
Abstract
An elderly man with COPD and heart failure was admitted to the Family Medicine Inpatient Service from the Emergency Department (ED) after experiencing acute onset of shortness of breath at home. He had recently been briefly hospitalized with COVID pneumonia. Upon arrival in the ED, he was requiring continuous positive airway pressure to maintain oxygen saturations. Overall, physical exam was notable for mild respiratory distress. Lab evaluation was unremarkable, but chest x-ray showed a right sided pneumothorax. Spontaneous pneumothoraces have been described in post-COVID cases, with COPD and mechanical ventilation thought to be risk factors. Treatment consists of supportive cares, needle decompression and thoracostomy if necessary. Providers should be aware of this rare albeit serious complication and monitor higher risk patients appropriately.
Case Presentation
A 70-year-old male was brought into the emergency department (ED) by emergency medical services (EMS) after awakening with sudden shortness of breath and pleuritic chest pain. He had been discharged from our hospital 9 days prior for Coronavirus disease 2019 (COVID-19) pneumonia. During that 2-day hospitalization, he was treated with remdesivir, dexamethasone, and supplemental oxygen while on the general medical wards. The patient has a past medical history significant for emphysema dominant severe chronic obstructive pulmonary disease (COPD) Gold Stage IV, heart failure with reduced ejection fraction with his last echo showing 43% EF, prior pulmonary aspergillosis status post right upper-lobe wedge resection and lower lobe bullectomy in 2016, on Eliquis due to paroxysmal atrial fibrillation and prior venous thrombosis, and a 30-pack year smoking history.
When EMS arrived at the patient’s home, his initial oxygen saturations were in the 70s. He was placed on 10 L nasal cannula and transitioned to continuous positive airway pressure (CPAP) by EMS. At ED presentation, he was saturating 97% on CPAP with a pressure of 7 and FiO2 of 60%. He was then transitioned to the ED CPAP, with a FiO2 of 30%, and remained stable. On physical exam, the patient was in mild respiratory distress, tachypneic, and breath sounds were decreased on the left. The patient’s initial blood workup included complete blood count, chemistry panel, troponins, lactate, and arterial blood gas. Blood work showed an unremarkable complete blood count and normal chemistry panel. Lactate was not elevated. Troponins were unchanging. The arterial blood gas showed hypercarbia, but normal pH. Electrocardiogram did not show ST changes concerning for a myocardial infarction. A portable chest x-ray (CXR) showed a large left spontaneous pneumothorax without features of tension (Figure 1). A pigtail catheter was placed with 20 cm H2O suction, and his oxygen saturation increased to 91% on room air. CXR after pigtail catheter placement showed satisfactory re-expansion with a small residual apical pneumothorax (Figure 2). Thoracic ultrasound of the chest showed good lung slide anteriorly and laterally.
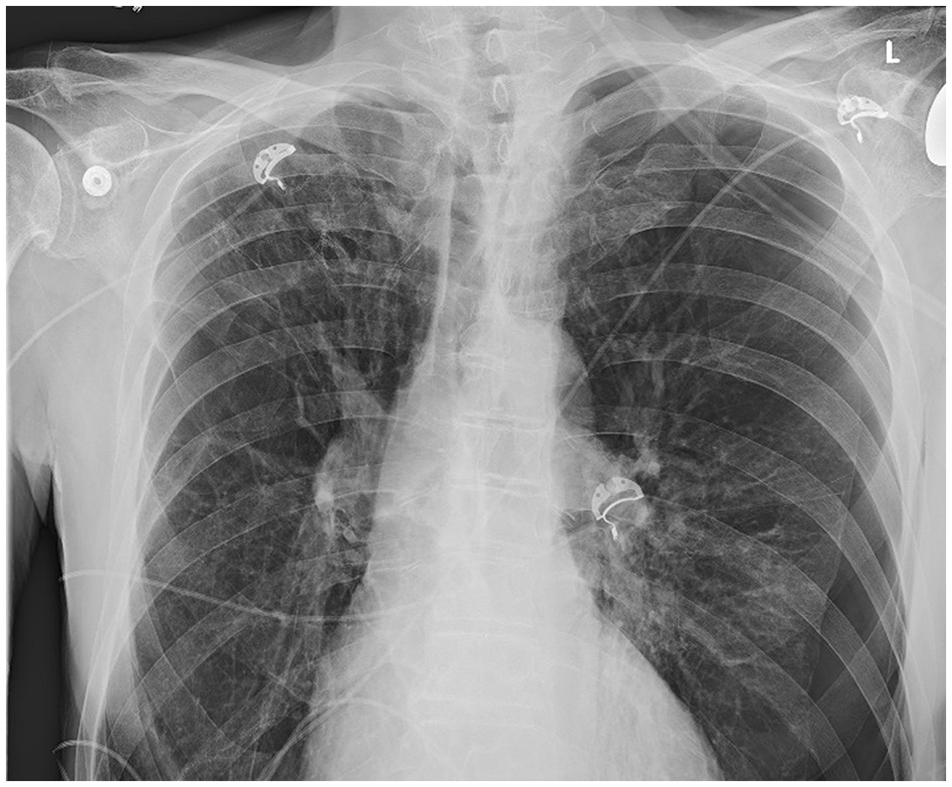
New moderate to large left pneumothorax.
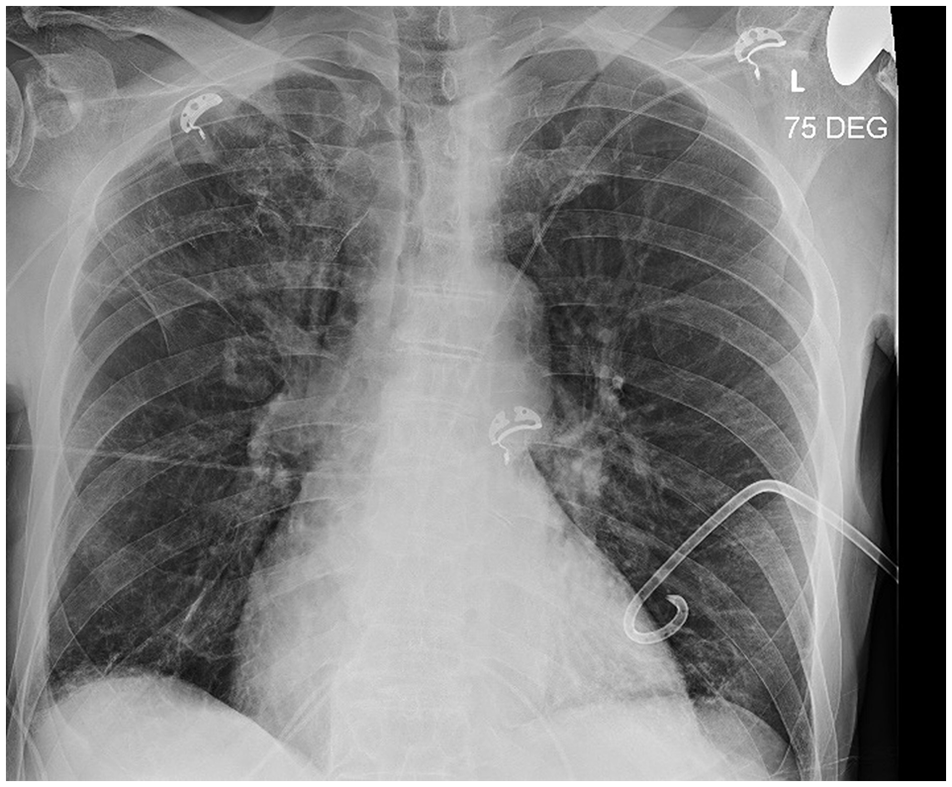
Left pigtail pleural catheter placed.
The patient was then transferred to the Family Medicine Inpatient Service in stable condition. Chest tube was in place with continued air and clear fluid draining. Oxygen saturations were maintained between 88 and 92% due to his history of COPD. Thoracic surgery was consulted as this was the patient’s first pneumothorax. They did not recommend surgical or chemical pleurodesis. Interventional pulmonology (IP) changed suction to −10 cm water wall suction and reassessment of pneumothorax showed interval improvement on CXR. A clamping trial and subsequent CXR showed resolution of the pneumothorax and the chest tube was subsequently removed. IP did not recommend a blood patch of pleurodesis for follow up.
After 5 days in the hospital, the patient remained afebrile and was saturating well on room air. A daytime oxygen study was performed prior to discharge that showed 1.5 L oxygen was needed with activity. He was discharged in stable condition to his home with close follow up with his primary care physician. He remained asymptomatic and radiology follow up 2 days later showed no significant changes from his last x-ray during his hospitalization. Due to his severe dyspnea at baseline, the patient met with palliative care 3 months later, where he was started on low dose morphine.
Discussion
This was an uncommon case of a spontaneous pneumothorax (SP) in the setting of COVID-19 and underlying lung disease (COPD). COVID SPs are rare, with limited reported cases in the literature. Likewise, risk factors have not been clearly established but are postulated to include mechanical or non-invasive ventilation, ICU admission, emphysema, and tocilizumab therapy.1 -3 The mechanism of SP formation with COVID has been thought to be due to inflammation and increased respiratory effort. 4 Our patient had 1 of these risk factors (emphysema due to COPD) but did not undergo non-invasive or mechanical ventilation nor received biologic therapy.
Incidence of SP’s in COVID-19 appears to be unusual with estimates 0.3 to 1% in hospitalized patients, though rates appear to be substantially increased (12-23%) in mechanical ventilation.4,5 Previous studies show that pre-existing lung disease is not seen in most COVID-19 SP cases. However, current data and literature are limited, and more research is needed, including the mechanism behind SP’s in COVID patients, as it appears to be multifactorial.
General clinical presentation of COVID SP’s includes a rapid clinical decline and increase in shortness of breath (SOB), 6 in line with this case. Despite limited research, COVID-19 SP’s have been shown to have a higher incidence than non-COVID SP’s, with chest pain being a far more common presenting symptom and right-sided SP’s are more common. 5 Interestingly, this case was left-sided, although the patient did present with SOB and pleuritic chest pain. Critically ill COVID patients tend to be more commonly affected by SP’s, 7 however, this patient was stable for floor management. COVID SP onset seems to occur around 9 to 20 days after initial admission, in line with this case. 4 In-hospital mortality of COVID-19 is increased fourfold by SPs, and survival rate is approximately 66%, with the age >70 being a predictor of mortality.8,9 Despite his comorbidities and age, our patient did well with prompt management and required only a chest tube, NC oxygen (no ventilation needed), and no transfer to the ICU required.
Non-COVID SP’s are also seen in patients with underlying lung disease, however other risk factors for non-COVID SP’s such as age and smoking haven’t yet been associated with COVID SP’s. 10 Management of non-COVID SP’s is also similar: supportive cares, needle decompression and thoracostomy if necessary. The recurrence of non-COVID SP’s remains high (up to 30% for primary and 43% for secondary) but the recurrence of COVID SP’s haven’t yet been established. 10
Conclusion
Prior lung damage and inflammation may predispose COVID-19 patients to pneumothorax development. Pneumothoraces are rare, but “can’t-miss” diagnosis in COVID-19 patients, resulting in increased mortality, especially for elderly patients. Providers should consider this life-threatening complication as part of the differential of new-onset chest pain or dyspnea in the week following COVID-19 disease, especially those patients with risk factors. Ultimately, our case underlines the importance of counseling and monitoring patients with underlying lung disease and COVID for clinical deterioration, as this could represent the onset of a SP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.