
Abstract
Objective:
Acid reflux disease is a common condition with recurrent symptoms affecting the quality of life of many Americans. Lifestyle/dietary modification is critical for management of acid reflux disease. Adherence to these recommendations is variable. The purpose of this study was to better understand the experience of patients with reflux disease (GERD/LPR) and explore factors that impact the integration of lifestyle modifications into their daily lives.
Methods:
Patient with diagnoses of GERD and/or LPR were recruited from an outpatient laryngology clinic and completed the Reflux Symptom Index (RSI) and a semi-structured interview. Interviews were transcribed and underwent thematic analysis.
Results:
Twenty-three patients—mean age and RSI of 61 and 16.1 respectively—were recruited. Four main themes emerged: (1) Care team interaction—focus and quality of physician counseling, useful educational handouts, dietician/nutritionist counseling; (2) Motivation to change—impact on symptom severity, avoiding undesired interventions, and poor health outcomes; (3) Implementing lifestyle changes; and (4) Impact of disease on patient. No patient had seen a dietician. Patients who experienced dietary counseling for other conditions felt reflux-specific counseling with a dietician would be beneficial. While patients found educational material on diet to be helpful, lists of foods to avoid were discouraging; providing a positive list of preferred foods may be more helpful.
Conclusion:
Lifestyle modification counseling should incorporate multiple aspects of the patient experience. Patients desire information regarding medication side effects. Educational handouts should include prioritized list of recommended dietary restrictions and acceptable/alternative food options. Referral for dedicated dietician counseling can also be considered to increase understanding of the importance of, and adherence to, lifestyle modification.
Introduction
Acid reflux disease is a common condition in the United States often associated with recurrent symptoms and poor quality of life. It can present as two different clinical subtypes: Gastroesophageal reflux disease (GERD) and Laryngopharyngeal reflux disease (LPR). GERD is the reflux of stomach acid into the esophagus, throat, and mouth which classically presents as heartburn. LPR, also known as silent reflux, is characterized by reflux of stomach acid and contents into the laryngopharynx, leading to hoarseness, dysphagia, chronic cough, and constant throat clearing. LPR can occur with or without GERD.
The mainstays of treatment for both conditions include medications as well as lifestyle modifications. Proton pump inhibitors (PPIs) are very commonly prescribed and available over the counter. While PPIs are very effective in reducing GERD symptoms, their superiority over placebo in LPR is controversial. 1 Lifestyle modifications can also be effective. The American College of Gastroenterology as well as the American Academy of Otolaryngology—Heck and Neck Surgery guidelines endorse lifestyle modifications for GERD and LPR. These include eating smaller, more frequent meals at least 2 to 3 hours before bedtime, limiting high-fat, tomato-based, and spicy foods, reducing carbonated, caffeinated, and citrus-based beverage intake, controlling weight, and avoiding use of alcohol and tobacco.
There is very limited research analyzing the patient experience with treatment of GERD and/or LPR. One notable 2017 study by Pisegna et al examined patient views on their reflux symptoms and medication routines. It found that the incorrect use of PPIs due to lack of patient education was one of the reasons for poor compliance and symptom improvement. 2 Likewise, adherence to lifestyle modifications has also been shown to be variable, resulting in poorly controlled symptoms. 3 However, to our knowledge, no qualitative studies have been conducted to investigate patient perspective on reflux lifestyle modifications and factors that impact adherence.
In our aging population, the incidence and severity of reflux is expected to rise further, with many elderly patients presenting to clinics with reflux-related complaints. 4 While PPIs can be prescribed for a limited time period, lifestyle changes will remain the main long-term treatment for management of chronic reflux disease. However, the changes can only be truly effective in managing reflux symptoms if patients are able to follow them approriately. The purpose of this qualitative study was to explore, from the patient perspective, factors that impact the integration of recommended dietary and lifestyle modifications in management of acid reflux disease in patients with GERD and/or LPR. By identifying barriers to integration, we hope to facilitate development of future interventions that improve adherence and symptom control, ultimately leading to a better quality of life.
Methods
Setting
The University of Kansas Institutional Review Board approved this study. Purposive sampling technique was used to recruit patients with diagnoses of GERD and/or LPR from an academic outpatient clinic of one otolaryngologist between July 2021 and October 2021. Electronic Medical Record (EMR) was accessed to identify patients who met the following inclusion criteria: 18 years or older with (1) a diagnosis of GERD and/or LPR documented in EMR, and (2) a previous physician recommendation to make lifestyle modifications at least 3 months prior to study, including elevation of the head of the bed and elimination of tomato-based products, citrus fruits, spicy foods, and carbonated and caffeinated drinks. Patients were excluded if they did not speak English or did not recall receiving counseling from their physicians regarding management of reflux disease. Recruitment was continued until thematic/data saturation was reached, such that further interviews and analysis no longer revealed any new themes and ideas.
Outcomes
All patients completed the Reflux Symptom Index (RSI), 5 a validated nine-item questionnaire designed to assess reflux symptoms and severity, at the time of recruitment as a means of assessing disease burden in our sample. It has a maximum total score of 45; a score of ≥13 is considered indicative of clinically significant reflux disease.
An additional questionnaire was used to collect basic demographic information (gender, race, ethnicity, education, employment status, income, ZIP code, and marital status), tobacco and alcohol use, current use of PPI, dietary regimen, and physical activity.
Individual semi-structured interviews using an interview guide (see Table 1) were conducted by the first author, primarily face-to-face in a private clinic room following the scheduled clinic appointments, with the exception of 4 interviews completed remotely on a later day via Zoom. Questions represented topics and factors identified in the literature to impact patient adherence to lifestyle changes, and captured patients’ knowledge of reflux disease, understanding of recommended reflux lifestyle modifications, and experience with making these changes. Interviews ranged from 10 to 25 min.
Example of Semi-structured Interview Questions.

Analysis
All in-person and remote interviews were audio-recorded via Zoom; recordings were auto-transcribed via Trint (London, UK) artificial intelligence software. Accuracy of transcripts was verified by the first author via comparison against audio recordings, and transcripts were then uploaded into Dedoose (Hermosa Beach, CA). Data was analyzed via qualitative content analysis method and conducted by both authors. 6 Inductive thematic coding approach was utilized. After review of a representative sample of five interviews, a preliminary codebook was formed de novo to represent major themes and subthemes that were manually generated from participant responses during the interviews. The preliminary codebook was revised in an iterative fashion until consensus was reached regarding final themes and subthemes. All interview transcripts were then individually coded. Descriptive statistical data from the RSI and associated demographic survey was performed in Microsoft Excel, version 16.16.27.
Results
Twenty-five patients were recruited and completed questionnaires. Two patients were unable to be contacted to arrange interviews. Of the twenty-three patients who completed questionnaires and interviews, 56.5% had both GERD and LPR, 34.8% had a diagnosis of LPR only, and 8.7% had GERD only. Average RSI score was 16.1 out of 45 (range: 3-33). Additional patient information from questionnaire responses is presented in Table 2.
Patient Characteristics and RSI Scores.

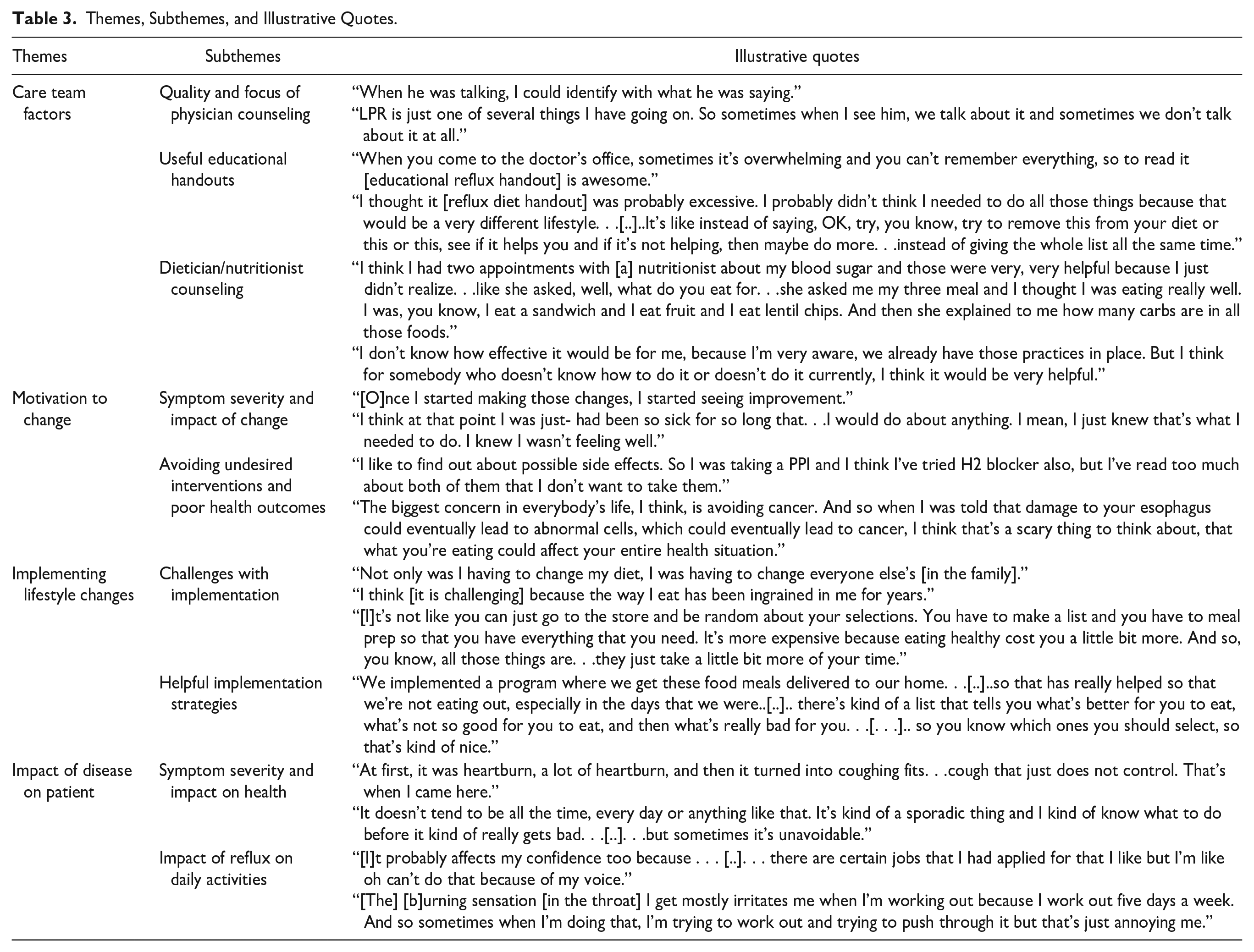
Four general themes emerged: (1) Care Team Interactions; (2) Motivation to Change; (3) Implementing Lifestyle Changes; and (4) Impact of Disease on Patient. Specific sub-themes were also identified, and representative quotes are shown in Table 3.
Themes, Subthemes, and Illustrative Quotes.
Care Team Interactions
Patients had opposing beliefs about the quality and focus of physician counseling. Most reported good interactions with their physician and felt that the quality of counseling was satisfactory. However, many patients also noted several areas of improvement regarding focus of physician counseling (Table 4). For example, when patients received a dietary handout at their appointment, they most commonly recalled being recommended to avoid foods like tomatoes, spices, oranges/citrus fruits, soda, and coffee/caffeine. Such “extensive list” of foods to avoid was “too much” and daunting for many patients. Providing a list of foods to prioritize was felt to be more helpful.
Recommendations for Physicians and Patients.

Patients were often motivated to incorporate recommended lifestyle changes to minimize their need for medications but felt counseling from their care team on PPI side effects was inadequate. Patients noted that physicians were typically more focused on prescribing medications than emphasizing lifestyle modifications or non-pharmacologic therapies.
“[P]hysicians tend to give you whatever drugs you need to help your problem without warning anything much about the side effects. . .[. .]. . .I really think doctors should give more natural options and of course, they will prescribe whatever you need to be comfortable, but they could also warn you of the side effects and say now, you know, if you did this instead. . .” – an 87-year-old patient with GERD
Although reflux-specific nutritionist/dietician counseling was not utilized for any patient, many believed it would be helpful for receiving personalized guidance, particularly for patients unfamiliar with the dietary changes recommended: “I can read all the books that are out there about acid reflux or about eating a good diet, but talking one-on-one about my specific diet, about what I have been eating and what I should be changing about what I do, that could be helpful.”
Motivation to Change
The most common motivating factor was severity of reflux disease and how lifestyle changes impacted it. Patients who experienced bothersome reflux symptoms for a long time or noticed worsening symptoms after poor diet choices and notable improvement following modifications were more motivated to change their lifestyle.
“[I was motivated] [b]ecause of the way my body felt. . .[. .]. . . I did not like the indigestion, the coughing, and just the way it made you feel when you were not to even trying to give those things up. Because once I did 80 percent, 90 percent give [up] those things [triggers], you know, I have felt better.” – a 70-year-old female with GERD and LPR
Avoiding medications, primarily because of side effects, was another frequently reported motivator of lifestyle change. Other reasons included polypharmacy and personal desire to not depend on medications. One 48-year-old female patient shared, “If I knew I could go off the medicine by making the [lifestyle] changes, maybe I would make more effort. . . If the doctor said, ‘you make these changes, we can get you off the medication’ that probably would be highly motivating.”
Fear of undergoing surgery for reflux disease sequelae, especially tracheal stenosis, also motivated several patients. For example, a 51-year-old patient stated: “At first, it was hard just changing my diet to give up things. But after our second surgery [for tracheal stenosis], I was like, it’s time to get serious so that I don’t have to do this all the time.”
Implementing Lifestyle Changes
Patients adopted several helpful strategies to overcome challenges of implementing lifestyle/dietary changes (Table 4). Social support was important for sustaining these modifications. Patients’ families offered gentle reminders and encouragement which “kept them going” when they felt like giving up. Patients noted that raising the head of the bed when laying down was a simple and easy lifestyle change. The most attempted dietary changes were fewer spices, less tomato-based sauces, and low-fat meals. Challenges with implementing dietary changes can be grouped into 2 categories: logistics and changing established dietary likes and habits.
Logistic factors were a hurdle particularly for cooking reflux-friendly meals at home. These included more planning requirement for grocery shopping and meal prep, lack of time to cook due to work schedule, and the need to accommodate family’s likes/dislikes by either cooking a separate meal for them or convincing them to adopt the patient’s lifestyle.
“I get off work, and especially back when I had three kids in the house, it’s just easier to just grab something that’s already premade, frozen or whatever, chock full of sodium or- and throw that in than it is to get all the ingredients and sit down, not sit down but stand up, make something up.” – a 53-year-old female with GERD and LPR
The other main challenge was changing established dietary likes and habits. Patients had the hardest time avoiding coffee and fast food when they were an integral part of their routine. “I really need that caffeine in the morning, and I don’t want to give it up.” Additionally, it was difficult for patients to find reflux-friendly food options when dining out and to restrain themselves if people around them were eating without restrictions, especially on vacations or special occasions with loved ones. Lack of, or delay in, desired results further added to the challenge. “I think one of the things that was frustrating was that while it [lifestyle changes] might help, it wasn’t a guarantee that that would help.” Another 51-year-old patient added, “[I]f you don’t immediately get the result that you want, you’re like, well, I don’t want to do this anymore. It’s not working. So, it’s just not the easiest.”
Impact of Disease on Patients
The majority of patients were able to describe acid reflux mechanism and its sequelae. Symptoms and disease severity were variable amongst patients. Reflux symptoms experienced by patients ranged from globus sensation and dysphagia and to chest pain and heartburn. Most bothersome symptoms included cough, hoarseness of voice, and throat clearing. Concurrent reflux-related conditions like tracheal/subglottic stenosis greatly shaped their health experiences, particularly resulting in hospitalizations and surgeries. “[T]he minute I feel it [reflux] coming on, it just seems like it just goes from zero to 60 in no time and then I end up having to go back in [to surgery] and get my throat, my trachea dilated.”
In addition, reflux disease affected how patients participate in daily activities, including work/hobbies, exercise, and grocery shopping. For patients who rely on their voice for recreational or professional activities such as church choir singers or real estate agents, hoarseness was felt to significantly impact their performance, self-esteem, and job opportunities. Difficulty with exercise was noted to be related to breathing issues caused by reflux. In terms of grocery shopping, patients looked at food labels more often and were more vigilant about what they buy.
Discussion
Lifestyle modifications are a key component of long-term management of reflux disease. Understanding patients’ perspective on reflux disease and lifestyle modifications is critical to ensuring improved adherence to recommendations. To address this gap in the literature, this study qualitatively analyzed semi-structured interview transcripts of patients with reflux disease (GERD and/or LPR) and identified 4 salient themes: care team interactions, motivation to change, implementing lifestyle changes, and impact of disease on patients. Better physician counseling on PPIs and lifestyle changes was desired. Dietary handouts need to be more practicable for patients and dietician referrals should be considered. Logistical factors were recognized as a major challenge to implementation of change.
Physician counseling should incorporate a comprehensive discussion of lifestyle modifications and medication/PPI side effects. Existing literature acknowledges the impact of lifestyle factors on GERD symptoms. 7 A meta-analysis study from 2019 investigating the efficacy of lifestyle modifications in adults with GERD found that, “key lifestyle factors such as diet, physical exercise, smoking, and alcohol use may affect most people living with GERD in some way but not necessary in the same way.” 2 Other studies have also found dietary modifications to be effective in managing reflux symptoms in LPR patients, 8 even as a possible alternative to medications. 9 Based on patient interviews, we believe physicians must spend more time counseling lifestyle changes and follow up on patient progress regularly. Feedback and reinforcement by physicians can contribute to patient adherence as noted in a Japanese study on hypertensive patients. 10 In addition, counseling on medication/PPI side effects was also desired by patients; it increased motivation to consider lifestyle changes. Several studies highlight suspected adverse effects of long-term PPI use.11,12 Yet, consistent with Ghosh et al 13 study, most of our patients did not receive this information from physicians, conducting their own research instead. Fox et al, 14 found that patients with allergic rhinitis had increased confidence in their physician’s suggested plan, and consequently better adherence, when the care team engaged in a discussion of their diagnosis, purpose and mechanism of intranasal treatment, and associated side effects. Physicians should include a discussion on PPI mechanism and side effects with patients for better education and likely improved adherence to lifestyle changes.
Dietary education and resources can also be enhanced. Patients prefer handouts with a prioritized list of foods to avoid and physician recommendations that include permissible/alternative food options. These suggestions should be incorporated into practice to help patients set realistic goals for themselves. It must also be noted that since patients felt their appointments were brief, there is insufficient time to discuss concerns regarding diet/lifestyle changes. Referral to nutritionist/dietician can address this issue by offering an additional resource for patients which is also effective in improving diet quality, diabetic outcomes, and weight loss. 15
In our study, patients indicated several hurdles in implementation of lifestyle changes. While we did not directly assess health literacy, most patients were able to provide correct descriptions of their understanding of LPR/GERD, suggesting that it did not impact adherence. This contrasts with another study which established a significant positive correlation between health literacy and adherence to non-medication regimens. 16 Primary hurdles for our patients were logistical challenges, changing established dietary habits, and frustration from lack of desired results. Similar barriers were identified in other studies on patients with cardiovascular disease risk, diabetes, and obesity.17 -19 Cooking meals was identified as a big problem which may also be addressed with nutrition/dietician counseling. While improvement is not immediate, patients able to link flare with consumption of triggering foods displayed better adherence with recommendations. Even outside of dietary changes, logistical factors remain a major barrier to treatment adherence. For example, patients with allergic rhinitis discussed increased time at the sink and cleaning needs afterwards as their biggest barrier to consistent use of intranasal treatments, such as nasal sprays. 14 Motivational interviewing, found to effective in improving cardiovascular health, 20 may also be utilized by physicians/dieticians, along with cognitive behavioral strategies to encourage patients through the implementation challenges they encounter.
This study had its limitations. Patient sample was collected from 1 physician’s clinic only and predominantly constituted Caucasian females. As such, external validity may be limited. Non-English-speaking patients were not included in the study due to inaccessibility of interpretation services. It is possible that such patients face unique and increased barriers which our study could not address. Furthermore, patients who agreed to be interviewed could also differ from those who were uninterested in their perception and experience with reflux management. Due to lack of feasibility, patients did not review transcripts after their interviews to verify accuracy. Another limitation is that this study did not differentiate between GERD and LPR. With no clear criteria to diagnose LPR, the determination of patients was solely based on documentation of LPR in the EMR which may also introduce bias for true diagnosis.
Conclusion
Patients with reflux disease are primarily motivated to attempt lifestyle changes by notable impact on symptoms and avoiding unnecessary medications due to side effects. Priority areas for improvement include physician counseling and patient education. Patients feel that they did not receive adequate counseling on PPI side effects. They desire knowledge about permitted foods, as opposed to exhaustive lists of items to avoid, which could potentially be done in conjunction with dietician/nutritionist referral. Physicians should be aware of implementation barriers and be ready to proactively counsel patients on how to address common issues. Further study on physician perspective of their counseling and challenges they encounter with patient adherence/response can help identify and bridge gaps between patient-physician expectations and align their goals and plans for better management of reflux disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.