
Abstract
Aim:
Low- and middle-income countries represent nearly 85% of all cervical cancer cases worldwide; thereby, it is extremely important to identify methods to improve the screening process. Therefore, this study aimed to summarize the primary characteristics of studies on accessibility, coverage, patient preferences, and factors associated with patient satisfaction or acceptance of colposcopy in primary healthcare.
Methods:
A search strategy, based on MeSH, Emtree, and free terms, was run through 5 databases (PubMed, Scopus, Embase, Ovid/Medline, and Web of Science). EndNote 20.1 © and Rayyan QCRI © were used for screening. A preset datasheet was used for data extraction.
Results:
The systematic search retrieved 1127 references, and after removing duplicates, screening the titles and abstracts, and reviewing the full text, 7 studies were included. The interrater reliability was 77.73% (kappa statistic = 0.1842). Most studies estimated the proportion of women that sought for colposcopy after a previous screening test for human papilloma virus. One study identifies barriers to colposcopy examination in women at risk of developing cervical cancer. Three studies assessed the decentralization of colposcopy from a tertiary healthcare center to a primary care center. Pap smear was the most common first-line screening test, followed by liquid-based cytology sample and visual inspection with acetic acid.
Conclusion:
Only a few countries have investigated the use of colposcopy in primary care. Thus, barriers and the care structure for this implementation to be successful in reducing cervical cancer incidence and mortality should be identified.
Introduction
Low- and middle-income countries (LMIC) represent nearly 85% of all cervical cancer cases worldwide and 99.7% of all cervical cancer specimens are associated with high-risk human papilloma virus (HPV) DNA.1,2 Lemp et al 3 found that a median age of 43.6% of women was 30 to 49 years who have ever been screened for cervical cancer in LMIC. This number decreases in countries located in sub–Saharan Africa where the estimated prevalence for cervical cancer screening is 16.9%.
Globally, China and India account for 35% of the global burden and deaths from cervical cancer. The lowest incidence has been found in patients from West Asia (Qatar, Israel, Turkey, and Saudi Arabia), with <5 cases per 100,000 women. 4 In regions with LMIC, such as South America and the Caribbean, countries with the highest incidence of cervical cancer are French Guiana and El Salvador, with reported incidences of 29.7 and 28.9%, respectively. However, countries with the highest mortality were Belize and Paraguay (17.4 and 15.3%, respectively). 5 Globally, 341,831 women were estimated to die from cervical cancer in 2020; therefore, it is extremely important to identify methods to improve the screening process, especially in LMIC. 6
Several methods have been proposed to increase and improve cervical cancer screening since, as mentioned above, a large number of people never get screened and many of those who started the screening process do not complete the process. A study by Buss et al 7 demonstrated that only 39.8% of women with an abnormal cytological report undergo colposcopy. To increase participation, the population should be educated about the entire screening process and the places where it can be performed, as well as the decentralization of procedures such as colposcopy.
Decentralization of colposcopy from hospitals belonging to the second or third level of care at health centers of the first level of care can improve the population’s access to this type of service, in addition to reducing the workload of tertiary care hospitals without affecting the service quality. This is especially relevant in LMIC with limited-resource health systems where, despite the multifactorial barriers to accessing a colposcopy, access to health systems is one the most important.8,9 Considering that research is an ideal means to identify solutions to specific problems, various studies have evaluated aspects related to colposcopy in primary care. However, to our knowledge, no study systematized this evidence. Therefore, this study primarily aimed to summarize the main characteristics of studies on accessibility, coverage, patient preferences, and factors associated with patient satisfaction or acceptance of colposcopy for any gynecological diseases in primary healthcare.
Methods
Study Design and Report Guidelines
This scoping review was conducted based on methodological guidelines for this study type10,11 following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) for drafting our results. 12
Search Strategy and Databases
We followed the Peer Review of Electronic Search Strategies checklist 13 for constructing the search strategy, using MeSH, Emtree, and free terms. Afterward, it was adapted for all databases, without applying date or language restrictions. Hand searches or reference list reviews were not employed. The systematic search was simultaneously conducted on October 05, 2022, using the following databases: PubMed, Scopus, Embase, Ovid/Medline, and Web of Science (Core Collection). The complete search strategy is attached as Supplemental Material (Table S1).
Eligibility Criteria and Study Selection Process
The eligibility criteria were (i) primary or secondary studies assessing the (ii) accessibility, coverage, preferences of patients, associated factors with, satisfaction of patients with, or acceptance of colposcopy for any gynecological disease in (iii) primary healthcare. Case reports, case series, letters to editor, abstracts, and narrative reviews were excluded. All phases of the study selection process were independently screened by at least 2 authors. Duplicates were removed using EndNote 20.1 © and Rayyan QCRI ©. 14 The remaining references were exported to Rayyan for screening the titles and abstracts (CPEG, LMAC, and EAHB). After identifying the potential references to be included, 3 authors (CPEG, LMAC, and EAHB) independently assessed the full text of each one. Any conflict or discrepancy in any phase of the study selection process was resolved by consensus.
Data Extraction and Synthesis
Data extraction was independently performed by 4 authors (LMAC, CPEG, EAHB, and EAAB) using a standardized data extraction sheet created in Google Sheets ©. The following information was extracted: author, publication date, country, outcome, main results, and conclusions. Due to the heterogeneous nature of the study, only a qualitative synthesis was performed.
Evaluation of Risk of Bias
The risk of bias assessment of the included studies was performed with the Newcastle–Ottawa Scale (NOS) for cohort studies 15 and ROBINS-I for non-randomized studies of intervention. 16
The Newcastle–Ottawa tool consists of 3 domains (selection, comparability, and outcome) with 8 items for cohort studies. A star system is used, with the maximum possible of 9 stars. Studies with 0 to 3 stars have a high, 4 to 6 stars have a moderate, and 7 stars have a lower risk of bias.
The ROBINS-I tool has 3 domains (preintervention, intervention, and postintervention) with 7 items. Each item can be classified as low (green), moderate (yellow), and high risks (red). If any of the items is high risk, the study is considered to have a high risk of bias.
For the study implementation, a conceptual framework for implementation fidelity was used, consisting of 3 categories 17 : adherence (content, coverage, frequency, and duration), moderators (intervention complexity, facilitation strategies, quality of delivery, and participant responsiveness), and identification of essential components.
Results
Study Selection Process
A systematic search retrieved 1127 references and 860 duplicates were removed. The titles and abstracts of the remaining references were screened, with an interrater reliability of 77.73% (kappa statistic = 0.1842). Afterward, the full texts of 96 references were assessed by full text, and finally, 7 studies were included.7,18 -23 A detailed flowchart of the study selection process is shown in the PRISMA flow diagram (Figure 1), with standardized reasons of full-text exclusion.
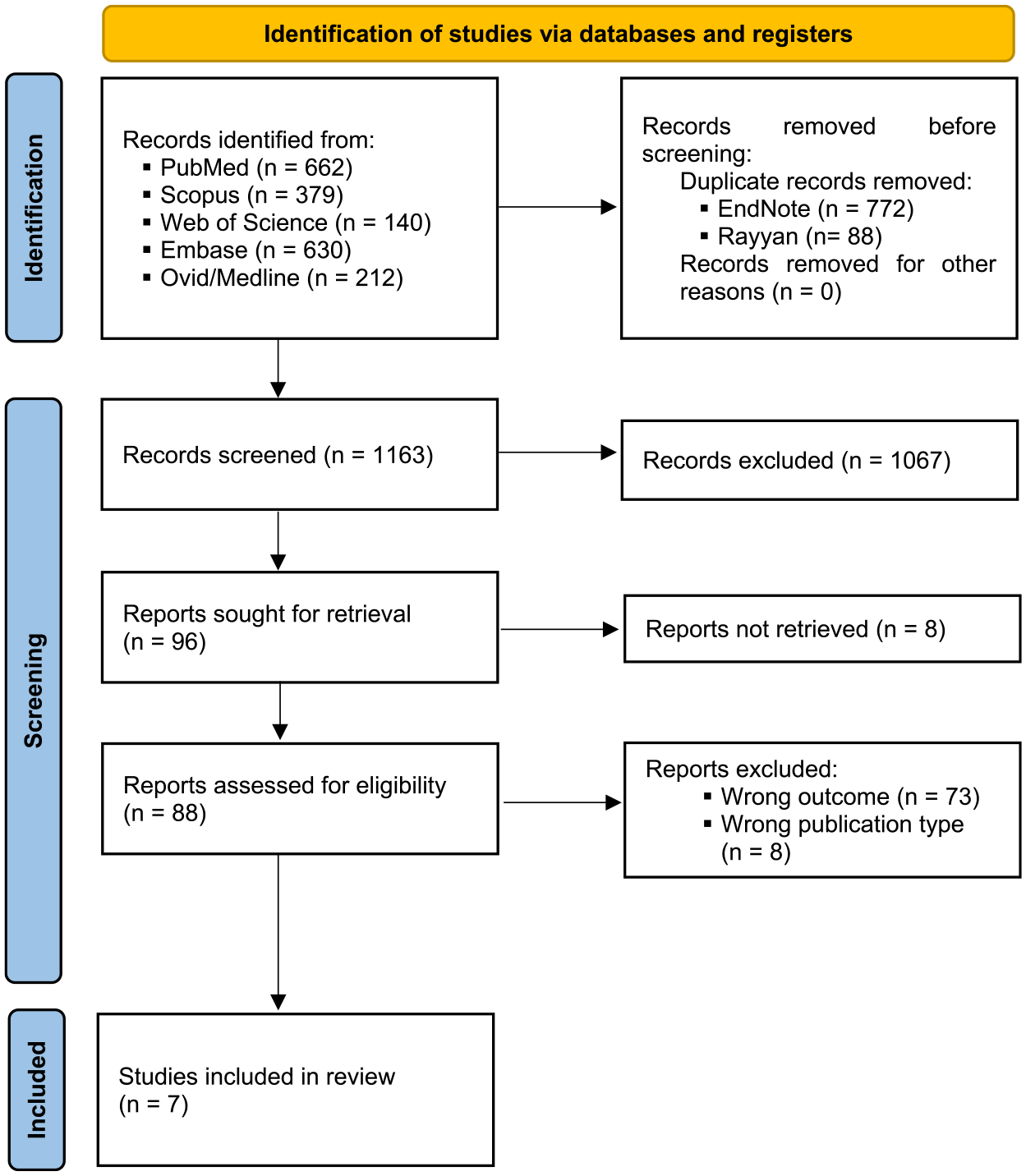
PRISMA flow diagram.
Characteristics of Included Articles
Table 1 presents the main characteristics and outcomes of the included studies. Five studies were cohorts.7,18,21 -23 As for the study location, 2 were conducted in Brazil,7,18 2 in South Africa,20,21 2 in Canada,22,23 and 1 in India. 19 The majority of women was ≥18 years, non-pregnant, and was previously screened with another HPV test. The most common first-line screening test was Pap smear,7,20 -23 followed by liquid-based cytology sample, 18 and visual inspection with acetic acid and HPV test using hybrid capture 2. 19 Most studies aimed to estimate the proportion of women who sought for colposcopy after a previous screening test for HPV.7,18,20,21,23 One study identifies barriers to colposcopy examination in women at risk of developing cervical cancer. 22 Three studies assessed the decentralization of colposcopy from a tertiary healthcare center to a primary care center.20,21,23
Characteristics of Included Studies.

Abbreviations: hr-HPV, high-risk HPV; LBC, liquid-based cytology.
It could be interpreted as coverage of 100% at the primary healthcare.
Impact and Uptake for Colposcopy at the Primary Healthcare
Based on the standardized algorithm of cervical cancer prevention adopted by most countries, only women with abnormal Pap smear results are referred for colposcopy, usually performed in the secondary or tertiary healthcare centers by a specialist gynecology oncologist; colposcopy services are not provided at primary healthcare centers. The prolonged waiting time for a colposcopy appointment, the time women required to travel for attending that appointment, and the overload of secondary- or tertiary-level healthcare centers offering colposcopy services, among other important limitations, make this scheme less efficient for cervical cancer prevention. In this sense, Maimela et al 20 assessed whether decentralization colposcopy services to primary healthcare centers increases the access to colposcopy. Before the study, gynecological oncologists trained district physicians to provide colposcopy services at the primary healthcare centers. They defined abnormal Pap smear results as the detection of high-grade squamous intraepithelial lesions (HSILs), atypical squamous cells, or HSIL squamous cell carcinomas. Women with abnormal results were scheduled for a colposcopy at the same primary healthcare center. They compare outcomes pre- and post-decentralization of colposcopy in women aged >18 years. The number of women who underwent Pap smear at the primary healthcare center and then colposcopy increased threefold post-decentralization. Further, the waiting time to access for colposcopy decreased to 21.7% in women who presented to the rural center. Likewise, Blanckenberg et al 21 found an improvement in colposcopy uptake by 18% from 1 year before to 1 year after the establishment of colposcopy service in a rural health center with a positive trend. Furthermore, a significant reduction with waiting time of 29 days was observed. This study confirmed that the establishment of a colposcopy service in a rural hospital could help improve access for many rural women requiring this service. Furthermore, Ogilvie et al 23 implemented a colposcopy service at the primary-level healthcare center and compared the rate of attendance for a colposcopy with the third level healthcare center. At post-decentralization of colposcopy to the primary care, the default rate fell from 17.2 to 1.3%, with a 15% difference in the default rate compared with the previous period.
Factors Associated With Attendance or Non-Attendance to a Colposcopy Appointment
Buss et al 7 estimated the proportion of women accessing colposcopy after an abnormal Pap smear result. In this study, 700 (39.8%) of 1761 abnormal cytology reports were associated with a subsequent colposcopy. Women residing in metropolitan areas were more likely to have a colposcopy record than those living outside of the capital area (524/700 vs 176/700). Cytology with atypical cells excluding a high-grade lesion was over represented among women with colposcopy (503/700 vs 187/700 for HISL and 10/700 for invasive cancer). A previous study of the same author 18 aimed to quantify the non-attendance rate to colposcopy among hr-HPV-positive women and to identify factors influencing this behavior. In this study, 1235 (80.4%) of 1537 women with HPV-positive tests underwent colposcopy. Multivariable analysis revealed that cytology result (HSIL) (odds ratio [OR], 2.16; 95% confidence interval [CI], 1.16-4.43), provision of in-house colposcopy (OR, 5.14; 95% CI, 3.81-7.01), and age 35 to 44 (OR, 1.40; 95% CI, 1.01-1.96), 45 to 54 (OR, 2.06; 95% CI, 1.32-3.32), and >55 years (OR, 2.32; 95% CI, 1.40-4.03) compared with 25 to 35 years were associated with colposcopy accessibility. Jones et al 22 evaluated the factors associated with non-attendance for colposcopy to guide health service planning and reported 24.7% (74/299) non-attendance to colposcopy, and the multivariable logistic regression analysis only evidenced significant differences between clinics C and A (OR, 5.06; 95% CI, 2.45-10.65).
Risk of Bias
Of the 5 cohort studies, 3 and 2 had a moderate and low risk of bias, respectively. Based on the eligibility domain, only 1 study did not report whether the outcome of interest did not occur at baseline, 7 whereas based on the comparability domain, only 2 studies were adjusted for confounding factors using regression models.18,22 In the outcome domain, only Buss et al 7 reported no significant losses during the follow up period (Table S2).
Maimela et al 20 presented a high risk of bias because the participants evaluated during the preintervention period were not the same as in the postintervention period (Table S3).
Mittal et al 19 reported that adherence to colposcopy in HPV-positive women and to the treatment of premalignant lesions was 78 and 80%, respectively. Conversely, adherence to the 1-year follow up was low (23.2%) due to telephone numbers or residence changes, poor understanding of the disease, and lack of support from spouse or family. In the moderator domain, the steps to follow are provided in detail to carry out the intervention. They also reported the intervention facilitation strategies, such as the training provided to study personnel, monitoring strategies, or the support of critical actors and stakeholders in the region. Regarding the delivery quality or participant responsiveness, they did not report any indicators that allow assessing the quality of the services offered, the user satisfaction, or the causes that hinder the ability to respond to the intervention.
Discussion
Our main results show that studies on this topic are cohorts and cover only a few countries. The primary screening method used is Pap smear, and women with abnormal Pap smear results were referred for colposcopy by a specialist. Although colposcopy services are not common in primary care, when they are established, they improve the efficiency of care.
Cervical cancer is highly preventable and can be easily treated if detected at an early stage. 24 However, its incidence and mortality in LMIC are disproportionate to that of high-income countries due to the lack of detection and prevention programs, or, when they exist, due to barriers in their adoption and implementation.24 -26 Thus, various LMCI show inequalities in the coverage of cervical cancer screening programs where the general detection rates continue to be suboptimal.24,27,28 Despite these, only a few studies on LMIC have been published on this subject.
Compared with no screening, all modeled cervical cancer screening strategies substantially improve cases, deaths, and life years. 29 Hence, to ensure broader access to eligible women and to minimize vertical investment, screening and treatment services have been widely integrated into primary healthcare. 29 Thus, various studies have shown successful initiatives to incorporate primary care centers in China, Zambia, Benin, the Ivory Coast, and Senegal; some of them were sponsored by the International Agency for Research on Cancer/World Health Organization.30,31 For example, in China, due to the uneven development of the social economy, early detection strategies are different in various regions. In Beijing, free cervical cancer screening pilot programs began in 2008 with cytology screening at primary healthcare facilities, with the increasing cervical cancer screening rate year by year. 30 In Benin, the Ivory Coast, and Senegal, timely screening as part of the routine service in primary healthcare screened as many women and treat a significant proportion of women with positive results with thermal ablation, having only minimal side effects. 31
Although Pap smear is the main screening examination, various experiences show successful results with other alternatives. In China, a study found that the primary cervical smear test was suitable and inexpensive as a cervical cancer screening method for women older than 35 years in primary care settings. 32 Colposcopes are expensive and not always available in primary care centers; therefore, women are referred to centers providing this service. Consequently, colposcopy is often inaccessible to many women in LMIC who are highly at risk of developing cervical cancer. 33 As an alternative to limitations in accessing a colposcope, in Perú, studies reported promising results in a telecolposcopy platform using a pocket colposcope for primary care settings to improve sensitivity and access colposcopy tests. 33 In this sense, this study suggests the possibility of bringing colposcopy to a primary care setting and eliminating a step in the referral process including the necessary evaluation by a specialist, which is important in systems where these are scarce. 33 Another similar experience occurred in Madagascar where the use of smartphones to perform digital visual inspection of the cervix was evaluated after applying 5% acetic acid inside and outside the point of care. 34 They found that, with this method, the sensitivity and specificity of the on-call assessment was similar to that of the external medical consensus. 34 Although this study was not conducted in primary care centers, they show the potential of telemedicine in medical facilities far from tertiary care centers. These 2 experiences revealed that alternative solutions to the long waiting time for a colposcopy appointment or trips to the second or third level health centers that offer these services.
These alternatives would also improve the limited access to screening methods in rural primary care facilities. The socioeconomic status is an important determinant in whether a woman is screened, diagnosed, and receives treatment in the eventual case of cervical cancer. 35 As a result, rural areas with poorer and lesser educated populations have higher rates of cervical cancer incidence and mortality than urban areas.36 -38 Therefore, the search for viable alternatives to improve access to diagnostic means should be a priority, including specific training to improve disease knowledge and screening rates. In India, a total of 8 volunteers and 17 health workers motivated women for 93 screening and health education sessions in 46 of 82 villages included, achieving a performance of 3.4/1000 for the detection of pre-cancer and cervical cancer. 39
Despite the fact that care efficiency in screening and care improves with the incorporation of primary care centers, this does not exclude the need for adequate training in physicians to avoid unnecessary referrals. A systematic review showed that prior pelvic evaluation rates occurred in only half of patients referred to higher complexity centers and in less than half of patients with suspicious symptoms. 40 Likewise, 39% of “clinically suspicious” cervixes referred for colposcopy were free of abnormalities on subsequent evaluation. 40 Furthermore, adequately trained personnel are important not only for a good diagnosis but also for adequate follow up if an impact on aspects such as cancer mortality is assessed. For example, although the increase in Pap coverage was not related to a decrease in the mortality rate in Colombia, a reduction in mortality was only found in departments with a higher proportion of women who sought medical advice when informed of the abnormal findings on the PAP smear. 28 These results suggest that for the strategy to be successful, not only deciding the necessity to include primary care establishments but also adequate training, an adequate follow up, and treatment structure are important.
In addition to the small number of studies, the heterogeneity of the studies included should be emphasized in this scoping review. In addition to different countries where the studies were conducted and different study designs, objectives, populations included, and even screening methods was performed stand out. Although these differences do not allow us to measure the results of our study because we are not answering a specific research question, they allow us to point out that the aspects studied regarding the use of colposcopy at the first level of care do not cover all issues that health professionals might need to make decisions in public health.
One of the aspects that merit research is the strategies that can be implemented to make up for the shortage of health professionals and the difficulties that primary care health centers have in meeting the population’s demands for care.41 -43 This is relevant if colposcopy should be included as a public health strategy at this level of care. Thus, it could mean an additional burden on physicians in these facilities at the expense of time for other activities and a greater likelihood of mental health problems that would further limit care. 44
Our study has some limitations. First, although we conducted a comprehensive and rigorous search strategy to identify relevant articles that met the study criteria, some studies may not be identified. Second, the study results may have been influenced by the search terms that were used, the number of databases consulted, and the selection of databases used in the search. As a result, the findings of this review may be influenced by publication bias. Another important limitation is the heterogeneity between the studies found, which may limit the comparability and generalizability of results. Another limitation is the lack of studies reporting outcomes in patient preferences and in factors associated with satisfaction or acceptance of colposcopy at the primary care level. These knowledge gaps should be addressed in future studies that allow for a broader vision of the implementation of colposcopy in primary care.
Conclusion
This scoping review provides a current map of studies that have evaluated the use of colposcopy in primary care. Our results show that few countries have investigated the subject; however, although the results are promising in some experiences, barriers should be identified to its implementation and the care structure for this implementation to be successful in reducing cervical cancer incidence and mortality.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231198942 – Supplemental material for Colposcopy in the Primary Health Care: A Scoping Review
Supplemental material, sj-docx-1-jpc-10.1177_21501319231198942 for Colposcopy in the Primary Health Care: A Scoping Review by Vicente A. Benites-Zapata, Enrique A. Hernandez-Bustamante, Luis M. Acuña-Chávez, Claudia P. Escudero-Gaytan, Juan R. Ulloque‑Badaracco, Esteban A. Alarcón-Braga, Gino Venegas and Percy Herrera-Añazco in Journal of Primary Care & Community Health
Footnotes
Author Contributions
Idea for the article: Vicente A. Benites-Zapata and Gino Venegas. Literature search: Luis M. Acuna-Chavez, Claudia P. Escudero-Gaytan, Juan R. Ulloque‑Badaracco, Esteban A. Alarcon-Braga. Data analysis: Vicente A. Benites-Zapata Luis M. Acuna-Chavez, Claudia P. Escudero-Gaytan, Juan R. Ulloque‑Badaracco, Esteban A. Alarcon-Braga. Drafted: Percy Herrera Añazco. Critically revised the work: Percy Herrera Añazco.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.