
Abstract
Purpose:
To characterize COVID-19 vaccine uptake in patients with chronic conditions at the large university-based Family Medicine practice serving a population with low COVID-19 vaccine acceptance.
Methods:
A rolling panel of patients attributed to the practice was submitted monthly to the Chesapeake Regional Health Information Exchange (CRISP) to monitor patients’ vaccination status. Chronic conditions were identified using the CMS Chronic Disease Warehouse. An outreach strategy deploying Care Managers was developed and implemented. Associations between vaccination status and patients’ characteristics were examined using a multivariable Cox’s proportional hazard regression modeling.
Results:
Among 8469 empaneled adult (18+) patients, 6404 (75.6%) received at least 1 dose of COVID-19 vaccine in December 2020 to March 2022. Patients were relatively young (83.4% <65 years old), predominantly female (72.3%), and non-Hispanic Black (83.0%). Among chronic conditions, hypertension had the highest prevalence (35.7%), followed by diabetes (17.0%). Associations between vaccine status and the presence of chronic conditions varied by age and race. Older patients (45+ years old) with diabetes and/or hypertension showed a statistically significant delay in receiving COVID-19 vaccine, while young Black adults (18-44 years old) with diabetes complicated by hypertension were more likely to be vaccinated compared to patients of the same age and race with no chronic conditions (Hazard ratio 1.45; 95% CI 1.19,1.77; P = .0003).
Conclusions:
The practice-specific COVID-19 vaccine CRISP dashboard helped to identify and address delays in receiving COVID-19 vaccine in the most vulnerable, underserved populations. Reasons for age and race-specific delays in patients with diabetes and hypertension should be explored further.
Keywords
Introduction
The COVID-19 pandemic had a profound effect on individuals with chronic diseases 1 with high morbidity and mortality.1-3 In addition, COVID-19 disproportionately affected socioeconomically vulnerable populations, leading to a high number of individuals with severe COVID-19-related illness, hospitalizations, and deaths.4,5 Non-Hispanic Black people residing in low-income neighborhoods have higher rates and suboptimal control of chronic conditions due to low utilization of health care services and poor compliance, 6 and are experiencing poor COVID-19 infection outcomes.4,5
One of the most important public health measures to prevent SARS-CoV-2 infection and mitigate its transmission is vaccination.7-9 COVID-19 vaccines became first available for high-risk exposure groups (health workers) on December 14, 2020. Eligibility was gradually expanded from January to March 2021 to other high-risk groups, including 65+ years old seniors. The vaccines became available to the general adult population on April 19, 2021. However, conflicting statements by the government, industry, healthcare, and community leaders resulted in widespread misinformation and mistrust of COVID-19 vaccine.4,5,9 As a result, low initial uptake of COVID-19 vaccine was observed in vulnerable demographic groups, including racial minorities, due to low health literacy and poor access to trusted sources of information.10,11 Such delay in acceptance or refusal of vaccination despite the availability of vaccination services is considered to be a main characteristic of vaccine hesitancy. 12 In addition, disparities in vaccine access have been identified as a significant contributor to low vaccination rates in Maryland. However, the situation has quickly improved due to the statewide equity-focused efforts, including the state’s Vaccine Equity Task Force, local governments, health care, and other organizations. 13
Primary care clinicians are trusted information providers to communities, with the highest likelihood of instilling confidence about the vaccine in their patients, including those most distrustful of the healthcare system. 14 Since the beginning of the COVID-19 pandemic, the University of Maryland Family Medicine (UFM) ambulatory practices found themselves on the frontline for the COVID-19 response in Maryland and created an efficient, effective, adaptive response to the pandemic.15,16 This study aims to describe the progression of COVID-19 vaccine uptake by UFM patients with chronic diseases.
Methods
Practice Description
The UFM offices provide primary and immediate care at 4 sites with 55 000 patient visits per year. The West Baltimore clinics are located in an underserved urban area with a Persistent Poverty designation by the Congressional Research Service. 17 The Howard County sites serve a more socioeconomically and racially diverse patient population. All sites use the Epic Electronic Health Records (Verona, Wisconsin) and offer all FDA-approved COVID-19 testing and vaccines.
Data Sources
Rolling panels of the UFM patients with at least 2 encounters during preceding 18 months were generated automatically in Epic and submitted to the Chesapeake Regional Health Information Exchange (CRISP) each month. Patients were matched against a statewide list of all individuals who have received COVID-19 vaccine at any site in Maryland. In collaboration with CRISP, a dashboard-type report has been developed to monitor vaccination progress for all patients attributed to the UFM practice. Reports were downloaded from the dashboard on the second day of the following month. These reports included the date of vaccination, vaccine type, treatment site, and demographic data (age, sex, race, Hispanic ethnicity). In addition, CRISP used the CMS Chronic Disease Warehouse to identify chronic conditions, including diabetes (type I and type II), hypertension, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), asthma, heart failure (HF), and stroke.
Outreach Activities in the UFM
The UFM followed the CDC best practice recommendations to address vaccine mistrust using the 3 C’s approach (complacency, convenience, confidence). 17 Using monthly CRISP reports, patients were prioritized based on the presence of multiple chronic conditions by Care Managers, who were registered nurses supervised by the practice’s clinical director. Care managers received training in how to use CRISP data and engage with unvaccinated patients. During outreach, they informed patients about CDC recommendations for COVID-19 vaccination, discussed patients’ eligibility, addressed vaccine mistrust and misconceptions, provided information on its safety and efficacy, arranged for an appointment at the patient’s preferred site, and assisted with transportation. All these activities were part of the Care Managers’ routine practice.
Study Design
A single-group retrospective dynamic cohort study.
Data Analysis
Data were analyzed using SAS 9.4 software (SAS Institute, Cary, NC). Statistical significance was established at two-sided α = .05. The primary outcome was the probability (hazard rate) of receiving at least 1 dose of any FDA-approved vaccine. Predictors included demographic (age, sex, race) and clinical characteristics (chronic conditions). The exact dates of diagnosis for chronic conditions were not available; therefore, we treated them as a baseline characteristic. Children (<18 years old) were excluded because of the very low prevalence of chronic conditions and changing eligibility criteria for vaccination.
Since the UFM practices serve a predominantly non-Hispanic Black population, we compared COVID-19 vaccination progress in this group with other race and ethnic groups, which included 64.7% non-Hispanic White, 10.2% non-Hispanic Asian, and 15.0% Hispanics regardless of race (Supplemental Table 1). Correlations between the presence of chronic conditions were assessed using Pearson correlation coefficient.
Associations between outcomes and predictors were initially examined using χ2 test for proportion followed by Kaplan-Meier survival curves analysis. Finally, a multivariable Cox’s proportional hazard regression modeling was used. Covariates were identified based on preliminary bivariate analyses looking for potential effect-measure modifiers.
We chose December 2, 2020, as a starting point for time-to-event analyses. For patients who received a vaccine, follow-up time (days) was defined as a difference between the date of their first recorded vaccination event and December 2, 2020. Follow-up time for unvaccinated patients was calculated as a difference between the second day of the month in which their name last appeared on the vaccine report and December 2, 2020.
We also accounted for different vaccine eligibility criteria before and after April 19, 2021. Patients who received their first vaccine dose before April 19, 2021, and unvaccinated patients who first appeared on the UFM panels in March to April 2021 were assigned to time zone 1. Those who received a vaccine after April 19, 2021, and unvaccinated patients who first appeared on the panels generated on 05/02/2021 or later were assigned to time zone 2. However, in the chosen modeling approach, the effect of the time zone was not estimated directly. 18
Results
Study Population
Overall, 8469 adult patients were empaneled between December 2, 2020, and April 1, 2022. Among them, 5387 patients (63.6%) joined the panel on or before 04/02/2021. The median time of FU was 147 days, range 14 to 485 days.
The study population was relatively young (83.4% <65 years old), predominantly female (72.3%), and non-Hispanic Black (83.0%); 35.7% had at least 1 of 7 chronic conditions monitored through the CRISP. Hypertension had the highest prevalence (24.2%), followed by diabetes (17.0%) (Table 1). Asthma was the most prevalent condition among 18 to 44 years old patients (59.9%), diabetes had the highest prevalence in the 45 to 64 year age group (50.8%), while HF was the most frequent among elderly patients (44.1%) (Table 1). Among young patients, 22.4% had at least 1 chronic condition; the proportion increased to 53.8% in the 65+ years old population (Table 1).
Demographic and Clinical Characteristics in the UFM-Empaneled Adult Population by Age Groups (March 2, 2021-April 1, 2022, N = 8469).
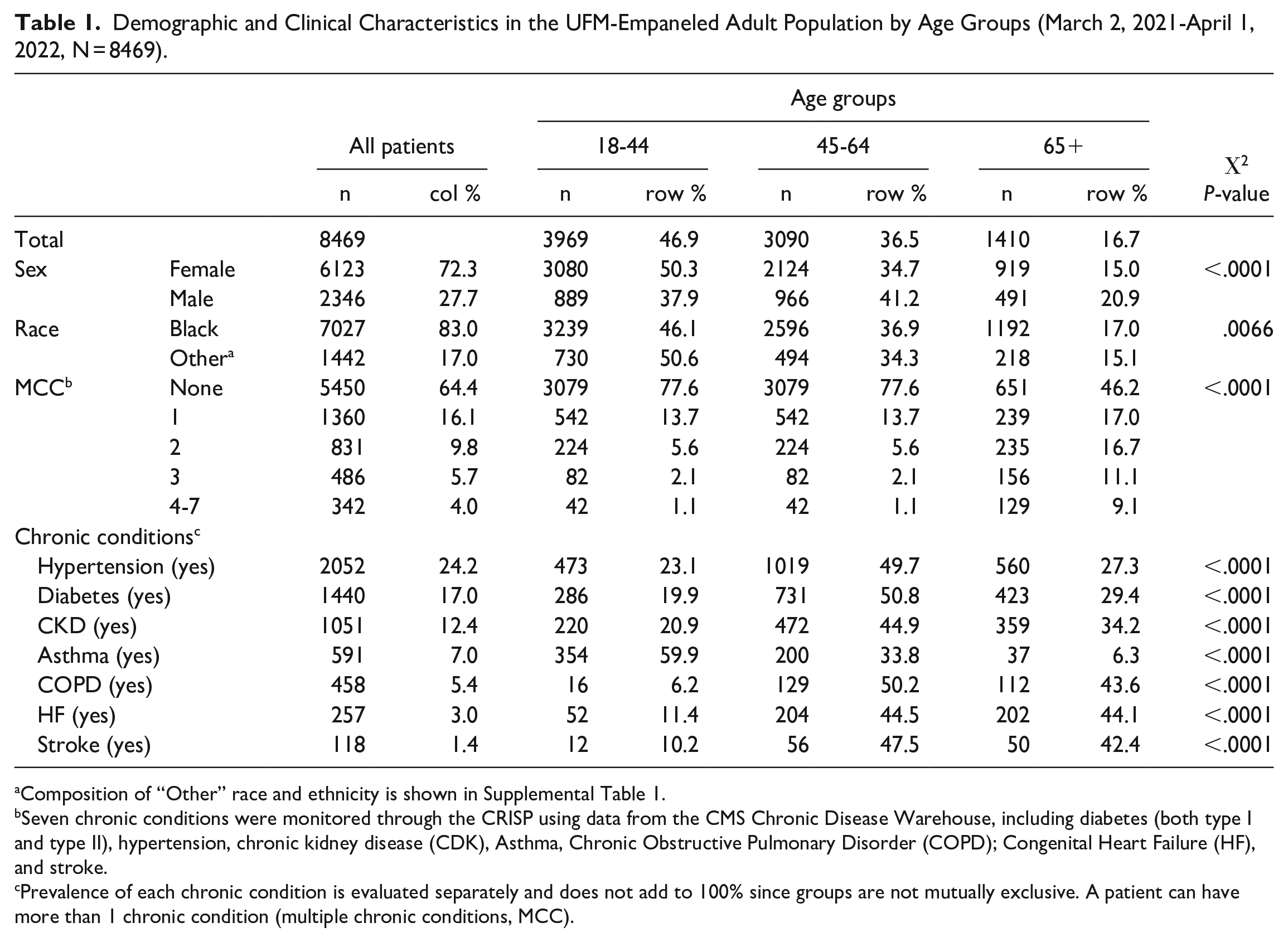
Composition of “Other” race and ethnicity is shown in Supplemental Table 1.
Seven chronic conditions were monitored through the CRISP using data from the CMS Chronic Disease Warehouse, including diabetes (both type I and type II), hypertension, chronic kidney disease (CDK), Asthma, Chronic Obstructive Pulmonary Disorder (COPD); Congenital Heart Failure (HF), and stroke.
Prevalence of each chronic condition is evaluated separately and does not add to 100% since groups are not mutually exclusive. A patient can have more than 1 chronic condition (multiple chronic conditions, MCC).
Correlation analysis showed that diabetes was often associated with hypertension (coefficient correlation ρ = .43). In addition, the presence of CKD had the highest correlation with diabetes and hypertension. The presence of other chronic conditions had a low correlation between each other and diabetes or hypertension (Supplemental Table 2).
Vaccination Progress in the UFM-Empaneled Patient Population
Cumulatively, 6404 UFM-empaneled adult patients (75.6%) received at least 1 dose of the COVID-19 vaccine during the study period. The proportion of vaccinated individuals was the highest among the elderly (85.1%) and the lowest among young adults (66.8%) (Supplemental Table 3). There was a significant difference in the proportion of vaccinated individuals between Black and other ethnic groups (73.7% and 85.0%, respectively) (Figure 1 and Supplemental Figure 3). This was mostly due to the delay in receiving vaccination among young Black patients (62.9%) compared to the patients from other ethnic groups of the same age (84.1%) (Figure 1 and Supplemental Figure 3).
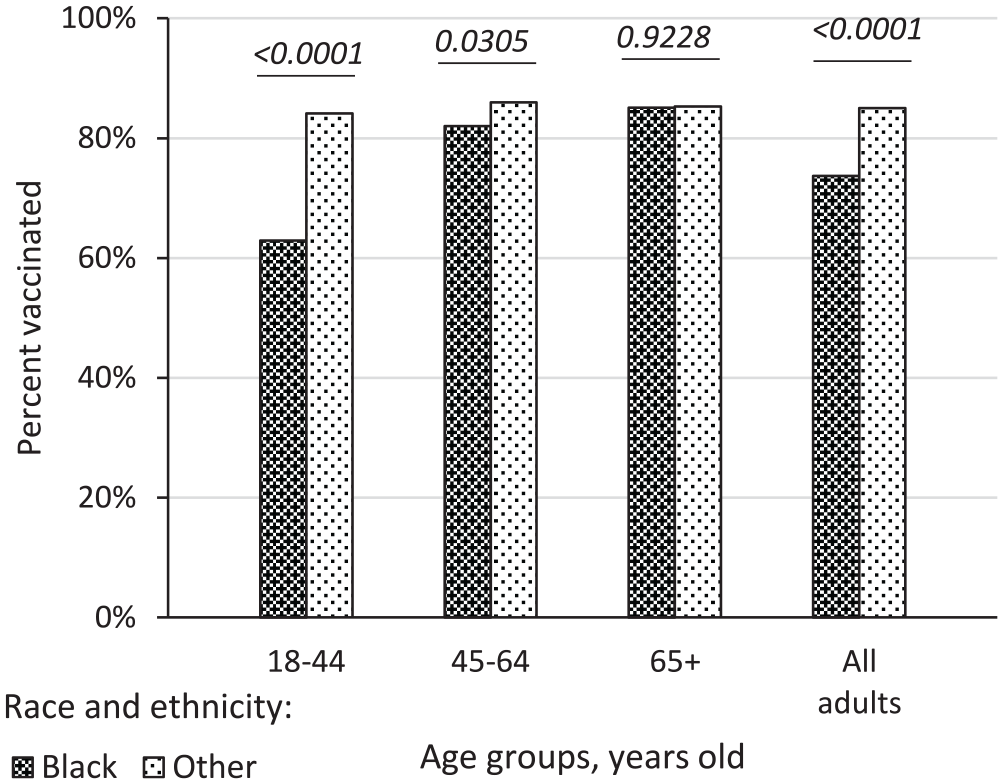
Proportion of COVID-19 vaccinated adult patients in the UFM-empaneled adult population by age and race (03/02/2021-04/01/2022). Proportions of patients who received at least 1 dose of COVID-19 vaccine within each age and race stratum are shown. Black non-Hispanic patients are compared to “Other” race and ethnicity group. Composition of “Other” group is shown in Supplemental Table 1. Frequencies in each stratum are shown in Supplemental Table 3. Chi-square p values are for association between proportion of vaccinated patients by race in each age stratum.
The analysis revealed that the proportion of vaccinated patients varied by chronic condition status (Figure 2 and Supplemental Table 3). Because of the highest prevalence and correlation between diabetes, hypertension, and CKD, we first evaluated vaccination progress in patients with all possible combinations of these 3 conditions (data not shown). The analysis revealed that patients who had diabetes and hypertension (regardless of CKD or other chronic diseases status) had the highest proportion of COVID-19-vaccinated individuals (84.7%) compared to patients who had either diabetes or hypertension (75.7%) or other chronic conditions (69.1%). The differences were most remarkable in the youngest patients (Figure 2 and Supplemental Table 3).
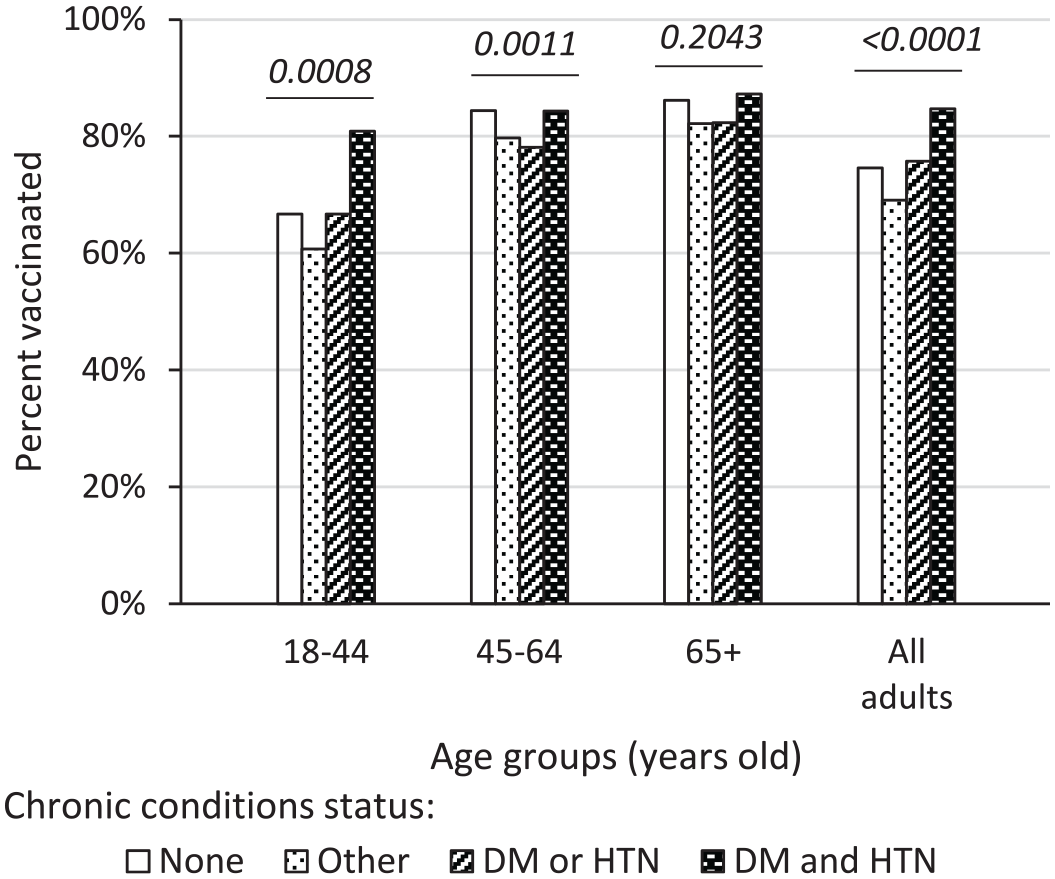
Proportion of COVID-19 vaccinated adult patients in the UFM-empaneled adult population by age and chronic conditions status (03/02/2021-04/01/2022). Proportions of patients who received at least 1 dose of COVID-19 vaccine within each age and chronic condition stratum are shown. Seven chronic conditions were monitored through the CRISP using data from the CMS Chronic Disease Warehouse. “Other” chronic conditions included chronic kidney disease, asthma, chronic obstructive pulmonary disease, heart failure, and stroke. Patients with both type I and type II diabetes were included. Chi-square P values are for association between proportion of vaccinated patients by chronic conditions in each age stratum. Frequencies in each stratum are shown in Supplemental Table 3. Abbreviations: DM, diabetes; HTN, hypertension.
Since our study population represented a rolling panel with a substantial loss of follow-up of patients who have not met empanelment criteria, as well as the addition of new patients who become eligible for inclusion into the panel during the study period, we also used a Kaplan-Meier “survival” analysis to assess COVID-19 vaccination progress. The results showed that there were statistically significant associations between age, race, sex, and the progress of COVID-19 vaccination expressed as the median time to get the first dose of the vaccine (relative to 12/2/2020). Vaccination progress was fastest in the elderly (65+ years old), males, patients from ethnic groups other than non-Hispanic Black, and those with diabetes complicated by hypertension (Supplemental Figure 1).
Multivariable Regression Model for the Probability of Accepting the COVID-19 Vaccine
We also assessed COVID-19 vaccination progress in the UFM-empaneled patients using a multivariable Cox’s proportional hazard regression model that included demographic characteristics (age groups, sex, Black race) and the presence of chronic conditions as predictors of delays in receiving a vaccine. Adjusting for other predictors, an association between vaccine status and sex was not statistically significant; therefore, sex was excluded from the final model (data not shown). Preliminary analyses of interaction terms revealed that age and Black race were effect-measure modifiers for the association between vaccine status and the presence of chronic conditions (and vice versa). Therefore, we stratified the analysis on age and included interaction terms between race and the presence of chronic conditions.
The estimates produced by the model are shown in Table 2. After adjustment for other factors in the model, the vaccination rate (hazard) for young Black patients (18-44 years old) with diabetes complicated by hypertension was 1.45 times higher than for patients of the same age and race who did not have chronic conditions (HR = 1.45; 95% CI 1.19, 1.77; P = .0003). In contrast, patients from other ethnic groups of the same age demonstrated a general trend of delay in receiving a vaccine. In the 45 to 64 years old group, such a trend was observed in patients with all chronic conditions regardless of race. For elderly patients (65+ years old), the differences in the vaccination rate were not statistically significant depending on race or chronic conditions. The exception was non-Black patients with chronic conditions other than diabetes or hypertension, where vaccination rate was 1.8 times higher than for those without chronic conditions (HR = 1.84; 95% CI 1.08, 3.12; P = .0238) (Table 2).
COVID-19 Vaccination Progress in the UFM-Empaneled Adult Patients: Results of Multivariable Cox’s Proportional Hazard Regression Model. a
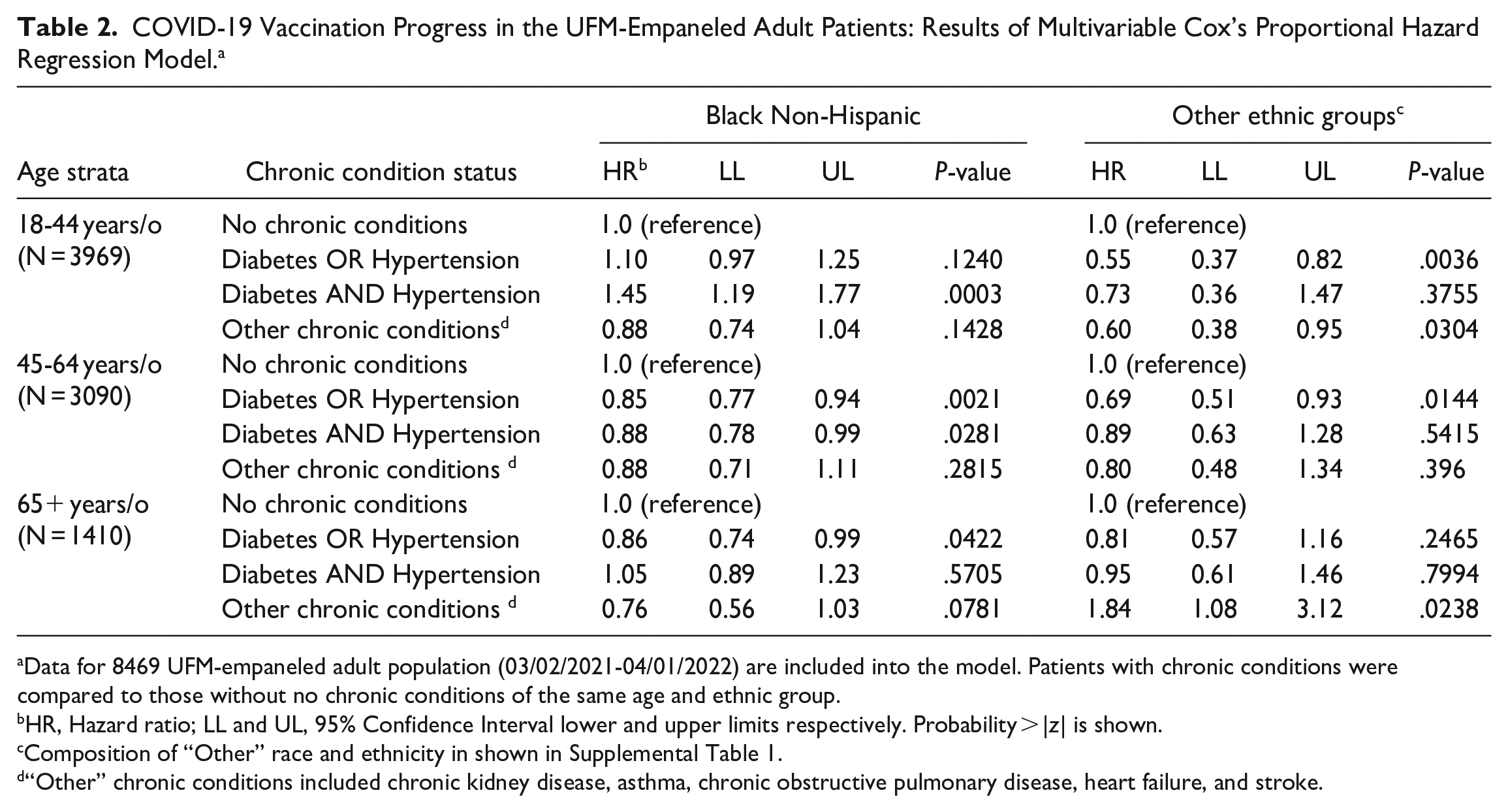
Data for 8469 UFM-empaneled adult population (03/02/2021-04/01/2022) are included into the model. Patients with chronic conditions were compared to those without no chronic conditions of the same age and ethnic group.
HR, Hazard ratio; LL and UL, 95% Confidence Interval lower and upper limits respectively. Probability > |z| is shown.
Composition of “Other” race and ethnicity in shown in Supplemental Table 1.
“Other” chronic conditions included chronic kidney disease, asthma, chronic obstructive pulmonary disease, heart failure, and stroke.
Discussion
The UFM serves neighborhoods characterized by persistent poverty and low access to health care. 17 The patient panel is comprised of relatively young, predominantly female individuals, the vast majority of whom are non-Hispanic Black. At the beginning of the COVID-19 pandemic and early COVID-19 vaccine availability, all these demographic subgroups were characterized by a high degree of mistrust in the safety and effectiveness of the COVID-19 vaccines.6,7,10 These mistrust and misconceptions were exacerbated by problems with access to vaccine sites in minority communities, associated confusion with multiple vaccine options, slow roll-out, and availability of vaccines at primary care sites. 19 Creation of the UFM practice-specific COVID-19 vaccine dashboard by the CRISP was the first step in identifying early patterns of vaccine acceptance in patients served by the UFM. Vaccine hesitancy is complex and context-specific, varying across time, place, and vaccine type, and is influenced by factors such as complacency, convenience, and confidence. Although we have not measured the 3C’ components, this approach was implemented in the UFM as the CDC best practice recommendations. Moreover, the time-to-event analysis employed in our study (Kaplan-Meier’s “survival” analysis and Cox proportional hazard modeling) directly measured a delay in receiving a vaccine, which is a major indicator of vaccine hesitancy. 12
To educate and inform patients about the COVID-19 vaccine, the UFM leadership organized active outreach to patients with chronic diseases to ensure that patients were engaged by providers whom they knew and trusted. We expected that trusted messenger outreach would lead to an increase in COVID-19 vaccination rates in vaccine-hesitant Black individuals. 20 Our data indirectly support this hypothesis. Among patients aged 45+ years old without chronic conditions, proportions of vaccinated individuals were similar regardless of race (83.8%-86.6%). Kaplan-Meier’s curves showed slower vaccine uptake among Black patients compared to other ethnic groups during the early periods of the vaccination campaign. The race-specific gap gradually closed during later periods (Supplemental Figure 1). Our observations are consistent with a recent study by Padamsee et al, 10 who demonstrated that while vaccination rates continue to be lower among Black versus White individuals, intentions of Black individuals to be vaccinated increased more rapidly over time due to the strong educational outreach, advocacy, and trusted voices.
Stratification by age groups in our study population revealed that young adults (18-44 years old), who comprised almost half of the population, were major contributors to the overall race-specific slow vaccine uptake. It has been shown that younger individuals perceived COVID-19 to be a mild disease and were reluctant to accept COVID-19 vaccine.21,22 In addition, vaccination rates in our population varied depending on the presence of chronic conditions. We found that young Black adults who had diabetes complicated by hypertension were more likely to be vaccinated compared to patients of the same age and race with no chronic conditions or patients with diabetes or hypertension alone. This tendency was race-specific since young patients from other ethnic groups with similar chronic conditions were more likely to delay COVID-19 vaccination. This unexpected finding suggested that younger Black individuals were more likely to be vaccinated if they had 2 or more chronic conditions, 1 of which was diabetes. Although, in retrospect, patients with diabetes and hypertension could have been singled out from the beginning to receive the vaccine, the paucity of literature on prioritization of vaccine delivery at the start of the COVID-19 vaccination precluded systematic planning. Although we believe that our outreach impacted vaccination rates, we recognize that individuals in the community were receiving information through multiple sources, including outreach calls by primary care practices, public health messaging, radio, television, social media, and community groups. Health messaging clearly stated that diabetes placed patients at higher risk, which may also have played a role in the decision to receive a vaccine that were observed in our patient population.
Patients with diabetes and hypertension are more likely to present with severe COVID-related illnesses.23,24 Despite this increased risk, individuals with diabetes have delayed getting vaccinated for COVID-19.4,5 In our study, middle-aged (45-64 years old) patients with diabetes and/or hypertension were less likely to receive a COVID-19 vaccine compared to patients of the same age and race who did not have chronic conditions. This observation could be partially explained by some reports that persons with diabetes have shown periods of hyperglycemia shortly after receiving a COVID-19 vaccination. 25 The delay in vaccination in this specific age group rather than younger or older patients could also reflect the complex nature of vaccine acceptance. In our study, elderly (65+ years old) patients who had either diabetes or hypertension also demonstrated a delay in receiving COVID-19 vaccine, while the vaccination rate of those who suffered from diabetes and hypertension was not significantly different from the control group of the same age. This could be explained, at least in part, by targeted outreach from UFM to elderly patients with multiple chronic conditions.
One of the limitations of our study is that our data are derived from a single ambulatory care practice. The vaccine distribution from December 2020 to March 2021 was driven by a high risk of occupational exposure, for which data were not available. Technical limitations may be present since we could not control data sharing between EHR, CRISP, and vaccination sites in the state of Maryland. Lastly, this study is based on data from a large practice located in Baltimore, Maryland, that serves a historically segregated, persistent poverty population in Baltimore, thus leading to questions about generalizability to a more diverse population. In our study, we interpreted the delay in receiving COVID-19 vaccine as contributing to vaccine hesitancy. However, we cannot exclude that other unmeasured factors could contribute to the delay or refusal to get vaccinated.
In conclusion, the creation of the UFM practice-specific COVID-19 vaccine dashboard by the CRISP gave our practice a chance to improve COVID-19 vaccination in patients it serves through outreach with trusted providers in vulnerable, underserved populations. There is a need for increased research in patients with diabetes and hypertension to explore the reasons for age-dependent vaccine hesitancy and barriers to COVID-19 vaccines.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231175369 – Supplemental material for Characterization of the COVID-19 Vaccine Uptake in Patients With Chronic Diseases in a Large University-based Family Medicine Clinical Practice
Supplemental material, sj-docx-1-jpc-10.1177_21501319231175369 for Characterization of the COVID-19 Vaccine Uptake in Patients With Chronic Diseases in a Large University-based Family Medicine Clinical Practice by Niharika Khanna, Elena Klyushnenkova, Min Zhan, Dae Hyoun Jeong, Colleen Kernan and David Stewart in Journal of Primary Care & Community Health
Footnotes
Authors’ Note
The manuscript contents have not been previously presented.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Maryland School of Medicine, Department of Family and Community Medicine departmental funds.
Ethics
The exempt status of the study was confirmed by the University of Maryland Baltimore Institutional Review Board (reference number HP-00091542).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.