
Abstract
Objectives:
Our study aims to assess the effectiveness of implementing a case manager-led Multidisciplinary Team approach in the primary healthcare setting on improving glycemic control and reducing cardiovascular risks for T2DM patients over a 6-month period.
Methods:
This retrospective record-based follow-up study was carried out on 3060 uncontrolled T2DM patients in primary healthcare centers in Riyadh First Health Cluster over a period of 6 months. The patient records are investigated and analyzed, including demographic characteristics and measurements of Hemoglobin A1c (HbA1c), Low-Density Lipoprotein Cholesterol (LDL-C), total cholesterol, and BP levels at enrollment and after 6 months of Multi-Disciplinary Team follow-up. The changes in the study variables and their correlations to each other are tested using Statistical Package for the Social Sciences software.
Results:
At enrollment, our patients were characterized by poor glycemic control (HbAIC > 8%). Most of them have high body weight with a mean BMI of (31.2 ± 1.7), and nearly two-thirds are either hypertensive or have dyslipidemia (43.4% and 47.3% respectively). After 6 months of MDT follow-up, there is a significant improvement in glycemic control among 1971 patients (64.4%), with a reduction in the mean level of different outcomes relative to baseline HbA1c (−15%, P < .001), total cholesterol (−9.0%, P < .001), LDL-C (−11.0%, P < .001), systolic BP (−7.7%, P < .001), and diastolic BP (−10.5%, P < .001). The improved glycemic control showed a significant positive correlation with the number of MDT visits but negatively correlated with BMI and the number of comorbidities. In addition, the improvements in secondary outcomes were positively and significantly correlated with such improvements in glycemic control.
Conclusion:
Case-manager-led MDT approach significantly improves glycemic control and significantly improves control over dyslipidemia and hypertension, reducing cardiovascular risks, and unfavorable events among such diabetic patients. We highly recommend developing more MDTs, training case managers, and rigorously evaluating the MDT approach.
Introduction
Approximately 6.28% of the population all over the world has type 2 diabetes mellitus (T2DM), with the incidence peaking at the age of 55 years and nearly equal gender distribution. 1 Diabetes is the tenth greatest cause of death, accounting for more than 1 million fatalities annually. 2 The prevalence of diabetes mellitus is increasing worldwide, and in developed nations, it is increasing considerably more quickly. The global prevalence of T2DM is expected to rise to 7.1% by 2030. 3
With an estimated population of 7 million people living with diabetes and more than 3 million with pre-diabetes, Saudi Arabia has the second-highest rate of diabetes in the Middle East and the seventh-highest rate worldwide, according to the World Health Organization. 4 Previous studies conducted in the Kingdom have estimated the prevalence of T2DM among adults to be between 18.2% in some provinces and 31.6% in the capital, Riyadh. Furthermore, the overall prevalence has been estimated to have risen from 23.7 to 25.4% of the Saudi population. 5
Along with the rising incidence of diabetes, a high prevalence of poor glycemic control has also been reported among diabetics. Alzaheb and Altamani 6 estimated that up to 74.9% of T2DM patients had inadequate glycemic control. Furthermore, diabetes is a very expensive ailment and is therefore prioritized in terms of public health. Diabetics face a variety of health challenges that necessitate the adoption and maintenance of healthy behaviors. 7 Diabetics, living with poor glycemic control, are at high risk for dyslipidemia, hypertension, and macrovascular complications. For the management of diabetes, the glycemic control and psychological health of those individuals are essential. The greatest option for reducing poor glycemic control and psychological concerns is to address these issues in the early stages of the disease. 8
T2DM is a chronic condition that necessitates continual interdisciplinary cooperation and patient self-management. 9 To address a person’s health needs, healthcare services are provided and coordinated through a collaborative process called case management. 10 The case manager-led Multi-Disciplinary Team (MDT) approach has been implemented in many countries faced with an increasing burden of caring costs for an increasing population with chronic diseases. One such example is that of Canada, where approximately 80% of healthcare costs may be attributed to around 10% of the population. Through the use of case management, the care of these patients may be better integrated and more efficient, thereby delivering greater patient satisfaction, better communication, and sharing patients in decision-making with their healthcare provider. 11
Various healthcare team members can give diabetes self-management training. The quality of services provided by various healthcare professions has not been clearly differentiated in a large portion of research comparing the effectiveness of discipline-based education. But according to published research, the multidisciplinary team members in charge of creating the curriculum and assisting in the delivery of care and education for diabetes should be the registered nurse, pharmacist, and registered nutritionist. 12 The largest and most dependable group of healthcare professionals are nurses. By acting as the link between theory and practice, nurses are uniquely positioned to spur positive improvements and transform healthcare delivery. 13 A study conducted in China revealed that adding simulation education and case management to routine self-management of diabetes effectively improved glycemic control in type 2 diabetic patients. 14
Several studies concluded that using multidisciplinary teams as a model of care delivery was associated with improved glycemic control, a major reduction in the cumulative incidence of complications related to diabetes, and a significant reduction in healthcare costs.11,15 -24
Riyadh First Health Cluster (RFHC), in Kingdom Saudi Arabia (KSA), started in 2020 to provide the case manager-led MDT approach among its primary healthcare centers toward improving care and follow-up of chronic diseases, especially diabetics. From 2020 up to 2022, a total of 21375 patients with T2DM were served and followed up every 3 months by MDTs throughout RFHC. Those suffering from diabetes have borne medical healthcare expenditures ten times, more than non-diabetics have. In Saudi Arabia, the direct costs of diabetes are nearly 13.9% of the total health expenditure. 4 Although current research seems to support the MDT approach to T2DM management, there are many obstacles to its adoption, including the rising prevalence of T2DM, limited resources, rising costs, poor team leadership, and communication. Therefore, there is an insistent demand to evaluate the MDT model’s efficiency if we were to improve diabetes intervention approaches for better glycemic control and reduction of diabetes-related complications and costs. 9 There are very rare studies with a small sample size conducted in Saudi Arabia, for evaluation of the effectiveness of the case manager-led MDT approach on glycemic control amongst T2DM patients. 15 Therefore, our study will be conducted on a larger sample, aiming to assess the effectiveness of implementing a case manager-led MDT approach in the primary healthcare setting on improving glycemic control and the cardiovascular risk profile of T2DM patients.
Methods
Study Design and Setting
This study was conducted as a multicenter retrospective record-based follow-up study on T2DM patients utilizing primary healthcare centers (PHCs) in Riyadh First Health Cluster in KSA during the period from January 2021 up to the end of 2022.
Target Populations
The populations targeted by the study are all patients with uncontrolled T2DM attending the primary healthcare centers in RFHC. A total of 21375 patients with T2DM were served by our MDTs among RFHC-PHCs. We focus on the primary healthcare setting, where most diabetic patients seek ongoing healthcare. The sample size was estimated to be (n = 549) at 80% power and a 5% margin of error to detect significant changes in A1C of 0.85 with the assumption of a 20% dropout rate.
To select the appropriate patients’ records (including high-risk patients) and to avoid confounding factors, they were identified according to certain inclusion and exclusion criteria. The inclusion criteria included all the uncontrolled T2DM patients (HbA1c > 8), older than 18 years old, who were receiving predominant usual care in primary care with no need for advanced diabetic care in secondary or tertiary hospitals. Patients were excluded if they were less than 18 years old, receiving long-term diabetic care in secondary care, patients with cancer or other similar complex conditions and/or limited life expectancy or complex disease, major disability or reduced mental capacity, and pregnant females.
Our study included the records of 3060 randomly selected patients out of 21375 T2DM patients, who were followed up every 3 months by MDTs over a period of 6 months. Incomplete records and drop-out patients were excluded.
Intervention Description (Case Manager-Led MDT Approach)
To deliver the best possible care for T2DM patients in the primary care setting and to ensure the standardization and consistency of the intervention provided, case managers were recruited, trained, and re-positioned in primary care from the existing nursing workforce. Each case manager led a multi-disciplinary team comprising a case manager, family medicine physician, chronic disease nurse, social worker, and health educator. The case managers work alongside primary care physicians (PCP) and health coaches to maintain an ongoing connection with study participants that includes direct therapeutic interventions, cooperation with their physicians, and motivational interviewing.
Patients were followed by a case manager every 3 months through a clearly defined pathway. Each case manager has approximately 100 patients to follow up with through the intervention. The studied patients continued to consult their PCP, as usual, every 3 months and also met with the case manager. The case manager also used phone or WhatsApp calls to follow up if patients attended any other appointments as needed to improve compliance with care plans and accessibility of health advice and information.
Basic information and knowledge about diabetes and its complications, glucose monitoring, insulin administration, and proper nutrition were taught to our participants. In addition, the case manager-led MDT assisted the patient in selecting appropriate choices for developing plans to achieve better glycemic control and to evaluate the progress of their condition. This included sound dietary habits, regular exercise of 30 min 5 days a week, adherence to their medication, and regular monitoring of HbA1c. Case managers also provide advice on the most suitable place to receive care if the patient has a complication, such as a diabetic foot.
In addition to this, the case managers ensured any annual screening was done and ensured early intensification of glycemic therapy where patients were demonstrating elevated blood glucose readings or symptomatic hyperglycemia.
Data Collection
Data collection tools and tracking of patient glycemic control
The patient sheets recorded by the case manager at baseline and 6 months after the intervention, had been reviewed and analyzed to compare glycemic control and secondary outcomes before and after the intervention. Case managers keep updated data about their patients, and these data include:
(I) The demographic and baseline characteristics (age, gender, BMI, disease duration, type of therapy, associated comorbidities, and the number of visits to MDT).
(II) Data on clinical parameters over time (HbA1c, LDL-C, total cholesterol, and BP). They were collected at baseline and 6 months after follow-up.
(III) Patients’ unfavorable events during the 6 months of follow-up (hypoglycemia episodes, ER visits in the last 3 months, and unplanned hospital admission).
Testing the study outcomes
This study’s outcomes include the percentage change in mean HbA1c, BP, LDL, and total cholesterol levels for detecting the overall improvement in each parameter. Then, to identify the percentage of T2DM patients showing different levels of improvement, we calculated the proportion of patients that reached the goal for HbA1c, BP, LDL, and total cholesterol. Our goals include HbA1c (less than 7% will be considered controlled, and from above, 7% up to <8% will be considered partially controlled), and BP less than 140/90 will be considered controlled. LDL < 100 mg/dL (2.6 mmol/L) and total cholesterol < 200 mg/dL (5.2 mmol/L) will be considered controlled. The patients’ glycemic control and secondary outcomes at baseline and 6 months after the intervention were compared.
Statistical Analysis
Data coding and analysis were performed using Statistical Package for the Social Sciences Version 21. Descriptive statistics were used to summarize the data, including the mean and standard deviation for quantitative outcomes and frequency tables for qualitative variables. The difference in quantitative clinical outcomes, comprising HbA1c, LDL, total cholesterol, and BP, before and after the intervention was compared using the paired t-test. While the chi-square test was used to compare qualitative variables. Correlations between glycemic control and other variables had been tested using the Pearson correlation coefficient (r) and Spearman’s correlation as needed. Two-sided tests will be used for all equality tests, and the test results are considered significant if (P ≤ 5).
Results
The final analysis in this study included the recorded data of 3060 patients with uncontrolled T2DM. The sociodemographic characteristics and clinical data of the studied T2DM patients are described in Table 1. Their mean ages were 52.6 ± 12.1 years (range 21-82 years), and 65.6% of them were females. The majority of participants have a high body weight with a mean BMI of (31.2 ± 1.7), and nearly two-thirds of them were either hypertensive or had dyslipidemia (43.4% and 47.3%, respectively). Our patients had uncontrolled T2DM (HbA1c > 8) and elevated blood pressure levels, with a mean duration of DM of 12.3 ± 10.6 years. The patients in our study had significantly higher use of oral hypoglycemic therapy alone (51.4%) versus (14.2%) for insulin use only, while 34.4% of them used mixed insulin and oral hypoglycemic therapy. During the 6 months of follow-up, they had a mean total number of visits (4.3 ± 1.1) to a case manager, physician, and health educator. In addition, 18.3% of patients had hypoglycemia episodes, only 2.3 % of them needed ER visits in the last 3 months, 1.1% were subjected to unplanned hospital admission, and nearly one-third of them (36.5%) were referred routinely to hospitals.
Demographic Characteristics and Clinical Data of the Studied Patients (N = 3060).
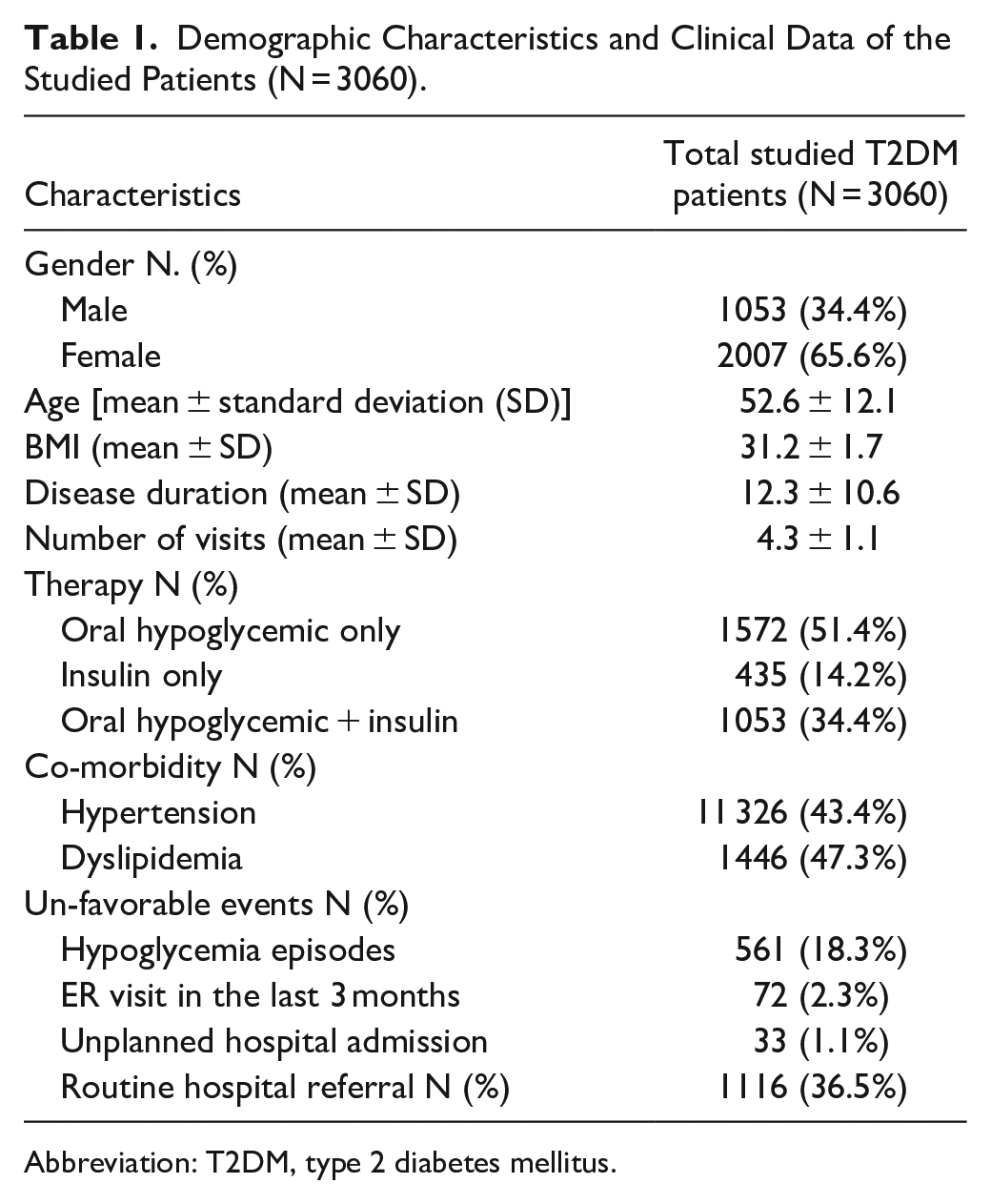
Abbreviation: T2DM, type 2 diabetes mellitus.
The changes in HbA1c in the studied group are further illustrated in Figure 1. It shows a clear reduction in the number of participants having HbA1c ≥8% (from 3060 at enrollment to only 1836 participants after 6 months of MDT intervention). This was accompanied by significant improvement in glycemic control among 1971 patients (64.4%), ranging from optimal control and partial control up to slight control (20.3%, 19.7%, and 24.4%) of patients, respectively. On the other hand, about 35.6% of participants showed no improvement in glycemic control.

Glycemic control among the studied group after 6 months of MDT follow-up.
The baseline and final levels and changes in our study outcomes are presented in Table 2. After 6 months of MDT intervention, a significant reduction in mean levels of different outcomes was detected among the studied patients. The percentages of changes relative to the baseline in their mean levels of HbA1c (−15%, P < .001), total cholesterol (−9.0%, P < .001), LDL (−11.0%, P < .001), systolic BP (−7.7%, P < .001), and diastolic BP (−10.5%, P < .001).
The Overall Impact of Case Manager-Led MDT on Glycemic Control, Serum Lipid Control, and Blood Pressure Control After 6 Months of MDT Follow-Up.

P ≤ .05 is significant.
As shown in Table 3, the MDT approach significantly impacted the improvement of hypoglycemic control, total cholesterol, LDL, and blood pressure control (P < .001). Nearly 2/3 of the studied T2DM patients achieved improved hypoglycemic control and a reduction of LDL (64.4% and 62.5%), respectively. Moreover, about three-fourths of our patients expressed a reduction in total cholesterol level and better blood pressure control (76.7% and 72.8%), respectively.
Percentage of Improvement in HbA1c, Total Cholesterol, LDL, and Blood Pressure Among the Studied Patients After 6 Months of MDT Follow-Up.
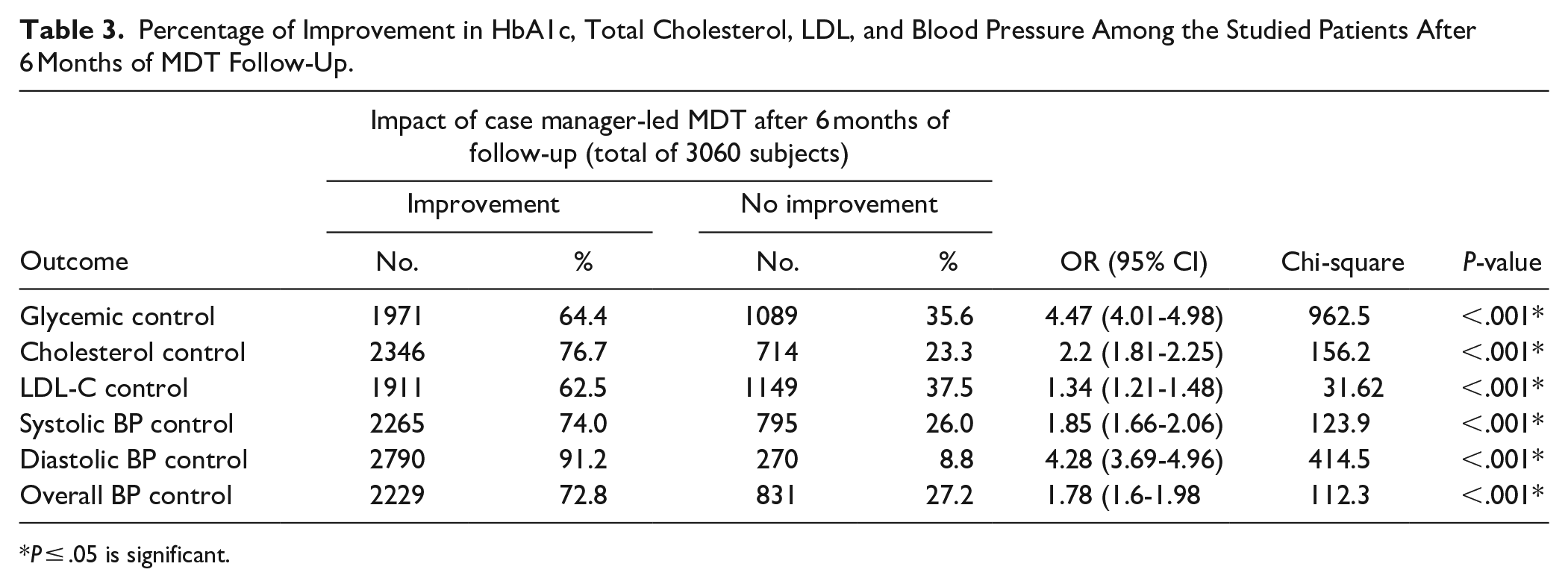
P ≤ .05 is significant.
The potential correlations between the improvement in glycemic control (HbA1c) and its impact on the improvement in other different outcomes were examined in Table 4. Among the studied group, the reduction in total cholesterol, LDL-C, systolic BP, and diastolic BP levels was positively and significantly correlated with such improvements in glycemic control. In addition, the improved glycemic control was positively and significantly correlated with the frequency of MDT visits with their case managers, but it showed a significant negative correlation with BMI and the number of associated comorbidities (Table 4).
Correlation Between the Pre-Post Changes in HbA1c Levels and Cholesterol Level, LDL Level, Blood Pressure, BMI, Number of MDT Visits, and Comorbidities.
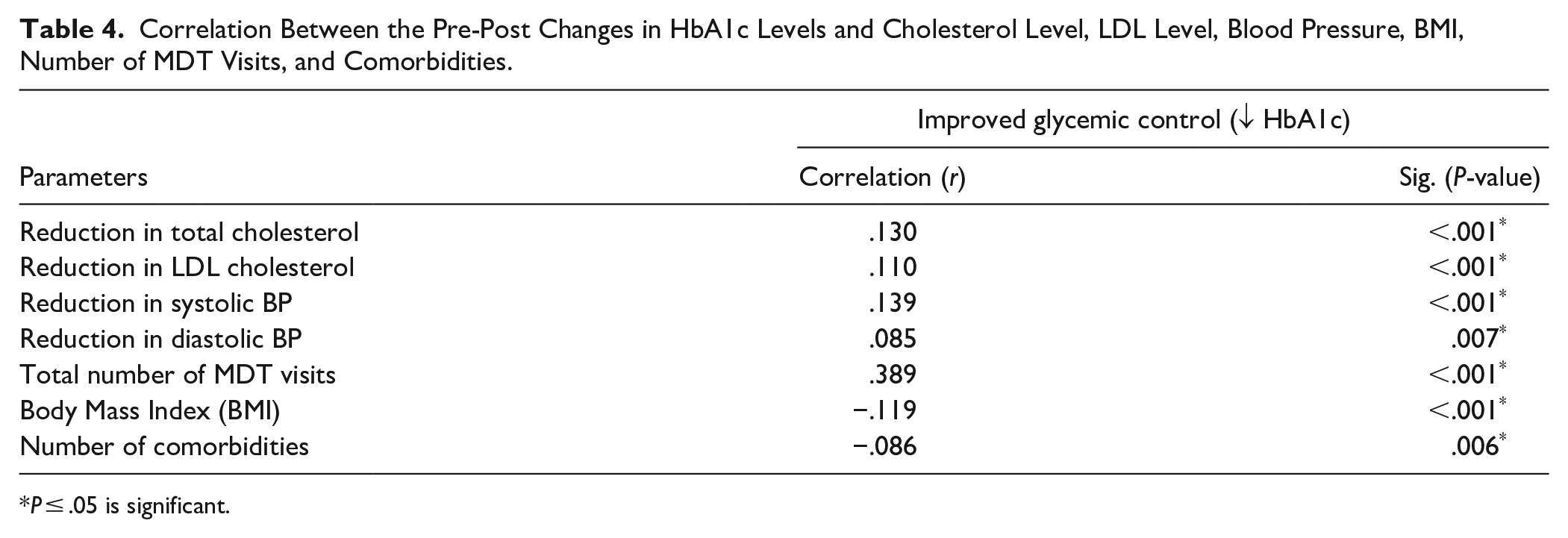
P ≤ .05 is significant.
Discussion
Case Manager Led Multi-Disciplinary Team is a relatively new approach to developing and improving the control of patients’ health, particularly those with chronic diseases. 16 An integrated MDT approach was achieved in the Riyadh First Health Cluster in KSA to improve diabetic care for patients with poorly controlled T2DM. In this study, we evaluated the theory that the case manager-led MDT approach is effective in improving hypoglycemic control and clinical outcomes among T2DM patients.
Among the studied 3060 patients with uncontrolled T2DM, the mean age was 52.6 ± 12.1 years, and 65.6% of them were female. This is nearly similar to the study of Tourkmani et al 15 in KSA and that of Azami et al 17 in Iran, where the mean age of their studied groups was (56.9 ± 12.0 and 56.0 ± 11.1 years) respectively. In addition, they noticed that about two-thirds of their patients were females. Concerning anti-diabetic treatment, 51.4% of patients in our study were under oral hypoglycemic therapy, 14.2% were under insulin use, and 34.4% of them used mixed insulin and oral hypoglycemic therapy. This is in agreement with the study of Ni et al 16 in China. On the contrary, Taïeb et al 18 in Tunisia found that nearly two-thirds of their patients are under insulin therapy.
In the present study, we assessed the effectiveness of the case manager-led MDT approach for the management of poorly controlled T2DM patients. The participants in our study showed significant improvements in glycemic control. Our results revealed a significant decrease of −15.0% in the mean HbA1c level through a regular follow-up by MDT over a period of 6 months. Almost 64.4% of our patients showed a significant reduction in their HbA1c, which was more than some other studies’ results. However, the detected reduction in HbA1c in our study was lower than in another study, with an absolute difference of 3.7. 15 This difference in HbA1c reduction among different studies could be interpreted by the differences in relative glycemic control at enrollment and the difference in the duration of follow-up from one study to another.
In agreement with our study, many other studies reported the effectiveness of implementing the MDT approach in primary care settings for the treatment of poorly controlled T2DM patients. These studies concluded that the MDT approach improves glycemic control and reduces cardiovascular risks among such patients.15 -24
A prior study conducted by Valle Nascimento et al 25 in Brazil discovered favorable outcomes among patients with chronic illnesses such as DM, and the overall reduction in this period was −0.338. In another systematic review conducted by Berhe et al 8 evaluating the use of motivational interviewing among patients with type 2 diabetes mellitus, three studies revealed that motivational interviewing significantly improves the mean HbA1c in the intervention group.
On the contrary, a study by Celano et al 26 found no statistically significant differences in the mean HbA1c as its level dropped from 8.87% to 8.48% during the study period. Furthermore, a study by Ismail et al 27 illustrates that training nurses on supporting self-management has not been associated with improvements in glycemic control, or any secondary outcomes, among T2DM patients.
In the present study, dyslipidemia and hypertension were found to be the main co-morbidities associated with T2DM among our patients. These findings are supported by the findings in many other studies. A new study conducted in China concluded that only 25.4% of the patients in the research group have hypertension. 28 On the contrary, a randomized, controlled interventional study presented the comorbidity for T2DM patients as 30.3% for hypertension and 46.2% for dyslipidemia. 15 In patients with T2DM, hypertension, and hyperlipidemia are frequent co-morbidities. The risk of problems related to diabetes can be decreased by maintaining constant glycemic control, decreasing blood pressure, and improving blood lipid profiles.
Moving to our secondary outcome, the present study revealed significant improvement in blood pressure, LDL cholesterol, and total cholesterol level control after MDT follow-up for 6 months. The mean levels of secondary outcomes were significantly reduced, including total cholesterol, LDL, systolic BP, and diastolic BP, by (−9.0%, −11.0%, −7.7%, and −10.5%) respectively. In addition, the reduction in total cholesterol, LDL, systolic BP, and diastolic BP levels is positively correlated with the improvement in glycemic control. Few studies have examined patient improvement in these variables. These findings are consistent with a study conducted by Nascimento following up on T2DM patients for 6 months and reporting a significant improvement in LDL and cholesterol. 25 Moreover, a study done in China evaluating multi-disciplinary teams detected significantly reduced total cholesterol and LDL-C levels among the studied participants after the intervention. 28
Our study revealed that patients’ number of visits positively affected the improvement in glycemic control. While glycemic control showed a negative and significant correlation with BMI and the number of comorbidities. In agreement with our study, Tourkmani et al 15 found that glycemic control was positively correlated to the frequency of visits among the studied group but negatively correlated with the number of comorbidities, which explains the improvements in patients’ HbA1c.
The participants in our study have increased body weight with a mean BMI of (31.2 ± 1.7). This mean BMI is in line with the study of Taïeb et al 18 in Tunisia and the study of Tourkmani et al 15 in KSA, higher than that in the study of Azami et al 17 in Iran and lower than that noticed in the study of Yu et al 28 in China.
However, there are no noticeable changes in BMI among our patients, and this may be a result of the short duration of this study, so we cannot find a significant change in BMI. A prospective observational study was conducted in France in line with our study. They concluded that there were no significant differences in BMI after a 12-month follow-up period. 18 However, another study, conducted by Azami et al 17 in Iran, found that after the intervention, the reduction success rate in BMI among the research group was 61.19%. These results emphasize the importance of weight reduction for better glycemic control, as HbA1c levels have a negative correlation with BMI.
In this study, we noticed a minimum of unfavorable events during the 6 months of follow-up. The main noticeable event was hypoglycemia episodes in 18.3% of patients during the study period. While the ER visits in the last 3 months and unplanned hospital admissions were very low (2.3% and 1.1%), respectively. In agreement with our finding, a case-control study by Ni et al 16 revealed a significant decrease in hospitalization among the interventional group when compared to the control group. Moreover, an Iranian study shows that none of the patients reported any adverse events, confirming the success of the intervention. 17
The current study provides a new vision of a case manager with a multidisciplinary team that targets diagnosed T2DM patients. Furthermore, the study tested patients’ results before and after the intervention. The result indicates that the approach used in primary health care centers (PHCs) was sufficient and improved the patient’s outcomes in terms of reducing HbA1c levels and cardiovascular risk.
Limitations of the Study
The absence of a control group is the main limitation of this study. However, we overcome that by pre- and post-evaluation of participants in our study. Another limitation is the short duration of this study, which does not account for secular trends, and we could not find a significant change in BMI. In addition, the retrospective nature of this study and the use of the participants’ recorded responses could possess some sort of bias. Finally, this study is a single-cluster project evaluation in only the Riyadh region, so caution is advised in generalizing some study findings in different countries.
Further multi-national research is recommended, considering more than one country, for better generalization of findings.
Conclusion
Our study concluded that the case-manager-led MDT approach has significantly improved glycemic control and its secondary outcomes among T2DM patients. It reduces the levels of HbA1c, total cholesterol, LDL, and blood pressure. In addition, proper glycemic control significantly improves control over dyslipidemia and hypertension, reducing cardiovascular risks and reducing unfavorable events among such diabetic patients. We strongly suggest maintaining a sufficient number of routine MDT visits, and we emphasize the importance of BMI reduction for better glycemic control among patients with T2DM. To enforce efforts, to fully meet this potential, we recommend developing more MDTs, providing more training for case managers, and rigorously evaluating the MDT approach over a longer period. In addition, we highly recommend the conduct of further research to assess the cost-benefit of such an MDT approach and its impact on reducing the costs of healthcare services delivered to diabetics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.