
Abstract
Background:
The prevalence of Post Traumatic Stress Disorder (PTSD) has been rising since the start of the COVID-19 pandemic, and affects females, sexual and gender minorities, and individuals with social risks at higher rates.
Objective:
This study examines if the prevalence of PTSD increased from 2019 to 2022 among patients who received care in a national network of safety-net, community-based health centers with integrated behavioral health programs that serve patients at high risk for PTSD.
Methods:
We analyzed electronic health record data from patients with 1 or more behavioral health visits during 2019 to 2022 using repeated cross-sectional data to visualize trends. Change in PTSD prevalence based on the diagnoses associated with each visit from 2019 to 2022 was assessed using a general linear mixed model adjusted for patient-level factors.
Results:
Over 4 years, 182 419 distinct patients received care for PTSD, with prevalence increasing from 2019 to 2022 (OR = 1.09, 95% CI = 1.08, 1.10). Females (OR = 1.81, 95% CI = 1.78, 1.84), LGBTQIA individuals (OR = 1.29, 95% CI = 1.26, 1.33), gender diverse individuals (OR = 1.36, 95% CI = 1.29, 1.42), and patients who reported 1 or more social determinants of health needs (OR = 1.52, 95% CI = 1.46, 1.57) were more likely to have a diagnosis of PTSD.
Conclusions:
In a worrying trend, PTSD prevalence has increased among people receiving integrated behavioral health care at community-based health centers, with disparities observed in subpopulations. Continued effort and investment are needed to meet this increasing need in safety-net settings, particularly for those subpopulations observed to have higher prevalence.
Keywords
Introduction
Post-traumatic stress disorder (PTSD) is a mental health condition triggered by experiencing a stressful, shocking, and dangerous event. 1 Lifetime exposure to trauma is estimated at 80% of the U.S. civilian population and lifetime prevalence of PTSD is estimated at 7.7% to 17.0%.2,3 Due to a complex interplay of biological, social, and economic risks, exposure to trauma, and development of PTSD disproportionately affects females, people who are racial/ethnic minorities, sexual and gender minorities, and have lower incomes.2 -7 Social determinants of health (also called social risks) such as lack of safe housing, lack of transportation access, or food insecurity contribute to both the prevalence of trauma exposure and the development of PTSD within marginalized populations.8,9
In the U.S., COVID-19 exacerbated long-standing health inequities by race, ethnicity, and income. 10 Emerging evidence suggests that the COVID-19 pandemic itself constitutes a traumatic event capable of eliciting traumatic stress reactions and triggering PTSD. 11 Early research indicates that females, sexual minorities, gender diverse individuals, and people with social risks were more likely to experience post-traumatic stress symptoms during the pandemic. 12
Unfortunately, the COVID-19 pandemic was not a singular event with a defined end date that can be attributed to an increase in PTSD. Even after stay-at-home orders were revoked, the repercussions of COVID-19 on housing and food insecurity and job loss persisted. 13 Furthermore, PTSD may emerge months or years after a traumatic event, or it can be triggered by the experience of multiple traumatic events. 14
Community-based health centers (referred to hereafter simply as health centers), which provide safety-net primary and behavioral health care to populations at high risk for PTSD, are an important setting for assessing trends in PTSD prevalence through a health equity lens.15 -17 Health center clinical data from electronic health records (EHRs) can help to elucidate trends in PTSD prevalence over time among populations with health disparities.
This study used EHR data from patients seeking behavioral health care at 200 health centers to evaluate PTSD prevalence over a 4-year period beginning with the year prior to the pandemic. We hypothesized that PTSD prevalence in this population would increase over the study period and would increase during and in the years following the COVID-19 pandemic.
Methods
Setting and Data Source
This retrospective study used data from OCHIN, a national nonprofit health innovation organization that provides a single instance of the Epic EHR system to members which include Federally Qualified Health Centers, Rural Health Centers, and health center lookalikes. 18 Data from the shared EHR (eg, patient demographics, insurance at appointment, patient addresses, prescriptions, diagnoses, laboratory results, and vitals) are collected and standardized, resulting in robust, longitudinal data. The Institutional Review Board of Case Western Reserve University reviewed and approved this study.
Study Sample
Per our study criteria, we first identified all primary care clinics that provided care in 2019 across the OCHIN member network. These methods are described elsewhere. 19 We then identified all patients who had a visit with a behavioral health provider and/or had an associated procedure code indicating an in-person or telehealth behavioral health visit in clinics with integrated behavioral health, between January 1, 2019 and December 31, 2022. A patient with multiple visits across years was considered to be a patient treated for PTSD in each year in which they had a visit. Behavioral health providers were classified based on credentialling information, with National Provider Identifier (NPI) codes. All visits for patients aged 12 to 89 years, between 2019 and 2022, completed by a behavioral health provider, and/or with a behavioral health procedure code were included in the analysis, resulting in a dataset focused on primary care-integrated behavioral health services. See Appendix A for a diagram of the sample selection.
Outcomes
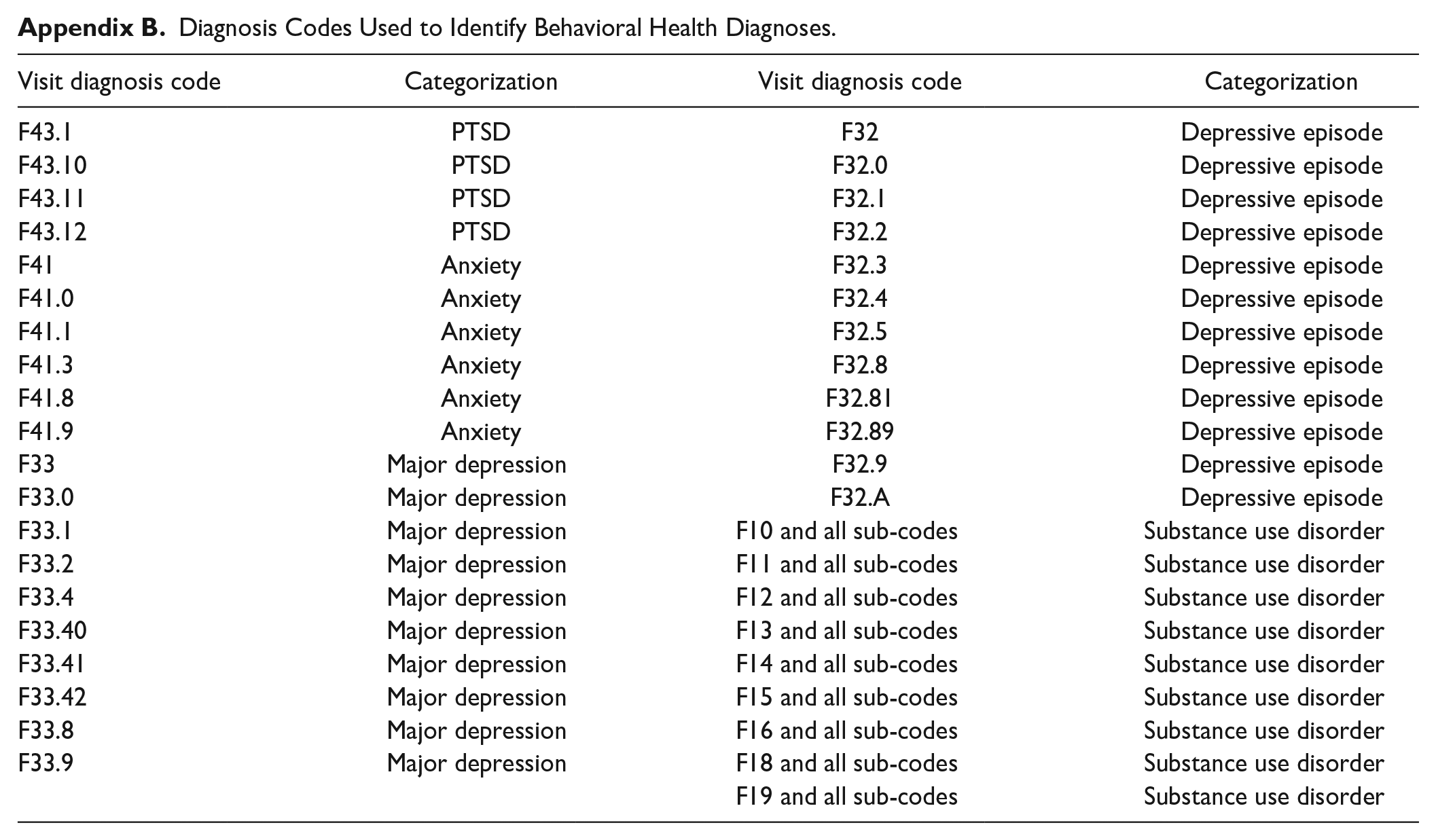
We defined the prevalence of PTSD as the percentage of patients with a PTSD diagnosis (see Appendix B for a full list of diagnosis codes included in analysis) during a visit for psychotherapy or psychiatry during a visit where the provide documented 1 or more diagnosis codes indicating PTSD.
Independent Variables
The primary independent variable of interest was the year over year change in PTSD prevalence in the population accessing integrated behavioral health services within health centers. Patient-level factors included in the analysis were age at last appointment during the year, legal sex, sexual orientation, indication of gender diversity, race, ethnicity, annual days of care (multiple visits during the same day were collapsed into 1 care day), social risk screening result (positive, negative, or unscreened), and other active behavioral health conditions. Gender diverse patients were identified in EHR data based on an algorithm that considers diagnosis and medical history, surgical history of gender reassignment, and structured EHR fields. 20 This algorithm went beyond basic demographic information to identify gender diverse patients.
Statistical Methods
The count of visits for PTSD and prevalence of PTSD were plotted by quarter and year. Recognizing that PTSD can present differently in adolescents and adults, we separately evaluated care among these 2 age groups. A generalized linear mixed model was used to evaluate PTSD care over 4 years. To account for the clustering of patients within clinics, the clinic identifier was included as a random effect. The diagnosis codes for the behavioral health conditions are provided in Appendix B.
Results
There were 182 419 distinct patients who received integrated behavioral health at one of the 200 clinics during the study period. Of these behavioral health patients, 13 205 (7%) were adolescents, 113 116 were (62%) female, and 37 350 (20%) were Black or African American; 6102 (3%) were determined to be transgender or gender diverse (TGD). See Table 1 for the full demographic profile of the patient sample (Table 2).
Demographic Characteristics of Adolescents and Adults Who Received Behavioral Health Care Across 200 Health Clinics From January 2019 to December 2022, by Post-Traumatic Stress Disorder (PTSD) Diagnosis.

Patients with unknown legal sex were excluded, due to an incomplete medical record. Legal sex is a required field in Epic.
Social determinants of health is a broad category, and each clinic has autonomy to determine which, and how many, social determinants of health they collect for patients. A patient was considered screened when at least 1 social risk domain was associated with a response.
Patients are included if they had a primary or secondary visit diagnosis during the year and at least 1 corresponding behavioral health visit during the year.
Exclusive of nicotine dependence.
Results of the Adjusted Generalized Linear Mixed Model of PTSD Treatment From 2019 to 2022.

The odds of having a PTSD diagnosis increased significantly from 2019 to 2022 (OR = 1.09, 95% CI = 1.08, 1.10). The percentage of adult behavioral health patients experiencing PTSD increased from 24.6% in the first quarter of 2019 to 31.6% in the fourth quarter of 2022 (Figure 1). Among adolescents, the percentage of individuals treated for PTSD (14%) was much lower than that in adults (27%). Data by quarter suggests a slight increase over the 4 years, with 13.4% of adolescent behavioral health patients being treated for PTSD in the first quarter of 2019, increasing to 17.2% in the fourth quarter of 2022. The percentage of adolescents who received care for PTSD peaked during 2020 and began to rise again in the third quarter of 2022. (Figure 2) Review of quarterly data suggests that PTSD was on an upwards trend prior to the start of the COVID-19 pandemic in March 2020, and that this increased trend continued across adolescent and adults for both males and females.

Adult patients (18-89) treated for PTSD in the behavioral health context by quarter 2019 to 2022.

Adolescent patients (12-17) treated for PTSD in the behavioral health context by quarter 2019 to 2022.
Multivariate modeling showed that specific patient populations experienced increasing odds of PTSD over the 4 years in this study: females were more likely to have a PTSD diagnosis compared to males (OR = 1.81, 95%CI 1.78-1.84). Patients who identify as Black or African American (OR = 1.09, 95% CI = 1.07, 1.12), identify as lesbian, gay, bisexual, queer, intersex, and asexual (LGBTQIA; OR = 1.29, 95% CI = 1.26, 1.33) or gender diverse individuals (OR = 1.36, 95% CI = 1.29, 1.42) had an increased odds of PTSD. Patients receiving care more frequently (defined as 7 or more days of care) also had a higher odds of PTSD compared to those with only a single visit (OR = 2.18, 95% CI = 2.13, 2.24) as did patients who screened positive for 1 or more social risks (OR = 1.52, 95% CI = 1.46, 1.57).
Discussion
This study shows that PTSD prevalence and treatment was increasing prior to the COVID-19 pandemic and continued to increase throughout 2022 among marginalized populations seeking care in health center settings. While lock-downs, job loss, and other conditions created during COVID-19 likely increased stress, trauma, and PTSD, quarterly review of PTSD prevalence from 2019 to 2022 showed a steady increase. This is likely due to a complex interplay of factors including the nature of PTSD presentation, behavioral health care access, and care seeking behaviors.
Consistent with previous findings, our study showed that people documented as females, Black or African American, or those who were identified as transgender or gender diverse were more likely to experience PTSD compared to people documented as male, white, or those who were presumed to be cisgender.2 -7 We also observed through data visualization that adult and adolescent females experience a higher prevalence of PTSD (Figures 1 and 2). The persistently higher prevalence is consistent with prior studies, suggesting that PTSD is related to multiple sociocultural and non-sociocultural factors in this population.2 -7,12 Our findings also demonstrated that among people who received care in health centers, those with PTSD were more likely to have frequent visits. This finding supports previous studies that PTSD is associated with greater healthcare utilization. 21 The finding that patients with other active behavioral health conditions had lower likelihood of comorbid PTSD was surprising as PTSD is often comorbid with depression, substance abuse, and anxiety disorder. 22 It is likely that this was due to diagnostic coding practices where clinicians may be documenting mental health comorbidities in provider notes rather than updating standardized EHR problem lists. 23
It is well documented that estimation of PTSD prevalence is challenging, as a wide variety of traumatic events may trigger PTSD 3 and that vulnerability and resistance to PTSD are largely variable. 24 Treatment capacity for PTSD is often lacking, especially among populations with low-income and/or public insurance. Finally, a complex interplay of factors can impact an individual’s choice to seek initial treatment and remain in treatment.
This study was conducted in health centers that offer integrated primary care and behavioral health care services. Health centers have been innovative and early adopters of integrated behavioral health models and were an essential source of behavioral health care for populations with a higher risk of PTSD through the pandemic.25,26 Health centers have innovated in the area of behavioral health care in recent years, with programs to improve access and increase the number of providers available. 27 However, health centers alone cannot solve persistent inequities in behavioral health access among underserved populations. 28 Significant new funding streams to bolster safety-net behavioral health clinics are designed to continue to address these gaps.29,30
Limitations of the current study include a clinic cohort that excluded free-standing behavioral health clinics and only comprised primary care clinics with integrated behavioral health care in health centers. 19 We limited the assessment of PTSD to behavioral health services and did not include care for PTSD provided during primary care visits. We recognize that primary care is an important venue to identify and manage PTSD, especially for safety-net populations who often have challenges with accessing behavioral health care.15,16,31 While screening for depression is recommended in primary care, there are no evidence-based guidelines at this time for PTSD screening for all primary care patients. 32 Our study is limited to patient EHR data collected at clinics within the OCHIN network. Care provided by therapists or psychiatrists in organizations not affiliated with OCHIN is not included in our study as these data were not available to the study team; this limitation would include referrals to outside organizations. It is therefore possible that PTSD prevalence may be underreported. Due to the optional nature of the collection of demographic data related to sexual orientation and gender identity, we may underreport PTSD prevalence in those populations. Despite these limitations, we measured PTSD the same way during each time period, and thus the trends over time are highly likely to be valid.
Health centers have invested significantly to increase behavioral health services to meet the needs of their patients.27,33 As PTSD prevalence continues to increase, there is a clear need for long-term strategies and investment in tailored PTSD care for the diverse populations served in health centers. Further study is warranted to track continued changes in PTSD prevalence and to investigate PTSD treatment modality (psychiatry vs psychotherapy) and care context (in-person vs telehealth) and the relationship between social risks and PTSD.
Footnotes
Appendix
Diagnosis Codes Used to Identify Behavioral Health Diagnoses.
| Visit diagnosis code | Categorization | Visit diagnosis code | Categorization |
|---|---|---|---|
| F43.1 | PTSD | F32 | Depressive episode |
| F43.10 | PTSD | F32.0 | Depressive episode |
| F43.11 | PTSD | F32.1 | Depressive episode |
| F43.12 | PTSD | F32.2 | Depressive episode |
| F41 | Anxiety | F32.3 | Depressive episode |
| F41.0 | Anxiety | F32.4 | Depressive episode |
| F41.1 | Anxiety | F32.5 | Depressive episode |
| F41.3 | Anxiety | F32.8 | Depressive episode |
| F41.8 | Anxiety | F32.81 | Depressive episode |
| F41.9 | Anxiety | F32.89 | Depressive episode |
| F33 | Major depression | F32.9 | Depressive episode |
| F33.0 | Major depression | F32.A | Depressive episode |
| F33.1 | Major depression | F10 and all sub-codes | Substance use disorder |
| F33.2 | Major depression | F11 and all sub-codes | Substance use disorder |
| F33.4 | Major depression | F12 and all sub-codes | Substance use disorder |
| F33.40 | Major depression | F13 and all sub-codes | Substance use disorder |
| F33.41 | Major depression | F14 and all sub-codes | Substance use disorder |
| F33.42 | Major depression | F15 and all sub-codes | Substance use disorder |
| F33.8 | Major depression | F16 and all sub-codes | Substance use disorder |
| F33.9 | Major depression | F18 and all sub-codes | Substance use disorder |
| F19 and all sub-codes | Substance use disorder |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Aging (R01AG074946) and the National Institute on Minority Health and Health Disparities (R01MD016389). The research reported in this work was powered by PCORnet®. PCORnet has been developed with funding from the Patient-Centered Outcomes Research Institute® (PCORI®) and conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a Clinical Research Network in PCORnet® led by OCHIN in partnership with Health Choice Network, Fenway Health, University of Washington, and Oregon Health & Science University. ADVANCE’s participation in PCORnet® is funded through the PCORI Award RI-OCHIN-01-MC.