
Abstract
Purpose:
To assess differences in mental health screening based on patient’s preferred language.
Methods:
For this retrospective cohort study, data for 85 725 unique patients from 10 primary care clinics in West Michigan were analyzed if patients received at least 1 mental health screening with the Patient Health Questionnaire 4 (PHQ-4) within a 12-month period (10/15/2021-10/14/2022). A general linear regression model was used to assess the adjusted odds ratios (aOR) of being screened.
Results:
Patients having a preferred language other than English (n = 2755) had an 87.0% chance of receiving the recommended mental health screening, compared to 76.7% of English-speaking patients (P < .001). A multivariable model revealed decreased screening odds for Kinyarwanda (aOR 0.29, 95% CI 0.19-0.45) and Persian/Dari/Pashto (aOR 0.46, 95% CI 0.23-0.91) speaking patients and higher screening odds for Spanish (aOR 1.45, 95% CI 1.19-1.77), Bosnian (aOR 2.13, 95% CI 1.11-4.11), and Vietnamese (aOR 2.25 95% CI 1.64-3.08) speaking patients compared to English speaking patients.
Conclusions:
Results highlight the inequities between the language groups that are probably the result of the challenges to access multilingual depression and anxiety screening instruments. Furthermore, providers may be prone to bias about who they think “needs” a mental health screening. We suggest that measures are implemented to ensure consistency in mental health screening regardless of a patients’ preferred language.
Keywords
Introduction
Depression and anxiety are serious health conditions that are associated with increased mortality, worsening of chronic medical conditions, functional disability, increased healthcare utilization, 1 and impaired quality of life. Many people who speak a language other than English and are settling in the United States are migrants, refugees, and displaced persons. They are considered to be particularly affected by depression, 2 post-traumatic stress disorder, and other mental health problems.3 -5 Migrants may be exposed to adverse or even traumatizing events during or after their migration.6 -8
In 2016, the United States Preventative Task Force (USPSTF) released a recommendation to provide consistent depression screening in primary care settings for all adult patients. 9 Recently, the USPSTF expanded its recommendations to screen for suicidal ideation and anxiety symptoms. 10 The Center for Disease Control and Prevention (CDC) has highlighted the role of primary care providers in providing basic mental health care to resettled populations and has underlined the importance of consistent screening as mental health symptoms can occur months or years after resettlement. 11 Despite the recommended domestic medical examination within 90 days of arrival in the United States, only a minority of eligible subjects received mental health screening. 12 This highlights the key role of primary care providers in consistently screening for mental health problems among newly arrived people. Research has shown that screening, detection, and subsequent early treatment of depression decrease clinical morbidity, 9 improve quality of life, and decrease healthcare costs.13,14 Racial and ethnic minorities as well as refugees benefit from consistent screening likewise.15 -18
Other studies have shown varied mental health screening rates between 59% 19 and 88.8%. 20 While some authors have found racial disparities in mental health screening21,22 and lower rates among patients with a preferred language other than English or Spanish, 20 little is known about mental health screening practice by language groups. This study aimed to assess mental health screening disparities among patients’ preferred language in a primary care setting.
Methods
In this retrospective cohort study, data from patients in 10 urban primary care clinics in West Michigan were analyzed. The study was deemed non-human subjects research by the decision of the Corewell Health institutional review board (#2022-342). Study results were reported in accordance with the The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 23
Setting
The Michigan based Corewell Health system comprises 22 hospitals and over 300 outpatient facilities in a large non-profit managed healthcare organization. This study was conducted in the Grand Rapids-Kentwood-Muskegon-Combined Statistical Area which is home to 1.4 million people. While important characteristics like household income are similar to the overall United States ($69 643 vs $69 717) the proportion of the foreign-born population is lower than that of the overall population (5.7%vs 13.6%). Despite this difference, West Michigan is home to many refugee communities, especially from sub-Saharan Africa (Rwanda, Democratic Republic of Congo) and East Asia (Myanmar).
Sample
This sample consists of all unique patients aged 16 and older who established care at one of the respective clinics and had at least 1 office visit between 10/15/2021 and 10/14/2022. A few patients who had only urgent care and pure clinical resource visits (eg, appointments for immunization) were excluded (Figure 1). No other inclusion or exclusion criteria were applied. Corewell Health’s honest broker performed data extraction from Electronic Medical Records (EMR, Epic HYPERSPACE, Epic Systems Corporation, Verona WI, USA) and provided de-identified datasets to the researchers.

Flow chart of patient inclusion.
The clinics were selected to match with different refugee and migrant communities in the region. The maximum number of clinics to include was suggested by Corewell Health’s Sensitive Data Sharing Workgroup to ensure that data extraction did not impede operability of the EMR system. The primary care clinics were primarily large clinics with a mean of 8581 (SD 6227, min 1251, max 22 059) served patients during the 12-month study period. These clinics comprise a total of 103.8 provider full time equivalent positions.
Primary Outcome
The primary outcome was defined as unique individuals receiving at least 1 mental health screening during the 12-month study period. Corewell Health introduced regular mental health screening in their primary care clinics using the Patient Health Questionnaire (PHQ-4) 24 in June 2017. This policy highlights screening “every patient age 18 or older at every visit.” Repeat screening were not deemed necessary if a patient was screened within the last 2 weeks. The PHQ-4 comprises 4 questions each targeting the main diagnostic criteria for depressive disorder and generalized anxiety disorder in accordance with Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM 5-TR). 25 The PHQ-4 is widely used in both research and patient care and has been validated among various populations and languages, 26 and has proven its usability among refugee and migrant patients. 27
Covariates
The requested dataset contained additional information on patients’ sociodemographics, including age (at first encounter), sex, preferred language for encounter (assessed by office staff, typically indicate need for interpreter service), and health insurance type (private insurance, no insurance, Medicare, Medicaid). Preferred languages other than English were grouped into the 10 most common languages or regions where they are predominantly spoken. While the groups “Kinyarwanda,” “Vietnamese,” “Nepali,” and “Spanish” only entail people with the respective preferred language, the “Persian/Dari/Pashto” group also comprises a small group speaking Urdu and thus reflect languages spoken mainly in Iran and Afghanistan. Likewise, the “Burmese” group comprises Chin Hakha, Karen Languages, Tamil, Rohingya, Kayah, Tedim, and Falam and therefore reflects languages and sub-dialects that are spoken in Myanmar. Also, we assigned Serbian language to the “Bosnian” group and Sudanese Arabic to “Arabic.” The “other European languages” group comprises French, Albanian, Portuguese, German, Greek, Polish, Italian, Dutch, Hungarian, Romanian, and Latvian, but not Bosnian, English, or Spanish speakers.
The following chronic conditions that are associated with higher mental health burdens were also included in analyses when they occurred during or before the study period: diabetes mellitus, 28 chronic ischemic heart disease, 29 chronic rheumatic/inflammatory condition, 30 malignancy and cancer, 31 and mental health diagnoses except tobacco use. We also recorded if patients had a preventive appointment for example, well child visits for 16 to 21 year-olds, annual physical or Medicare Annual Wellness Visits 32 during the study period as screening for mental health problems would be expected at these appointments.
Statistical Analyses
First, descriptive statistics (absolute and relative frequencies, mean, standard deviation [SD]) were used to characterize our sample stratified after preferred language of encounter (English and non-English). To test the independence between language groups and other categorical or continuous variables, the Chi-Square or Mann-Whitney-U test was used, where applicable. In all tables, missing values are reported.
Second, unadjusted mental health screening prevalence with corresponding 95% confidence intervals (95% CI) is reported for sociodemographic and disease-related factors as well as preferred language. Forest plots were built using GraphPadPrism 9.5 (GraphPad Software, San Diego, CA, USA).
Third, a multivariable analysis was conducted. We used a general linear model with logit link function to assess the association between preferred language on mental health screening while adjusting for sociodemographic factors (age, sex, health insurance), frequency of encounters, preventive encounters, chronic conditions (diabetes mellitus, chronic ischemic heart disease, cancer diagnosis, mental health diagnosis) and the respective clinic. The binary outcome was defined as receiving at least 1 mental health screening within the 12-month study period. Results for different languages are reported as adjusted odds ratios (aOR) with corresponding 95% with English speaking patients as reference. A table reporting aORs for all non-language covariates can be found in the Supplemental Appendix.
All statistical analyses were carried out using SPSS 28 (IBM, Armonk, NY, USA) and P values <.05 were considered significant.
Results
After applying exclusion criteria, n = 85 725 patients with a total of 184 503 encounters during the study period were analyzed (Figure 1).
Patients in our sample were between 16 and 104 years old (mean 51.0 years, SD 18.9) and 58.4% were females. In total, 3.2% (n = 2755) patients had a preferred language other than English. These patients preferred 1 of 62 different languages, with Spanish (40.3%), Vietnamese (27.3%), Bosnian (5.8%), Kinyarwanda (4.0%), Nepali (3.2%), and Burmese (2.8%) being the most prevalent.
While sex and mean age did not differ significantly between English-speaking and patients with a language other than English, the proportion of 36 to 55-year-olds was somewhat higher among the latter group. Patients with a language preferred other than English also had more encounters with primary care providers during the study period (mean 2.4vs 2.1 among English-speaking patients, P < .001) and were less often insured through Medicare (18.1%vs 29.1% among English speaking patients, P < .001). While diabetes mellitus was more prevalent among patients with a preferred language other than English, (22.5%vs 13.5%, P < .001), other chronic conditions like chronic ischemic heart disease, chronic inflammatory/rheumatic condition, malignancy/cancer, mental health problems were less common (all P < .001, see Table 1).
Characteristics of Enrolled Subjects.

English versus language other than English, Chi-square test/Mann-Whitney U test, where applicable, missing language n = 89.
Missing sex n = 2.
“Other” includes Native Hawaiian or Other Pacific Islander, missing race n = 2286.
Missing ethnicity n = 1907.
For each encounter, English-speaking patients had a 63.2% likelihood (95% CI 63.0-63.5) of completing the screening, while those with a preferred language other than English had a likelihood of 72.6% (95% CI 71.5-73.7). Within a year, 76.7% of English-speaking patients received a screening (95% CI 76.3-76.9), and 87.0% of patients with a preferred language other than English (95% CI 85.7-88.2) received a screening. However, there were considerable differences between the preferred languages, with screening prevalence rates from 60.6% (Kinyarwanda) to 94.0% (Vietnamese). Also, differences in screening rates were observed among different ethnic and racial groups, type of insurance, number of encounters, and if a patient had a pre-existing conditions (Figure 2).
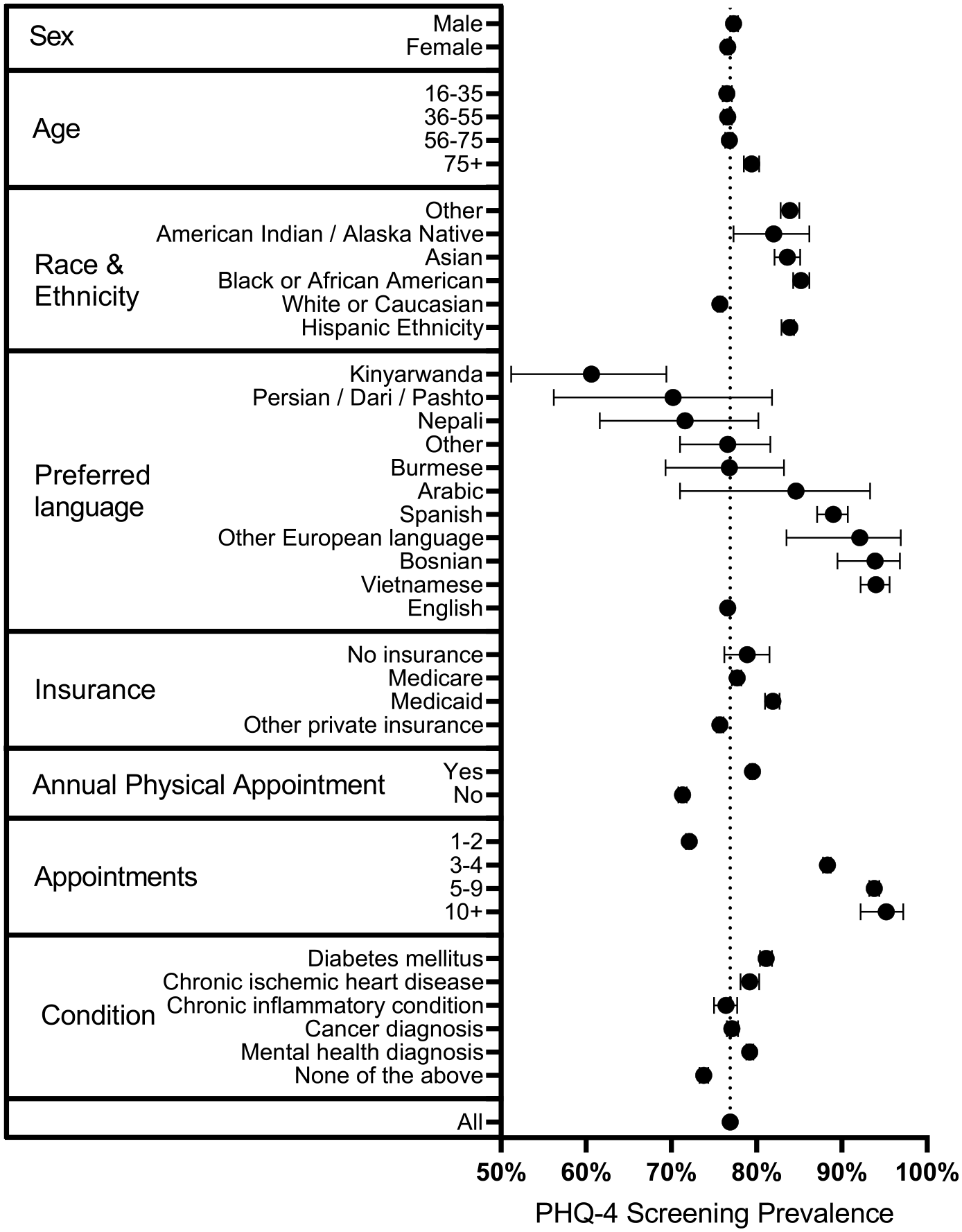
Unadjusted PHQ-4 screening prevalence rates (with 95% confidence intervals).
Finally, we performed a binary logistic regression analysis with logit link function (n = 85 723 subjects) with the dependent variable “receiving at least one PHQ-4 screening within the 12 months study period” (Table 2). The analyses revealed significant lower odds to receive a screening for patients with a preference of Kinyarwanda and Persian/Dari/Pashto language, and higher odds for patients with a preference of Spanish, Bosnian/Serbian, and Vietnamese language compared to English-speaking patients. Adjusted odd’s ratios of all covariates are shown in the Supplemental Appendix.
Adjusted Odds Ratio’s Among Preferred Languages.

Discussion
In this retrospective cohort study, we found that patients having a preferred language other than English had higher chances of receiving the recommended mental health screening compared to English-speaking patients. The difference between both groups of receiving a mental health screening within the 12-month study period was 10.3% (76.7% English vs 87.0% non-English). This conclusion changes when stratified for different languages: a multivariable model revealed considerably lower screening odds for Kinyarwanda and Persian/Dari/Pashto speaking patients and confirmed higher screening odds for Spanish, Bosnian, and Vietnamese speaking patients compared to English speaking patients.
A cohort study involving 52 944 patients from 6 primary care facilities in San Francisco, California, conducted before the Coronavirus disease 2019 (COVID-19) pandemic, reported similarly higher screening odds for Spanish-speaking patients but lower odds for Chinese-speaking patients and patients with other non-English language preferences. However, these differences were not consistent after the introduction of a general screening policy. 20
Availability of Validated Mental Health Screening Instruments
A key prerequisite to conducting a mental health screening in non-English speaking patients is access to validated and culturally adapted screening instruments for the respective language. 33 The official repository for the widely used PHQ-4 or the more comprehensive Generalized Anxiety Disorder 7 questionnaire (GAD-7) 34 and Patient Health Questionnaire (PHQ-9) 35 is the website “PHQ screeners” 36 by the pharmaceutical company Pfizer. While GAD-7 and PHQ-9 screeners are provided in more than 50 languages, the PHQ-4 is mostly unavailable in any other languages than English. For example, of the language groups in our sample, the PHQ-9/GAD-7 was only available for Spanish, Arabic and some other European languages at this website.
Furthermore, providers would need to compile their own PHQ-4 out of the available GAD-7 and PHQ-9 screeners, however these “self-made” instruments are not validated. Eventually, clinics may be unprepared to screen patients using the PHQ-4 because of the added effort that must go into creating translated copies. Other options for providers to gain access to validated screening instruments are through a research of PubMed or other databases. While many surveys are not validated for the particular purpose another major obstacle is that many instruments are either not included in the manuscript37,38 or are published under a non-open access license.39,40 Lastly, for some languages (including Kinyarwanda, Pashto) there have not been attempts to translate and validate instruments such as the GAD-7 or the PHQ-9. This is probably the main reason why Kinyarwanda and Pashto speaking patients are the least likely to receive a mental health screening. This is all the more concerning as the vast majority of these patients have fled from areas of armed conflict and have a correspondingly high risk for unrecognized mental health problems.41,42 Conversely, for those language where translated and validated screenings instrument were available, higher screening rates were apparent.
Another option for conducting mental health screening among patients where no screening instrument is available is to instantly interpret the English version of the instrument by an interpreter. While this pragmatic approach is neither quality assured nor recommended, it allowed some of the Kinyarwanda speaking patients in our cohort to receive a mental health screening. Furthermore, this requires consistent access to well-trained culturally competent interpreting services that are familiar with mental health, which are often unavailable in primary care settings. 43
Reluctancy to Screen and Provider’s Implicit Bias
Besides barriers in accessing screening instruments, providers may be reluctant to screen for various reasons. Although primary care providers can identify approximately half of their depressive patients when no psychometric instrument is used, 44 many providers still decide on who receives screening on a case-by-case basis 45 or the perception of “knowing a patient personally.” 46 Other barriers include lack of comfort in treating patients with mental health problems. 47
Furthermore, providers may face limited capacities to refer non-English speaking patients to culturally and linguistically competent mental health treatment. Given the widespread shortage of mental health providers, there may also be a barrier for non-English speaking patients to receive the necessary care.48,49 The CDC recommends that providers that regularly provide care to refugee patients should foster a good working relationship with refugee resettlement agencies and their mental health support structures. 11
Despite this, mental health assessment is necessary for primary care providers to evaluate if somatic symptoms and ailments are originating from a mental health concern. 11 As cultural variations in the clinical presentation of psychological distress may occur, providers who do not screen for mental health may misinterpret cultural idioms of distress which may lead to unnecessary tests or inappropriate treatment.50,51
Patients with the preferred languages Spanish, Bosnian, or Vietnamese in our studies had an increased likelihood to receive a screening compared to non-English speakers. Refugee intake and migration from the region where these languages are spoken occurred decades ago, for example, through the “Indochina Migration and Refugee Assistance Act” 52 from 1975 or the acceptance of Burmese and Bhutanese refugees in 2018. 53 Conversely, those with rather low screening rates are rather new to the US: For example, refugees from the Democratic Republic of Congo were by far the largest refugee group admitted to the US in 2019. 53 It is conceivable that clinics providing care to those patients developed workarounds over time and that decades of ongoing patient-provider relationships diminished hesitancy in bringing up mental health as a topic. As there is a high and growing number of Spanish speakers in the U.S. (approximately 41.8 million people), it is similarly likely that clinics are prepared to provide mental health screening to this group. 54 While both would explain screening odds that are comparable to English speaking patients, it remains unclear why screening rates for Bosnian and Vietnamese speaking patients are twice as high compared to English speaking patients. This may reflect that providers acknowledge the increased risk for mental health problems among these populations or may be the result of increased diversity equity and inclusion initiatives to address mental health challenges. Researchers have also discussed providers’ implicit bias as a factor in diagnosing mental health conditions in minority populations. 55
Strengths and Limitations
Our study relies on EMR-data and thus on the documentation accuracy. It is possible, that clinic staff may have performed a mental health screening but not documented it or falsely indicated preferred patients’ language as “English.” However, this might only has happened in some few cases and would not have changed the results considerably.
Other limitations include that we could not adjust for the length a patient stayed in the US or the migration status (eg, refugee, resettled migrant, migrant with a non-permanent or permanent resident visa, naturalized US citizen, born US citizen) as this information was lacking. Furthermore, the clinics and patients included in the research are not representative of the entire U.S. population. For example, the proportion of White or Caucasian people was higher in our sample than in the overall U.S. population. However, a strength of this study is the large and complete sample of patients that were included from 10 primary care clinics. As those clinics encompass over 100 primary care providers, a considerable provider bias is unlikely.
Our study could not account certain patient-associated reasons for not receiving a mental health screening, such as illiteracy, or decline to complete screening. Due to the nature of retrospective study, we could also not assess if patients received translated screening instruments or if English instruments were instantly interpreted on site. Prospective observational studies can provide a deeper understanding of the actual mental health screening practice and might further inform strategies to enhance screening uptake.
Conclusions
Screening for mental health in primary care settings is a vital component of a routine health maintenance exam and should be performed for all patients, no matter the language they speak. Providers and clinics on the local level should be aware that populations newer to the area might be less likely to be screened for mental health disorders, despite their high risk. This awareness hopefully might translate into higher screening rates. On organizational level, an open access repository on publicly available, translated, and validated mental health screening instruments, multilingual digital tools that streamline the mental health screening process,56 -58 and efforts to culturally and linguistically diversify the healthcare workforce59,60 might further contribute to consistent mental health screening.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231200304 – Supplemental material for Mental Health Screening Differences in Non-English Speaking Patients: Results From a Retrospective Cohort Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319231200304 for Mental Health Screening Differences in Non-English Speaking Patients: Results From a Retrospective Cohort Study by Frank Müller, Alyssa M. Abdelnour, Diana N. Rutaremara, Judith E. Arnetz, Eric D. Achtyes, Omayma Alshaarawy and Harland T. Holman in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors want to thank the Corewell Health Office of Research and Education and the Corewell Health Honest Broker for their support. We acknowledge support by the Open Access Publication Funds of the Göttingen University.
Author’s Note
Prior presentation(s): This work has not been presented at any conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FM received funding as Peter C. and Pat Cook endowed clinical research fellow. OA is funded by the United States National Center for Complementary and Integrative Health [R00AT009156] and Michigan State University. The funding organizations had no role, in designing the study; collecting, analyzing, or interpreting data; or writing or submitting the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.