
Abstract
Introduction:
While there may be differences in the choice of suicide methods between attempters with and those without a history of psychiatric disorders, it is not clear whether these differences predict the actual degree of physical injury. The present study aimed to investigate the association between the history of psychiatric disorder and the degree of physical injury among suicide attempters in a Japanese rural area.
Methods:
We conducted a cross-sectional study analyzing secondary data of 806 suicide attempters from April 2012 to March 2022 obtained from a Japanese rural city. The exposure variable was a history of psychiatric disorders. The primary outcome was the degree of physical injury of suicide attempters: moderate and severe. We conducted a multivariate Poisson regression analysis to estimate the prevalence ratios (PRs) and 95% confidence intervals (CIs).
Results:
Among 806 suicide attempters, a significant negative association between the history of psychiatric disorder and the degree of physical injury was observed (PR = 0.40; 95% CI, 0.28-0.59). Those with and without psychiatric disorders were more likely to choose low- and severe-lethality suicide methods such as drug or psychotropic overdoses and hanging or deep wrist injuries, respectively (P < .001).
Conclusions:
The present study highlights the importance of considering suicide attempters, both with and without psychiatric disorders, while formulating targeted suicide prevention strategies.
Introduction
Globally, approximately 800 000 people die by suicide annually. In 2016, the suicide rate was 10.6 suicides per 100 000 persons. 1 However, the global age-standardized suicide rate decreased by 36% from 2000 to 2019, 2 with the suicide rate in Japan, which is higher compared to other high-income countries, also showing a decline.3,4 However, after the outbreak of the COVID-19 pandemic in 2019, the suicide rate has been gradually increasing in Japan.4,5 Previous studies have reported that suicide rates tend to increase in response to social events such as economic difficulties.6,7 Because suicides may increase due to global social events such as natural disasters, infectious disease pandemics, and economic crises, suicide prevention strategies are an important and urgent public health issue.
The major risks for suicide are a history of suicide attempts and of psychiatric disorders.8 -10 A systematic review and meta-analysis revealed that a history of self-harm and the presence of any psychiatric disorders are associated with more than a 10-fold increase in the odds of suicide.7,10 Therefore, addressing both factors would significantly impact suicide prevention strategies.
People who attempt suicide once are more likely to engage in subsequent, potentially lethal suicidal behavior. Identifying and monitoring suicide attempters is crucial. Although the number of suicide attempters is reportedly 10 to 30 times higher than that of those who completed suicide, there is little and low-quality data on global suicide attempts. 8 It is thus necessary to analyze public data through which suicide attempters can be identified and their medical information can be collected.
Those with psychiatric disorders comprise one of the major at-risk groups for suicide attempts as well as completed suicides.8,11 -13 More than 90% of suicide attempters are reportedly afflicted with one or more psychiatric disorders. 11 Accordingly, screening people with psychiatric disorders as high-risk is essential. However, the presence of these disorders alone is not a sufficient cause to explain suicide attempts. Characteristics of suicidal behavior differ between those with and those without a history of psychiatric disorders. A previous study reported that individuals with psychiatric disorders exhibit a tendency to opt for less lethal suicide attempts, whereas those without psychiatric disorders tended to choose more lethal means. 14 While differences exist in suicide methods between those with and without psychiatric disorders, it is not clear whether they imply the actual degree of physical injury. In addition to the chosen methods of suicide attempts, assessing the degree of physical injury due to the suicide attempt may reveal differences in suicidal behavior between those with and those without psychiatric disorders. To the best of our knowledge, however, few studies have examined the association between the history of psychiatric disorder and the degree of physical injury among suicide attempters in the community, which this study seeks to do using secondary data and focusing on a Japanese rural area.
Methods
Study Design and Data Source
We conducted a cross-sectional study using secondary data obtained from Akita City in rural northern Japan. Akita City’s public health center collects data on self-inflicted injuries from 5 hospitals with emergency room departments. The data include information on circumstances leading up to emergency room visits, history of psychiatric disorders, and degree of physical injury as assessed by paramedics, emergency physicians, and psychiatrists at the time of the patient’s emergency room assessment. If there was insufficient information regarding a history of psychiatric disorders, the assessment staff confirmed the detailed history to other hospitals in Akita City. We obtained data on 1119 suicide attempts from April 2012 to March 2022 in a format that preserves the anonymity of individuals. These 1119 attempts reflect any transport to the emergency center and thus may include multiple attempts for the same individual for those who attempted suicide and were transported more than once during this time period. This study received ethical approval from the Institutional Review Board of Akita University Medical School (approval number: 2998). The data used in this study were anonymized and devoid of personal information to follow strict ethical guidelines. No identifying information that could potentially violate the privacy of individuals was included in the analysis.
Data Contents
We obtained data for age by decade, sex, history of psychiatric disorders, degree of physical injury, number of suicide attempts, availability of supporters, treatment for psychiatric disorder, other medical department treatment, and methods of suicide attempts.
The exposure variable was history of psychiatric disorders, classified according to the International Classification of Disease, 10th revision (ICD-10). 15 The presence of a history of psychiatric disorders was defined as an individual who met any one of the following ICD-10 codes: F0-F8, F99, or G40.
The primary outcome was the degree of physical injury of suicide attempters, which was assessed by emergency physicians and classified into the following 4 categories: cardiopulmonary arrest, severe, moderate, and low. Suicide attempters were classified into 2 groups: moderate (low or moderate) and severe (severe or cardiopulmonary arrest).
Statistical Analysis
Out of the 1119 suicide attempters, 230 with no relevant data on history of psychiatric disorders and 83 with no data on degree of physical injury were excluded, leaving 806 individuals who were included in the analysis.
To determine the baseline characteristics, we evaluated the distribution of age (10-39, 40-59, ≥60, missing), sex (male, female, missing), number of suicide attempts (first time, twice or more, missing), availability of supporters (presence, absence, missing), psychiatric treatment (currently in treatment, previously treated, none, missing), and other medical department treatment (currently in treatment, previously treated, none, missing) according to each group of individuals with/without a history of psychiatric disorders, using a Fisher’s exact test.
To examine the association between a history of psychiatric disorders and degree of physical injury, we conducted a multivariate Poisson regression analysis with robust error variance and estimating the prevalence ratios (PRs) and 95% confidence intervals (CIs).16,17 The following 2 models were employed in this study: Model 1 was adjusted for age and sex, while Model 2 was additionally adjusted for number of suicide attempts and availability of supporters. We also conducted stratified analyses by sex (male and female) and age (<60 years and ≥60 years), testing for interactions between them. In these analyses, we excluded participants who had no data on sex and age, respectively.
We used a Fisher’s exact test and a post-hoc Bonferroni test to compare the degree of physical injury (cardiopulmonary arrest, severe, moderate, and low) between those with and those without psychiatric disorders. Chi-square tests were used to compare common methods of suicide attempts (hanging, deep wrist injuries, drug and psychotropic overdoses) between those with and those without psychiatric disorders. Additionally, as a post-hoc demonstration, we estimated the proportion of individuals currently receiving psychiatric treatment among those who attempted suicide by each specific method according to their history of psychiatric disorders.
All statistical analyses were performed using IBM SPSS Statistics version 28 (IBM SPSS Software Group, Chicago, IL, USA). All statistical tests were 2-sided analyses, and differences were considered significant at P < .05.
Results
Of the total participants (n = 806), 616 (76.4%) had a history of one or more psychiatric disorders. Table 1 depicts the characteristics of participants according to their history of psychiatric disorders. There were 421 (52.2%) participants aged 10-39, 197 (24.4%) aged 40-59, 139 (17.2%) aged ≥ 60, and 49 (6.1%) with missing data, respectively. Participants with psychiatric disorders were slightly younger than those without; 545 participants (67.6%) were female, and they exhibited no difference according to their history of psychiatric disorders. Although participants with no psychiatric disorders had more missing data, those with psychiatric disorders were more likely to be first-time suicide attempters. Of the total participants, most (n = 724, 89.8%) had supporters. Compared with participants with no psychiatric disorders, those with psychiatric disorders were more likely to currently receive psychiatric treatment. However, no difference was found in terms of the status of other medical department treatment based on their history of psychiatric disorders.
Characteristics According to History of Psychiatric Disorders (n = 806).

Table 2 depicts the results of the association between the history of psychiatric disorders and the degree of physical injury using multivariate Poisson regression analysis. In Model 1, after adjusting for sex and age, a significant negative association between the history of psychiatric disorders and the degree of physical injury was observed (PR = 0.34; 95% CI = 0.25-0.46; P < .001). In Model 2, after adjusting for full confounders, a significant negative association was observed between the same variables (PR = 0.40; 95% CI = 0.28-0.59; P < .001).
Association Between History of Psychiatric Disorders and Degree of Physical Injury (n = 806).

Abbreviations: PR, prevalence ratio; CI, confidence interval.
Model 1 (adjustment variables): sex and age. Model 1 (adjustment variables): model 1, number of suicide attempts, and availability of supporters.
Table 3 depicts the results of the stratified analyses of the association between the history of psychiatric disorders and the degree of physical injury. Analyses stratified by sex revealed no significant interaction (P = .601). In both male and female participants, the presence of psychiatric disorders was negatively associated with the degree of physical injury, with PRs (95% CIs) of 0.36 (0.22-0.60) and 0.47 (0.26-0.85), respectively. In analyses stratified by age, significant associations were observed among participants aged < 60 and ≥ 60 (PR = 0.59; 95% CI = 0.37-0.93 and PR = 0.20; 95% CI = 0.11-0.37, respectively). Although the PR of participants aged ≥ 60 years was larger than those aged < 60 years, no significant interaction was observed (P = .085).
Stratified Analyses by Sex and Age.

Abbreviations: PR, prevalence ratio; CI, confidence interval.
Stratified by sex (adjustment variables): age, number of suicide attempts, and availability of supporters. Stratified by age (adjustment variables): sex, number of suicide attempts, and availability of supporters.
Figure 1 provides a detailed comparison of the degree of physical injury between those with and those without psychiatric disorders using a Fisher’s exact test and a post-hoc Bonferroni test. With the former, a significant difference was observed between the history of psychiatric disorders and the degree of physical injury (P < .001). With the latter, significant differences were found between history of psychiatric disorders and cardiopulmonary arrest and moderate physical injury (P < .001). Participants with psychiatric disorders were more likely to exhibit a moderate degree of injury (35.4%), whereas those with no psychiatric disorders were more likely to exhibit cardiopulmonary arrest (23.7%).

Comparison of the detailed degree of physical injury between participants with psychiatric disorders and those without (n = 806).
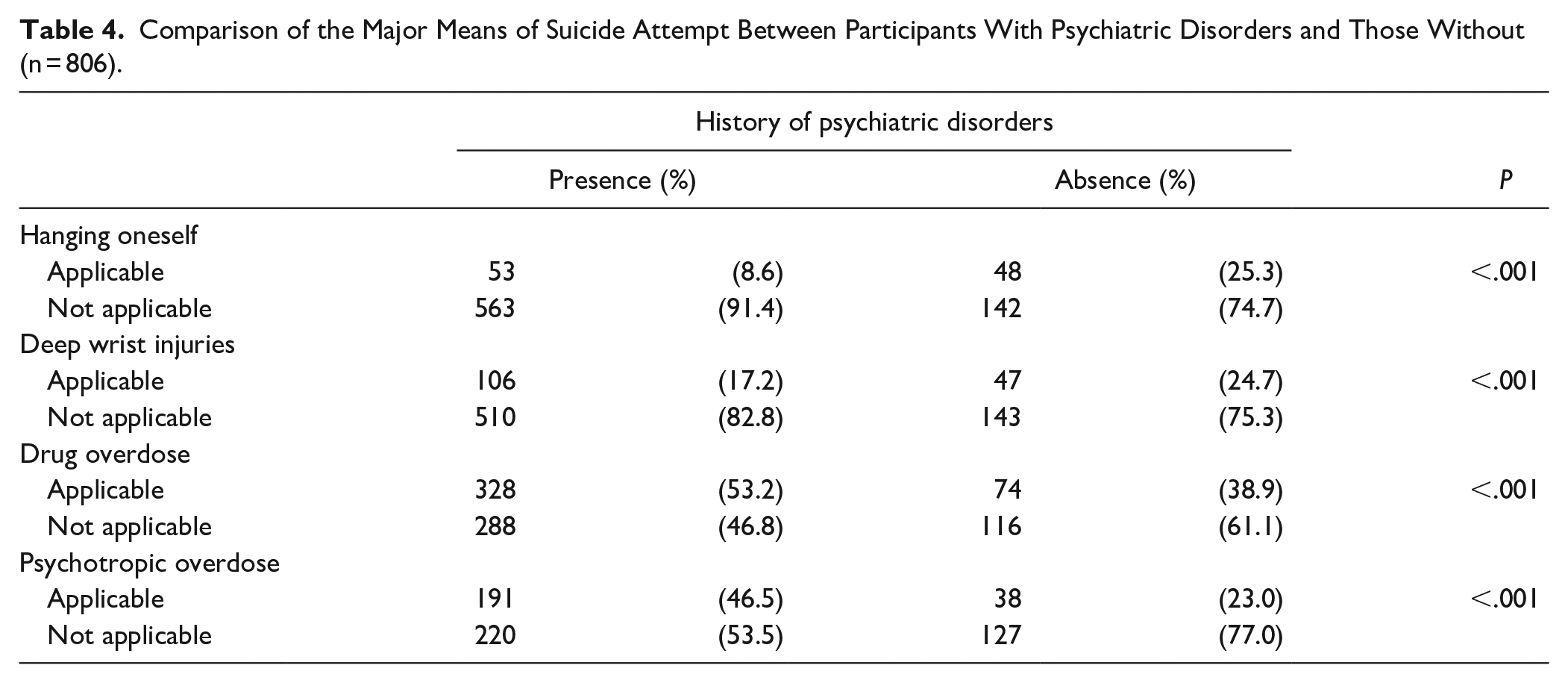
Table 4 shows the comparison between the most common methods of suicide attempts between participants with and those without psychiatric disorders using a chi-square test. Participants with psychiatric disorders were more likely to attempt suicide by drug or psychotropic overdoses (P < .001), while those with no psychiatric disorders were more likely to attempt suicide by hanging or deep wrist injuries (P < .001). The proportions of individuals currently receiving psychiatric treatment among those who attempted suicide by each method (based on their history of psychiatric disorders: presence vs absence) were as follows: 60.4%versus 31.3% for hanging, 61.3%versus 55.3% for deep wrist injuries, 72.9%versus 70.3% for drug overdose, and 84.3%versus 89.5% for psychotropic overdose.
Comparison of the Major Means of Suicide Attempt Between Participants With Psychiatric Disorders and Those Without (n = 806).
Discussion
The results of analyzing secondary data from a Japanese rural area revealed that the proportion of individuals with severe physical injury among those with psychiatric disorders was statistically significant lower than among those without psychiatric disorders. No difference in this association by sex or age (≥ 60 or < 60 years) was observed. People with psychiatric disorders were more likely to have moderate physical injuries compared to those without psychiatric disorders, who were more likely to have cardiopulmonary arrest.
Although previous studies have examined the different suicide methods employed by attempters with and without psychiatric disorders, they have failed to explore the degree of physical injury due to the suicide attempt. Among soldiers in Israel, having a psychiatric disorder was significantly associated with mild, but not moderate and severe, suicide attempts even with increased odds ratios. 18 This is inconsistent with the results of the present study. Soldiers’ exposure to specific stresses, such as combat, has a negative impact on their mental health and suicide risk,19,20 which may be the reason for the differing results in the general population.
In a Korean study that examined suicide methods’ lethality among attempters, the presence of psychiatric disorders was associated with the choice of a low-lethality suicide method such as drug overdose, whereas the absence of psychiatric disorders was associated with that of a high-lethality one such as hanging. 14 Another study reported that patients with schizophrenia were more likely to choose methods such as drug overdose (low lethality), while the general US population was more likely to choose methods such as firearms (severe lethality). 21 These results were consistent with the results from the present study, which revealed that those with psychiatric disorders are more likely to choose drug overdose, while those without psychiatric disorders are more likely to choose hanging or deep wrist injury. Because the possession of firearms is restricted to very few people in Japan, cases of suicide by firearm are extremely rare. 22 A systematic review revealed that the most common methods of suicide attempts in Japan were drug overdose (52%), wrist injury (38%), jumping from a height (12%), and hanging (7%). 23 Our findings were similar, except for jumping (3.8%, data not shown), seemingly reflecting the trend for Japan as a whole.
Regarding suicide prevention strategies, psychiatric visits, including diagnosis of psychiatric disorders, have a significant impact.8,24 -26 In the present study, among suicide attempters who chose hanging, the proportion of those without psychiatric disorders who were currently undergoing psychiatric treatment was half (31.3%) of those with psychiatric disorders (60.4%). This could be partially attributed to stigma. Psychiatric disorders are often viewed as socially unacceptable, especially in Asian societies, 27 and such stigma and discrimination against individuals diagnosed with psychiatric disorders may cause delays and avoidance of psychiatric treatment. 28 For example, in a rural area of Japan (similar to the present study area), stigma against psychiatric disorders was found to negatively impact patients, making it difficult for them to seek help from others. 29 Promoting help-seeking is an important aspect of suicide prevention.30,31 It is also important to offer support to suicide attempters with and without psychiatric disorders so that they can visit a psychiatrist and practice help-seeking behavior.
This study has a strength. We examined the association between the history of psychiatric disorders and the suicide methods of—as well as the degree of physical injury among—attempters. Hence, the finding that those with undiagnosed psychiatric disorders may choose more lethal suicidal behaviors can be helpful to formulate suicide prevention strategies.
The present study, however, also has some limitations. First, it was conducted using secondary data from a single city in rural Japan. As mentioned in the discussion, compared to urban areas, this rural study area may be more affected by social stigma against psychiatric disorders. Therefore, the generalizability of our findings to Japanese suicide attempters may be limited. Second, some suicide attempters died from cardiopulmonary arrest after being transported to the emergency room. Although the assessment staff in the emergency room confirmed the psychiatric disorders of those who suffered cardiopulmonary arrest through their past medical records, a misclassification could have occurred. Third, the data of this study included those who were transported to the emergency center several times. Because we obtained data in a format that did not identify individuals, data duplication could not be addressed. However, we did examine the association between psychiatric disorders and the degree of physical injury among first-time suicide attempters (excluding any data duplication), and the findings did not differ from the main results (PR = 0.57; 95% CI, 0.31-1.04; P = .067).
Conclusion
This study revealed the importance of taking into consideration both individuals with and those without psychiatric disorders as a suicide prevention strategy among suicide attempters. For those without psychiatric disorders, medical and social support should be made accessible, allowing them to visit psychiatrists and seek in help, which could lead to a decrease in suicide rates.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.