
Abstract
Objective:
This study evaluates the efficacy of Internet-Based Training in Trauma Care for Nurses (IBTTCN) to improve nurses’ trauma intervention self-efficacy, professional quality of life, and attitudes and knowledge about post-traumatic stress disorder.
Methods:
Forty-one nurses participated from May to July 2021. The assessment points were at baseline (T1), immediately after program completion (4 weeks; T2), and 1 month after T2 (T3). Data were analyzed using repeated-measures analysis and generalized estimating equations.
Results:
In the intervention group, trauma intervention self-efficacy increased significantly after the IBTTCN, and the effect of such self-efficacy over time was significant.
Conclusions:
The IBTTCN improved nurses’ trauma intervention self-efficacy.
Introduction
Frequent exposure to adverse events in daily life can lead to post-traumatic stress disorder (PTSD). 1 PTSD is highly associated with severe psychiatric problems, including anxiety disorders, sleep disorders, depression, suicide ideation, and suicide. 2 Further, PTSD can be 1 of the various mental health consequences of the recent COVID-19 pandemic and its associated daily life stressors among the general population. 3 Researchers have demonstrated that as awareness of the prevalence and long-term effects of trauma increase, mental health experts must be more sensitive to the impact of trauma on those involved in traumatic experiences. 4
Despite the importance of PTSD, a disparity exists between the need for services of professionals with experience in PTSD and their availability. Courtois and Gold suggested that the inattention to the traumatic stress field in the curriculum of most health professions has contributed to service resource inadequacy 5 ; they also emphasize the need to build a network of experts and train personnel to assist people in overcoming, as quickly as possible, their traumas stemming from daily life happenings. 5
Further, although PTSD has become a familiar term among the general public, many health professionals do not have adequate knowledge or skills to treat PTSD and related disorders.6 -8 Some professionals are even reluctant to provide services for treating PTSD because of own lack of self-confidence.5,6 Nurses in the United States of America reported insufficient knowledge, attitudes, and low self-efficacy regarding PTSD. 7 Hoysted et al 9 showed that a lack of trauma knowledge and confidence in intervention skills are barriers to nurses caring for clients with PTSD. Moreover, nurses who encounter clients who have experienced trauma undergo long-term and repeated exposure to compassion and empathy for the psychological pain of their clients, leading these nurses to potentially experience burnout, secondary trauma in own lives, or even a decrease in compassion satisfaction.10,11
Particularly in Korea, psychological trauma centers operate as subdivisions of mental health welfare centers for local communities. 12 Accordingly, nurses working at these centers are the forefront providers of advice/therapeutic interventions for clients with psychological trauma. Although these professionals play a pivotal role in trauma treatment, Dong and Seo 13 demonstrated that they have less opportunities for systematic training in trauma care compared with other professions. This highlights the relevance of emphasizing the development of well-structured training programs for nurses working in these centers to enhance their competency in trauma care.
Still, there are several barriers to delivering training to health professionals, 9 including time constraints, confusing evidence on what to do, and lack of flexible access to education. 14 Regarding treatments for trauma, some of the widely applied methods are cognitive behavioral therapy, exposure therapy, and eye movement desensitization and reprocessing (also known as EMDR) training 15 ; nevertheless, they are not applicable for all clients, and obstacles exist in their application in the nursing context because of nurses’ education. To address these challenges and create a widely accessible training program, we developed an Internet-based trauma recovery training program that is cost- and resource-efficient and has minimal time restrictions for nurse trainees.
Despite these advantages, online education does have its limitations, including limited social interaction and hardships in planning/adjusting studying schedules. 16 To try and overcome these disadvantages of online education (as a one-way training method), we added a real-time online workshop training session to the program. In it, students could deliver feedback about the program, ask related questions, and provide suggestions for improving it. We also set a certain relevant period for the training sessions to allow participants to freely partake in the training at a suitable time.
The program was named Internet-Based Training in Trauma Care for Nurses (IBTTCN). It was based on Swanson’s caring theory, 14 and delivers evidence-based information on how to provide interventions that assist clients with PTSD in overcoming trauma. Swanson’s caring theory has been used as a framework in various nursing practice fields to increase nursing practice quality and client satisfaction, 17 and posits that “client well-being” can be achieved through 5 steps: “maintaining belief,” “knowing,” “being with,” “doing for,” and “enabling.” 18 The “maintaining belief” step emphasizes the trust between the client and the nurse. The “knowing” step aims to develop the client’s understanding of the meaning of previous life events; from this perspective, rather than emphasizing or avoiding traumatic experiences, the nurse and client try to create knowledge/understanding around the human responses to recovery. In the “being with” step, the nurse reports on the necessity behind recognizing the client’s feelings by providing them with the needed space for sharing their feelings/experiences. The “doing for” stage is characterized by the nurse delivering care for the client. In this study, the “doing for” step emphasized the client’s self-help process by recognizing their traumatic experiences, maintaining rational thinking during stressful situations, and controlling negative emotions. In the “enabling” stage, nurses help clients to change their daily routine and solve problems on their own as they encounter new events. The program used in this research was structured to allow for nurses to deliver care according to each of these steps. For example, nurses were trained to use “response letters” to help develop strong and deep trust with clients, corresponding to the “maintaining belief” step.
To the best of our knowledge, no study thus far has examined the efficacy of an Internet-based training program for improving nurses’ trauma care intervention competency. Thus, this study aimed to (1) develop the IBTTCN, which targets nurses’ trauma care intervention competency, and (2) evaluate its impact on trauma intervention self-efficacy, professional quality of life (pro-QOL), attitude, and knowledge about PTSD.
Methods
Study Design and Ethics
This cluster randomized controlled trial (RCT) was conducted between May and July 2021, employed cluster randomized sampling, and compared the IBTTCN group with a 1-month waitlist control group. All surveys and interventions were provided via online links. The online training program allowed self-learning by enabling participants to individually access the online links. The same workbook and online training program were provided to the control group, but only after the intervention group responded to the 1-month follow-up test.
This trial was registered at the ClinicalTrials.gov US National Library of Medicine (registration number: NCT05446974) and is available online. The CONSORT checklist was used as the reporting guideline. 19 Ethical approval was obtained from the Yonsei University Human Research Ethics Committee of the institution to which the authors were affiliated (4–2021-0324). All procedures in this study were performed in accordance with the Declaration of Helsinki.
Recruitment Procedures and Participants
The required sample size was calculated using G*Power, version 3.1.3. Considering a repeated-measures analysis with a power of 90%, a median effect size of 0.25, a significance level of 0.05, 2 groups, and 3 measurements, the total number of samples required was 36, with 18 each for the intervention and control groups.
Regarding recruitment, to avoid contamination by word of the intervention spreading, samples were extracted through cluster randomized sampling from each participating institution. We sent an official letter to 108 community mental health and welfare centers in 8 metropolitan cities in Korea to recruit participants, and nurses could communicate their intention to participate by accessing an online link. The recruitment period was 4 weeks.
The inclusion criteria were as follows: having a nursing license; currently working at a mental health welfare center; being able to access the program through a computer/mobile gadget; understanding the purpose and voluntarily agreeing to participate in the research. The exclusion criterion was not agreeing to participate in the study.
Training Program
Workbook
The workbook was developed by reorganizing the Internet-based trauma recovery nursing intervention developed by Kim et al. 14 Through it, participating nurses could learn how interventions may easily and efficiently be provided to their clients (Table 1). The workbook comprises a nursing intervention method for trauma victims and guidelines for dealing with such clients. These guidelines for nurses were devised according to expert-based knowledge on trauma derived through a review of the latest literature on treatments and preventive interventions for trauma. The workbook emphasizes the points to focus on during an intervention and describes an interactive feedback method involving the client.
Topics and Contents of the Workbook.

Online education
The self-learning online training program was developed according to the workbook (Table 2). It comprises 8 sessions of approximately 20 min each, totaling around 3 h. The program included visual prompts in Power Point format, voice-recorded training sessions by researchers, and emphasized what nurses should focus on in the workbook. As aforementioned, the program was presented in an online format to make it simple, widely accessible, and cost-effective, and the training was provided using an online platform to check participants’ access and learning progress.
Baseline Characteristics of Participants (N = 41).

Note. Cont., control group; Int., intervention group; M, mean; PMHRN, psychiatric mental health registered nurse; pro-QOL, professional quality of life; PTSD, post-traumatic stress disorder; SD, standard deviation.
Fisher’s exact test result.
Mann-Whitney test.
Real-time online workshop
After completing all the online self-training sessions (Supplemental Appendix 1), the nurses participated in a real-time online workshop. As described, this workshop was conducted to overcome 1 of the limitations of online self-learning. Participants could choose the most convenient option from 2 workshop times that were made available. To allow for the feedback of all participants to be heard at the workshop, participants from the intervention group were divided into subgroups of 10 people each, and those from the control group into subgroups of 10 to 11 people each. All researchers who developed the program were present during the feedback sessions of the 2 workshops, which lasted approximately 2 h each. Participants shared questions and their impressions regarding the training content, and the researchers provided relevant answers. Participants also provided feedback and suggestions for program improvement.
Measures
General characteristics
The sociodemographic characteristics included in the questionnaire were age, sex, religion, marital status, education level, psychiatric mental health registered nurse license, career experience, and education related to trauma.
Trauma intervention self-efficacy
To measure trauma intervention self-efficacy, we used questions developed by Palfrey et al 4 to measure confidence in trauma intervention. After obtaining approval from the original tool developer via e-mail, the original questionnaire was translated into Korean by the research team. Two non-expert, Korean nurses located in the United States of America and fluent in both English and Korean translated it back into English and confirmed that the meanings in the English and Korean versions were the same.
Five items were used to evaluate self-perception of trauma-related work performance, work confidence, response to trauma, knowledge and skill level, and the relevance of training and awareness of trauma services. They were responded on a 10-point scale (1 = not at all; 10 = very high); the higher the score, the higher the self-efficacy of trauma intervention, 4 and total scores were calculated using the average score for all items. This instrument was applied at all time points, and its Cronbach’s ⍺ in this study was .96.
Professional quality of life
To measure pro-QOL, we used the 30-item Korean version of the Pro Quality of Life 5 (K-ProQOL 5) tool, which was developed for mental health professionals by Stamm, 20 and translated by Joo et al. 11 The sub-domains are compassion satisfaction, burnout, and secondary trauma stress, each with 10 items. Items are responded on a five-point scale (1 = not at all; 5 = very often); a higher score indicates a higher level of pro-QOL on each domain. 11 This instrument was applied at all 3 time points, and the Cronbach’s α was .92 for compassion satisfaction, .81 for burnout, and .83 for secondary trauma stress.
Attitudes and knowledge about PTSD
We used the 8-item Korean version of the Attitude and Knowledge Measurement Tool for PTSD, which was developed by Tsai et al, 21 and translated by Bang et al, 1 to measure attitudes and knowledge about PTSD. For attitudes, the tool has 2 subscales: attitude toward government policy (5 items) and attitude toward clients with PTSD (3 items). Items are responded to on a 4-point scale (1 = strongly agree; 4 = strongly disagree); lower scores indicate a higher degree of agreement with the question. 1
It also comprises 8 items on knowledge about PTSD that were responded to on a 4-point scale (1 = very much; 4 = not at all), with points 1 and 2 being treated as correct answers and points 3 and 4 being treated as incorrect answers. For each question, a correct and an incorrect answer was awarded 1 and 0 points, respectively, allowing for overall knowledge scores to be obtained (total range, 0-8 points), with higher scores indicating a higher level of knowledge. This instrument was applied at all time points. The Cronbach’s ⍺ was .79 for attitude toward government policy, .83 for attitude toward clients with PTSD, and .61 for knowledge about PTSD.
Procedures
Consent, enrollment, and randomization
After sending the official letter to 108 community mental health centers, participants who wished to participate in the study were provided with detailed information about the study on a website linked by QR code. After confirming their eligibility, participants were requested to provide written informed consent. To prevent word of the experiment from spreading, the centers to which the participating candidates belonged were randomly assigned to the intervention and control groups using the “random sequence generator” of Research Randomizer (https://www.randomizer.org/). The participants were blinded to group allocation throughout the study.
Pre-test
Participants were randomly assigned to the intervention or control groups, and then provided with a link for the baseline test via e-mail.
Training
We sent the workbook to the intervention group via post immediately after pre-test completion and provided them with links to the self-learning program platform via e-mail and text messages. The duration of the online self-learning program was 3 weeks. To induce participants’ learning and ensure sufficient understanding, the program was divided into 8 sessions, with 2 or 3 sessions being provided per week; this frequency of 2 or 3 sessions per week was meant to prevent participants from listening to all the sessions at once and provide them with sufficient time for self-study.
Through a function of the online platform (ie, Naver Band), we could check whether each participant was learning individually. Specifically, when we uploaded each session, we could check which participants had opened the file, and after learning, participants were asked to leave a “name-learned” comment. We could also confirm learning through access to a copy of the screenshot of the participant’s screen when using the platform. To minimize dropouts, text messages were sent twice a week to notify session start and encourage participants to engage in the learning activity.
All participants in the intervention group completed the 8-session training and partook in the real-time online workshop (4th week of training) to share their training experiences.
Post-test
After the 4th week of training, a post-test was applied to both the intervention and control groups. Once more, we provided a link for the online platform survey, and the questionnaire was the same as that used in the pre-test.
One-month follow-up
In both groups, at 4 weeks after the post-test, the follow-up survey was conducted. All participants completed the follow-up survey. To show our appreciation for their participation, we rewarded participants in both groups with 100 000 Won (around US$ 100) upon follow-up test completion.
Data Analysis
The collected data were analyzed using SPSS for Windows (IBM), version 27.0. Participants’ general characteristics were presented using descriptive statistics, specifically frequency, percentage, mean, and standard deviation. A homogeneity test was performed, and participants’ general characteristics were assessed using chi-squared test, Fisher’s exact test, t-test, and Mann-Whitney U-test. The variables were tested for normality using Kolmogorov-Smirnov and Shapiro-Wilk tests.
Group differences for the variables of interest at pre- and post-test were analyzed using the Mann-Whitney U-test and t-test, depending on the normality test. A repeated-measures analysis of variance was used to examine group differences over time. In addition, generalized estimating equations were used to test for variables that were not normally distributed.
Results
Participants’ Flow
In total, 42 participants from 24 centers were recruited. Immediately before the intervention, 1 participant withdrew from the study (Figure 1), so only 41 participants completed the study, with 20 being assigned to the intervention and 21 to the control group.

CONSORT flow diagram of this study.
Participants’ Baseline Characteristics
No statistically significant differences were observed between the intervention and control groups at baseline (Table 2). Of the participating nurses, 31 (75.6%) had a psychiatric mental health registered nurse license; 19 (46.3%) participants had between 3 and less than 10 years of experience; 39 (95.1%) had cared for a client with PTSD in the past, while 29 (70.7%) participants had received trauma-related education. The groups showed no significant differences in baseline trauma intervention self-efficacy, general self-efficacy, pro-QOL, and attitudes or knowledge about PTSD.
Effect of the Intervention
Trauma intervention self-efficacy
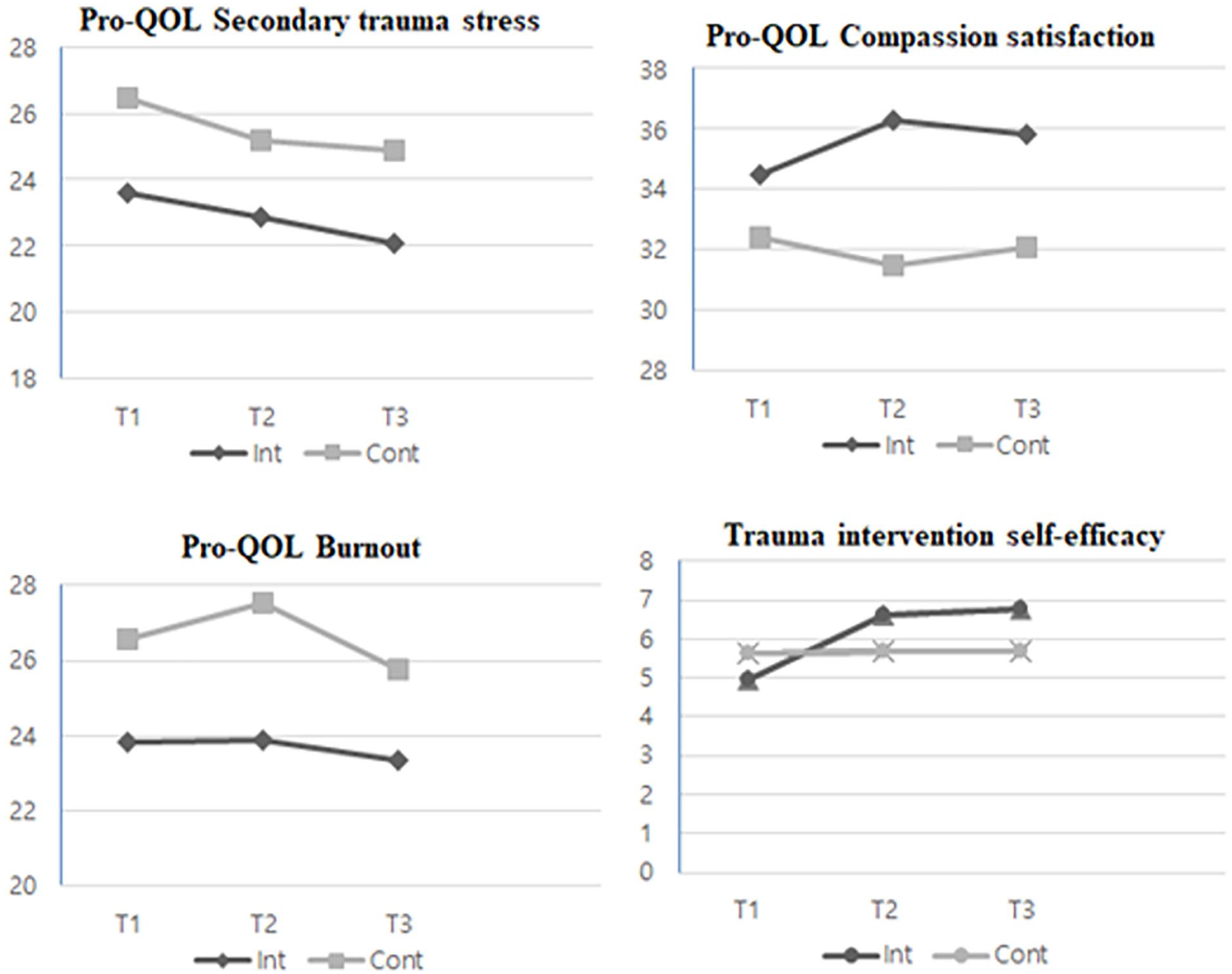
The means and standard errors (SE) of the scores for all variables at each time point are presented in Table 3. Figure 2 shows the estimated mean scores across all time points by group.
Effects of the Intervention on Trauma Intervention Self-efficacy, Professional Quality of Life, and Attitudes and Knowledge About PTSD.

Abbreviations: Cont., control group; Int., intervention group; PTSD, post-traumatic stress disorder; measurements were performed before the program (T1), at the end of the program (T2), and one month after program completion (T3); intervention group (n = 20); control group (n = 21).
Estimated mean ± standard error.
Wilks’ lambda multivariate test.
Generalized estimating equations models.
Effects of the intervention at different time points in the intervention and control group.
Trauma intervention self-efficacy had a significant effect on the groups over time (F = 10.095, P < .001). A post-hoc analysis was performed to confirm group differences at each time point. Although the score for self-efficacy was lower for the intervention group at baseline compared with the control group, it improved (T1 = 4.97; T2 = 6.60). However, the difference between the 2 groups at T2 was not statistically significant (t = −1,921, P = .063). While the score for the control group decreased from T2 to T3, that for the intervention group improved (T3 = 6.77), and the difference between the 2 groups was significant at T3 (t = −2.145, P = .040).
Professional quality of life
Compassion satisfaction was not significantly different between the groups over time (F = 2.795, P = .067). We also assessed group differences for compassion satisfaction at each time point using post-hoc analysis. While the score of the intervention group increased from T1 to T2, that of the control group decreased, leading to a significant difference between the 2 groups at T2 (t = −2.579, P = .014). At T3, the intervention group’s score decreased and the control group’s score increased slightly; the difference between the 2 groups remained significant (t = −2.166, P = .036; Table 3; Figure 2).
No statistically significant differences were found between groups over time for either burnout (t = 0.717, P = .491) or secondary trauma stress (t = 0.132, P = .877). Nonetheless, the post-hoc analysis revealed a significant difference between groups in burnout at T2 (t = 2.133, P = .039). While scores for burnout increased at T2 for both groups, the increase in the control group was more significant. Meanwhile, secondary trauma stress differed significantly between groups at T3 (t = 2.040, P = .048), with the scores decreasing at T2 and T3 in both groups compared with those at T1. However, a significant reduction occurred in the control group.
Attitudes and knowledge
The scores for attitudes and knowledge about PTSD were not normally distributed; therefore, the intervention effect over time was confirmed using generalized estimating equations. Attitudes toward government policy did not significantly affect the groups over time (χ2 = 4.266, P = .119). The post-hoc analysis showed that the scores for attitudes toward government policy decreased in the control group and increased in the intervention group from T2 to T3. There was also a significant difference between the 2 groups at T2 (z = −2.235, P = .02) and T3 (z = −2.763, P = .006). There were no statistically significant results regarding attitudes toward clients with PTSD.
The results for knowledge about PTSD did not significantly differ between groups over time (χ2 = 5.915, P = .0052). Our post-hoc analysis revealed that the intervention group scored lower than the control group at T1; the intervention group’s score increased significantly at T3; the score at T3 of the intervention group was significantly higher than that of the control group (z = −1.987, P = .047).
Discussion
This RCT assessed the effects of the IBTTCN on trauma intervention self-efficacy, pro-QOL, attitudes toward PTSD, and knowledge about PTSD among registered nurses at mental health welfare centers. The results show the effectiveness of Internet-based training focused on enhancing confidence through self-directed learning among nurses.
Regarding trauma intervention self-efficacy, the difference between the intervention and control groups over time was significant, suggesting the intervention’s effectiveness. Although the intervention group’s score was lower than that of the control group at baseline, it was higher both immediately after the intervention and at the one-month follow-up. We also observed that the score change for each item on trauma intervention self-efficacy was significant in the intervention group. The training provided various data/resources for nurse trainees, allowing them to directly apply their learnings from the program, which is based on Swanson’s caring theory, 14 to their clients. The intervention group was also presented with specific methods for dealing with clients with PTSD, such as therapeutic communication methods for engaging with clients and strategies for correcting clients’ false cognitive distortions. After the training, the intervention group showed improved confidence in assessing trauma, responding to trauma disclosure, and a greater awareness of related services/resources. Therefore, the program could increase trauma intervention self-efficacy, and participating nurses demonstrated an increase in their self-reported confidence and attitudes toward assessing/treating people with trauma. This is consistent with previous studies showing, after trauma care training, an increase in the overall self-confidence of health professionals, 4 and on their related knowledge, skills, and positive attitudes. 22
Regarding pro-QOL, the difference between groups was not significant at post-test. Although the effect over time was not significant, the post-hoc analysis showed that compassion satisfaction (ie, 1 sub-domain of pro-QOL) increased only in the intervention group at post-test and at follow-up. However, burnout increased more in the intervention group at post-test, and secondary trauma stress decreased more in the control group at follow-up. Compared with baseline, the changes at post-test and at follow-up were inconsistent. These results suggest that the promotion of burnout and secondary trauma stress may be more influenced by other, non-explored factors and occur separately from the promotion of positive factors (eg, job achievement).11,23 Our results also support the weak negative correlation of compassion satisfaction and secondary trauma stress. 20 Therefore, burnout and secondary trauma stress should be distinguished, and intervened on separately, from variables such as compassion satisfaction, which reflects job satisfaction.20,24
Although the training we proposed strengthened job-related competencies and enhanced compassion satisfaction, it did not affect burnout and stress, which mutually influence each other and nurses’ personal and job variables. 23 In the future, stakeholders could endeavor to develop management systems and education that consider each nurse’s professional career and duties. Burnout has organization-related effects, such as on workplace culture and workload, and is predicted to occur when people experience organizational politics and bureaucracy, 25 entailing the need to train personnel in an institutional approach.8,26 Further, to enhance job effectiveness among nurses treating clients with PTSD, it can also be helpful to deliver individualized education from multiple perspectives and tailored to nurses’ individual needs by assessing stressors at the individual level that can be intervened on and that lower burnout or job satisfaction. Some researchers have used therapists’ burnout and compassion scales as competency evaluation methods,20,25 and the results of this study partially support the use of such scales. Nonetheless, the validity of indirect measures, such as pro-QOL, in competency evaluation should be established through further research.
The differences between groups over time in attitudes toward government policy, toward clients with PTSD, and knowledge about PTSD were found to be non-significant after the intervention. The average scores of the intervention and control groups for attitudes toward government policy on PTSD were 3.45 and 3.33 (out of 4), respectively; these figures are similar to the average score of 3.3 in a study conducted with the American public, 21 and higher than the scores of 1.54 to 2.14 in a study with a sample of Korean nursing students. 1 Furthermore, compared with the results of previous studies,1,21 both groups in our sample reportedly held more positive attitudes toward more government funding for research/training/services regarding PTSD at baseline. Specifically, the intervention group may have been satisfied with the participation in the training program we proposed, and there may be the need for continuous support from the government for nurse training and services.
Although both the intervention and control groups showed an increase in their knowledge about PTSD over time, they did not significantly differ. Meanwhile, the intervention group had high scores at follow-up, partially supporting the intervention effect on knowledge about PTSD. The scores of both groups were also higher than the average found in a study conducted among the American public (5.25), 21 and another among Korean nursing students (4.75). 1 Considering that our participants were working as psychiatric nurses at local community mental health welfare centers at the time of the research, we can assume that they already had some general knowledge of PTSD prior to participating in this study. Nonetheless, some professionals (eg, social workers and clinical psychologists) may need more advanced education on PTSD.1,22 Researchers could endeavor to define the different knowledge education interventions that may be suitable for nurses with divergent careers and needs, evaluate questions based on their careers and needs, and extend the training period of the proposed program.
The significance of this study lies in its development and analysis of an online nursing training program. Online training programs can help nurses deal with their generalized lack of time and space constraints for participation, while face to-face counseling has greater accessibility barriers due to most nurses facing difficulties in having a flexible schedule. Online intervention programs also have the advantage of being more cost effective than face-to-face consultations, allowing for 1:1 interactions, and can be developed to include interventions through two-way communication. 16
Limitations
Regarding limitations, first, the training was only provided to nurses working in community settings. Future research could evaluate intervention effectiveness for nurses working in clinical settings and other healthcare professionals.
Second, the training program did not improve the pro-QOL of individual nurses, entailing the need to add content to the training program targeted at reducing burnout and indirect stress in nurses’ work. Finally, our study did not include a long follow-up (eg, 6-month assessment). Researchers could consider the use of long-term follow-ups.
Conclusions
Our results demonstrate that an Internet-based self-learning training improved PTSD intervention competency among nurses. However, there were no significant improvements in their pro-QOL. Researchers could add training content aimed at addressing nurses’ secondary trauma or burnout, and it may be essential to test the effectiveness of the proposed training for other healthcare professionals.
This study emphasizes the need for continuous education and support from the government. Moreover, the COVID-19 pandemic brought with it numerous novel, and often unprecedented, difficulties related to face-to-face interventions. This program may allow for nurses to partake in training through an online platform at any time and place, thus showing consideration of the scheduling limitations that nurses who work in shifts experience.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231181982 – Supplemental material for Evaluation of Internet-Based Training in Trauma Care for Nurses in Mental Health Welfare Centers: A Cluster Randomized Controlled Trial
Supplemental material, sj-docx-1-jpc-10.1177_21501319231181982 for Evaluation of Internet-Based Training in Trauma Care for Nurses in Mental Health Welfare Centers: A Cluster Randomized Controlled Trial by Sunah Kim, Go-Un Kim and Jinyoung Park in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (NRF-2018R1A2B6001504), which was involved in the data collection process and editing of the manuscript.
Ethics Approval
This trial was registered at the ClinicalTrials.gov-U.S. National Library of Medicine (registration number: NCT05446974) and is available online. The CONSORT checklist for RCTs was used as the reporting guideline. Ethical approval was obtained from Yonsei University Human Research Ethics Committee (4–2021-0324). All procedures in this study were performed in accordance with the Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.