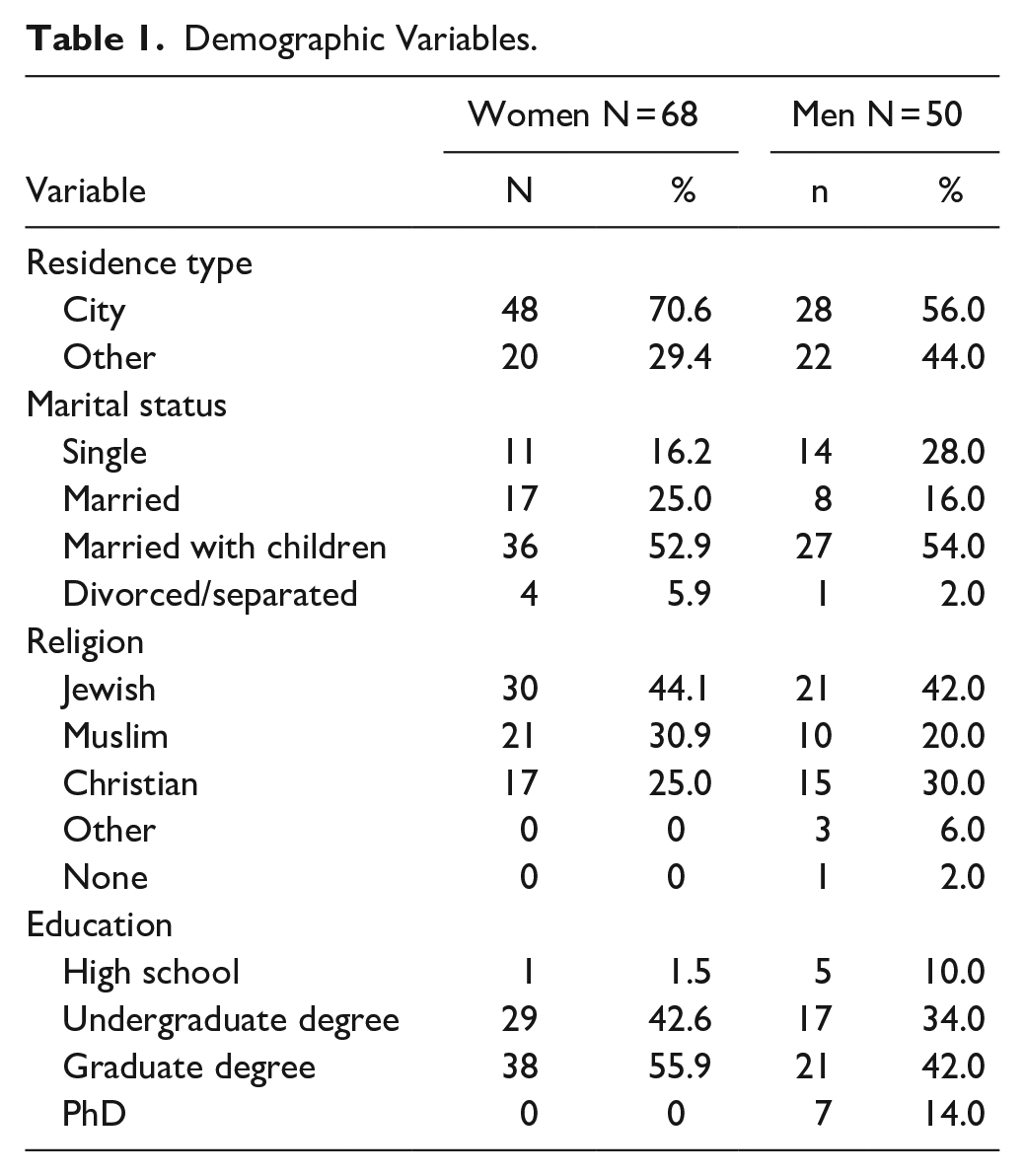
The University of Haifa, Faculty of Social Welfare and Health Sciences Ethics Committee approved this cross-sectional 30 study (503/20). We initially recruited a convenience sample of 153 healthy (community-dwelling adults (20-50 years) by advertising on social media. All were proficient in their country official language. The IBM SPSS software we used randomly eliminated data of several female participants to create gender groups of comparable sizes. Thus, our final sample comprised 118 participants, including 25 who had had COVID-19 (Table 1). G*power software (Version 3.1.9.4) was used to conduct a post hoc power analysis, based on a multivariate analysis of variance (MANOVA) examining group differences, for 2 research groups (men/women) and 4 research variables (of DLQA factors, which was chosen since this MANOVA included the most factors), with a sample size of 118 participants, f2(v) = 0.23, α = .001, a power of 0.84 was accepted.
Demographic Variables.
Individuals who expressed interest in participating and signed the consent form received direct online access, through Google Forms, to the demographic questionnaire, SF-12, and DLQ. The data were collected anonymously, without personal identifying information, between October 28 and December 7, 2020.
The demographic questionnaire gathered background information (gender, age, socioeconomic status, and education) and health status during the pandemic (previous conditions and COVID-19 infection).
The SF-12 31 is a valid, reliable, 32 shortened self-reported version of the SF-36. 33 It includes 12 items from the original questionnaire assessing physical (8 items) and mental (4 items) health components. Respondents rate the items on an ordinal multiple-choice scale; each item has its own scale, and responses vary across items. The final score is the sum of all item scores after several are reversed. Separate scores for each component may be calculated. Scores range from 12 to 47; higher scores reflect better health states.
The DLQ 34 is a valid, reliable 35 self-report assessing IADL and emphasizing functional cognition. It can identify and rate functional activities that changed due to cognitive decline—or changed from the person’s perspective—and, thus, can assist therapists in identifying functional intervention goals. The DLQ is unique because respondents rate the cognitive challenges they experience when performing a range of tasks. Because even healthy people with high functioning levels may perceive some everyday tasks as more mentally challenging, 22 the DLQ is suited to assessing clinical populations with cognitive decline or healthy populations.
The questionnaire is divided into 2 parts: The DLQ-A assesses activities and participation (eg, financial management and household activities); the DLQ-B refers to cognitive symptoms or impairments (eg, working memory) and assesses body function (Figure 1). The questionnaire includes 56 items rated on an ordinal scale from 1 (no mental or cognitive difficulties) to 4 (unable to perform the task). Four additional items about the respondents’ perceptions of their overall functioning and cognitive abilities are rated from 1 (excellent) to 5 (weak). Respondents also rate their satisfaction with their ability to perform what they need and want to do in their everyday lives between 1 (satisfied) and 5 (disappointed).
Internal consistency of the study questionnaires was evaluated based on Cronbach’s alpha. First, the SF-12 internal consistency was tested. For the questionnaire’s physical part (six items), α = .70; for the mental part (5 items), α = .84; and for the whole questionnaire (11 items), α = .83. Internal consistency of the DLQ was then calculated. Cronbach’s alpha for DLQ-A (28 items) α = .94; for DLQ-A Factor 1, household activities (8 items) α = .86; Factor 2, activities involving language comprehension and expression (7 items) α = .82; Factor 3, community participation (7 items) α = .80; and Factor 4, complex tasks (6 items) α = .80. Cronbach’s alpha for DLQ-B (24 items) α = .96; for DLQ-B Factor 1, executive functioning (11 items) α = .93; Factor 2, memory (4 items) α = .79; and Factor 3, the monitoring executive function (9 items) α = .90.
Data analysis was performed using IBM SPSS (Version 27). We used descriptive statistics to describe participants’ demographics and outcome measures. MANOVA test examined differences between COVID-19 and non-COVID-19 participants on the DLQ and SF-12 scores. ANOVA examined differences between gender on total score, and MANOVA examined differences between gender on the factors of each test. Pearson correlations were used to examine correlations between DLQ and SF-12 scores between gender groups. Results were considered significant at P < .05. The statistical tests conducted to confirm that the findings showed normal distribution were acceptable (respectively, skewness and kurtosis values −0.59-1.31 and −0.67-2.3). Therefore, parametric tests were used in all data analyses.
Results
The MANOVA results showed no significant differences in the DLQ and SF-12 scores between participants who previously had contracted COVID-19 (P = .68) and those who had not (P = .83). However, significant gender differences were found in the DLQ and SF-12 scores, As shown in Table 2. The ANOVA tests examined differences in total scores: showed significant gender differences in DLQA, DLQB, and SF12 total scores. MANOVA tests showed gender differences in DLQA, DLQB, and SF12 factor scores. Men’s mean DLQ scores were lower than the women’s, meaning that the men’s self-reported responses attested to better functional cognition. Men scored significantly higher on all SF12 questionnaire elements, reflecting better health states (Table 2).
Mean Scores, Standard Deviations, and F scores of Daily Living Questionnaire (DLQ) and Short Form Health Status Survey (SF-1) by Gender.

We examined the association between the men’s and women’s functional cognition (assessed by the DLQ) and health states (assessed by the SF-12). Negative associations emerged between the values due to inverted scales (Table 3). In the SF-12 general part, all associations were statistically significant (at P < .01 or P < .05). However, several correlations did not reach statistical significance in the SF-12 physical and mental scales.
Associations Between Short Form Health Status Survey (SF-12) and Daily Living Questionnaire (DLQ) Scores by Gender.

P < .05. **P < .01.
We explored associations between demographic variables (eg, residential location, number of children, number of rooms and individuals living in the home, education, and religion) and the DLQ and SF-12 scores using Pearson’s correlations. Because no significant results emerged, we concluded these were not confounding variables in this study.
Discussion
This study examined COVID-19’s effects on adults’ functional cognition and health between gender groups based on the DLQ and SF-12. The data were collected during COVID-19-related lockdowns. No differences were found in functional cognition or health states between participants who previously had contracted COVID-19 and those who had not. We assume that people who did not contract COVID-19 nevertheless experienced isolation, disease, or death of a familiar person (especially during the initial lockdowns) and, like those who contracted the disease, report decreased health status or functional cognition. This might explain the lack of differences in our results. This finding partially aligns with Cleaton et al’s 36 findings of no between-group differences in SF-12 physical scores but significantly lower mental health in the group who had contracted COVID-19. Among the additional research in the literature, Hampshire et al 37 found that COVID-19 negatively affected individuals’ cognitive states, especially executive functions associated with IADL functioning. A more recent study examining young, healthy individuals who had contracted COVID-19 showed significant health declines and increased need for assistance performing IADL. These results indicate that COVID-19 had a considerable impact on everyday functioning even several months after contracting the illness. 38
In our study, men had better scores than women in DLQ and SF-12 tests, reflecting better physical and mental health states and functional cognition during the COVID-19 pandemic. Likewise, Rosenblum and Cohen Elimelech 26 found that a great proportion of older women than older men reported decreased health status during the pandemic. Our study shows similar results among younger participants. Several environmental, biological, or psychological factors differentiating men and women could explain these findings. Gendered labor division, gendered roles, and social norms of performing domestic and care work in a household (eg, cooking, cleaning, and childcare) increased due to COVID-19; such work fell disproportionately on women. 39 Therefore, it might be that more stress was imposed on women than men; perhaps women had to balance employment with childcare more frequently during the lockdowns. Healthcare providers should address these crucial issues in their interventions during the pandemic.
Ausín et al 40 found that women showed more depression, anxiety, PTSD, and loneliness symptoms and less spiritual well-being than men during the lockdown. Samples from the United States, Canada, Denmark, Brazil, and Spain (N = 31 141) showed consistent gender differences in time spent on necessities during the pandemic. For instance, women (especially mothers) spent more time than men on childcare and household chores. 41
Another finding of our study associated better functional cognition with better health. Men’s and women’s functional cognition (DLQ) and health states (SF-12) differed, and all associations were statistically significant in the SF-12 general part. However, several correlations in those questionnaires’ physical and mental parts did not reach statistical significance, meaning no differences between men and women.
This study was based on a convenience sample; therefore, it is impossible to generalize its conclusions. Further, the sample included only a few individuals who had contracted COVID-19, with no information on the symptom severity they experienced. The findings might have been different if the percentage of participants who had had the disease was larger. Results of this study should be interpreted cautiously since data collection of this study begun during lockdowns (October 2020), while the longer effects of COVID-19 pandemic may have not been fully presented yet in some of the participants. Moreover, participants answered the questionnaires once. If they were to answer again in a longitudinal study, their reports might differ due to Long-COVID-19 syndrome, in which their health status and functional cognition might worsen over time. Future studies should include larger, more representative samples of individuals who had contracted COVID-19 and consider adding standard, objective, health and functional cognition measures to complement the self-report measures.
This study’s findings show the importance of addressing gender differences during a crisis like the COVID-19 pandemic. A functional cognition (IADL) assessment is advised when assessing and treating individuals who contracted COVID-19, even if young and healthy. The DLQ, an important questionnaire in the occupational therapist’s toolbox for evaluating functional cognition, might also be valuable for other health providers, allowing them to assess important information about the person’s function.
Footnotes
Acknowledgements
We would like to thank Dovrat Sagie, Heba yahia, Yael Gutman, Rozan Copty, and Shir Segal-Rotenberg for their help in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.