
Abstract
Introduction:
The UK Government partnered with industry to tackle cardiovascular disease (CVD) in the first NHS population health agreement. The ambition was to prevent 150 000 strokes, heart attacks and dementia cases over the next 10 years with a new siRNA LDL-C lowering therapy (Inclisiran) delivered within Integrated Care Services by primary care to support a comprehensive approach to lipid management. Following the approval of inclisiran, and guidance published by the National Institute for Health & Care Excellence (NICE) on its use, this paper has been created by a UK general practice to share real-world observations of cases and the potential service benefits of rolling out this innovative drug treatment. The process of identifying patients at risk of atherosclerotic cardiovascular disease (ASCVD) and lessons learned from implementing in practice is also addressed. Workstreams were developed to rapidly roll out a low clinical burden enhanced lipid management program incorporating siRNA LDL-C lowering therapy into primary care practice.
Approach/Method:
(1) Multi-disciplinary team (MDT) education program based on freely available Academic Health Science Network (AHSN), National Institute for Health & Care Excellence (NICE), and commercial materials. (2) Automated searches using a software program were run to identify “at-risk” patients alongside manual case-finding in everyday clinics. (3) Patients were invited for review using multi-channel modalities. (4) Where appropriate, treatment was commenced after consent was obtained. (5) Automated recall systems are used to ensure follow-up; initially at 3 months, then every 6 months.
Discussion and Conclusions:
Enhanced lipid management as a secondary prevention measure is achievable in line with national guidance and objectives. The methodology and education/training processes used in combination with reconstructing the management process can help practice staff realize the program benefits, which in turn can lead to a shift in behavior where all staff embed manual case-finding of high-risk patients into everyday consultations and reviews; enabling rapid identification of eligible patients. Taking a multi-disciplinary, holistic approach to new initiatives reduces service burden, particularly for GPs. Leveraging resources from the AHSN and others removes additional training pressures often associated with new initiatives and provides a wealth of educational material to support primary care MDT upskilling.
Keywords
Introduction and Background
Cardiovascular disease causes one death every 3 min, almost a quarter (24%) of all deaths in the UK. 1 It is also one of the conditions most strongly associated with health inequalities (Figure 1), with many people living with undetected, high-risk conditions, such as high cholesterol.2,3 In particular, people living in the most deprived areas in England are almost 4 times as likely to die prematurely from cardiovascular disease than those in the least deprived. 3 This, combined with the estimated £7.4 billion per year financial burden to the NHS, 4 has led to cardiovascular disease being cited as “the single biggest area where the NHS can save lives over the next 10 years” 2 with the identification of at-risk people for optimal lipid management specified as one of five priority areas requiring accelerated improvement through NHS England and NHS Improvement’s Core20Plus5 program. 5
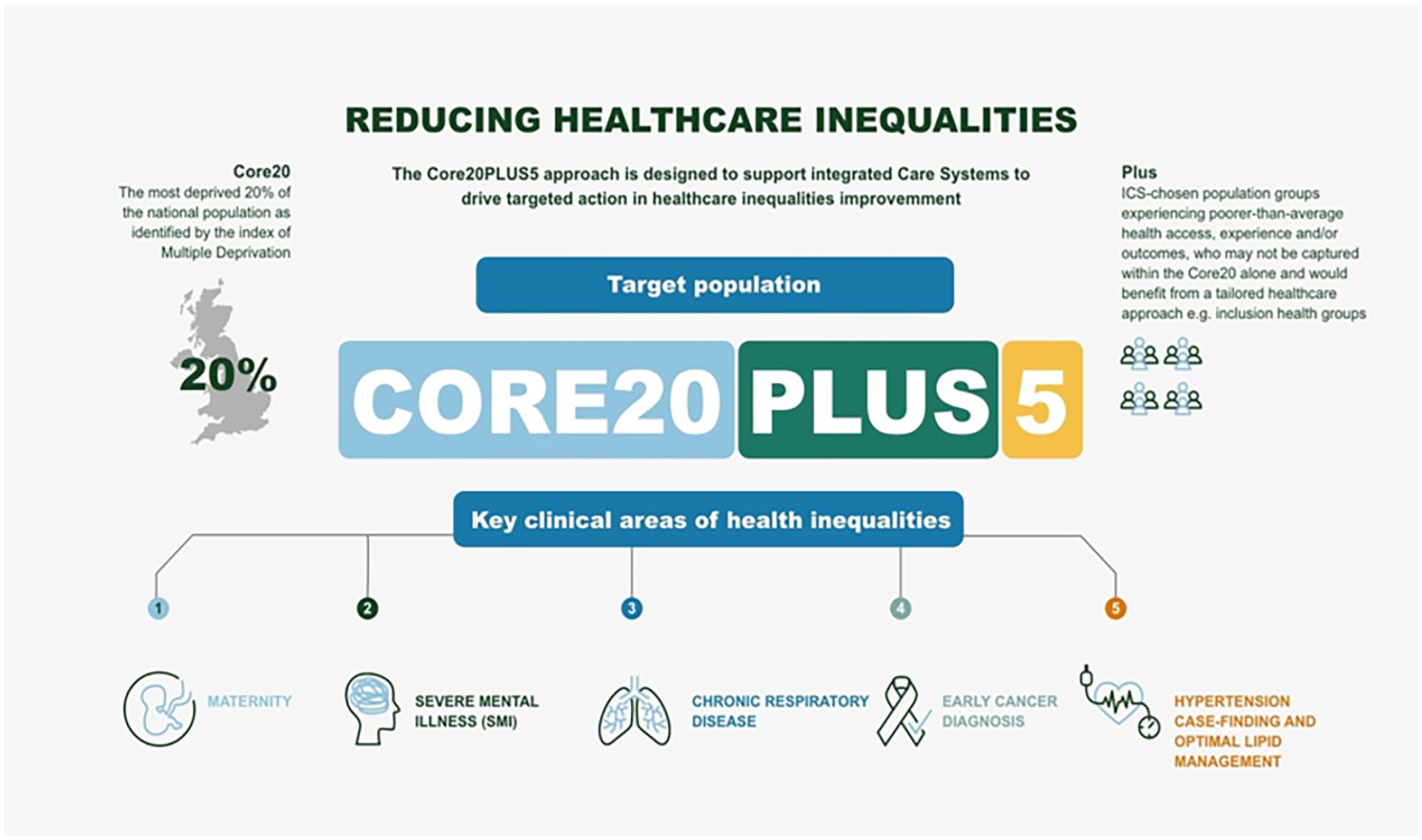
Core20Plus5 approach (adapted from NHS England 5 ).
To support the drive for optimal lipid management, NHS England, the Accelerated Access Collaborative (AAC), the Academic Health Science Network (AHSN), and a pharmaceutical partner are collaborating on the rollout of a population health agreement, using a siRNA (small interfering ribonucleic acid) LDL-C (Low-density lipoprotein cholesterol) lowering therapy (inclisiran) in primary care. Following the approval of inclisiran, and guidance published by the National Institute for Health & Care Excellence (NICE) on its use, this paper has been created by a UK general practice to share real-world observations of cases and the potential benefits of this innovative treatment. The process of identifying patients at risk of atherosclerotic cardiovascular disease (ASCVD) and lessons learned from implementing in practice will also be addressed. As this rollout is in its infancy, further work is needed before publishing demonstrable wide-scale efficacy and benefits.
The authoring practice of this case study is in a rural English county with a high prevalence of cardiovascular disease affecting 160 000 of a population of 756 000 (2019), resulting in 290 deaths each month. 6 At the time of the rollout, the practice population was 6542 (31 March 2022), with the subset of “at-risk” patients eligible for inclisiran significantly higher than the national average:
Stroke—203.1%
Peripheral arterial disease—165.1%
Ischemic heart disease—183.3%
The practice team were therefore keen to champion this preventative approach, using data-driven insights alongside this innovative therapeutic intervention to find and treat patients at risk.
Optimal Lipid Management—Enhancing the Therapeutic Approach
LDL-C is a well-established, modifiable risk factor in the development of ASCVD,7,8 a condition that affects over 3 million people in the UK (Figure 2). 9 Sustained LDL-C lowering can help prevent the development and progression of cardiovascular events associated with ASCVD,5,6 ultimately reducing mortality. 8 This is even more critical in patients with other comorbidities (diabetes, chronic kidney disease, and polyvascular disease) as a drop in LDL-C can even more significantly reduce the risk of major adverse cardiovascular events compared to patients with higher levels of LDL-C in this cohort. 10

Impact of elevated LDL-C.
Traditional lipid-lowering methods, alongside the prescription of statins and other lipid-lowering medications, have varying abilities to lower LDL-C up to a maximum reduction of 60%. 8 Whilst the safety profile of statins is considered satisfactory, statin monotherapy is unlikely to achieve LDL-C goals for most patients,8,11 therefore additional LDL-C lowering is often needed 11 and must be maintained.12,13 There are also disadvantages and risks associated with statins, including intolerance, 14 adverse reactions, 15 increased risk of developing type 2 diabetes, 16 and adherence to once-daily doses. 17
Other therapies, such as inclisiran, have therefore been introduced to the market as either an alternative to or in addition to a statin. Inclisiran is an innovative LDL-C-lowering therapy administered via subcutaneous injection as monotherapy or in addition to other lipid-lowering therapies, 18 with the convenience of 2 doses a year. It works differently from other lipid-lowering therapies by preventing the production of PCSK9 in the liver.18,19 Instead of blocking circulating PCSK9 like other LDL-C-lowering therapies, inclisiran, as a siRNA therapy, interferes with the RNA that codes for this protein, reducing its production in the first place.18,19
Inclisiran has been available to prescribe in the UK since September 2021 and is indicated in adults with primary hypercholesterolemia (heterozygous familial and non-familial) or mixed dyslipidaemia, as an adjunct to diet (a) in combination with a statin or statin with other lipid-lowering therapies in patients unable to reach LDL-C goals with the maximum tolerated dose of a statin, or (b) alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant, or for whom a statin is contraindicated. 20
The national guidance for lipid management for secondary prevention of cardiovascular disease, 21 published by NICE in October 2021, recommends inclisiran as an option for the treatment of adult patients who have already had certain cardiovascular events*, and have persistently elevated LDL-C levels (≥2.6 mmol/L) despite a maximum tolerated dose of statins with or without other lipid-lowering therapies or other lipid-lowering therapies when statins are not tolerated or are contraindicated. 22
* Cardiovascular events include acute coronary syndrome (such as myocardial infarction or unstable angina needing hospitalisation), coronary or other arterial revascularisation procedures, coronary heart disease, ischaemic stroke or peripheral arterial disease.
Objectives
The approach to address this unmet burden in primary care is to optimize lipid management in high-risk patients using siRNA LDL-C lowering therapy when clinically indicated; closing the gap between guidelines and clinical practice through a proactive, holistic, population health management approach to achieve optimal lipid control. The specific objectives in this rural practice were to:
Offer appropriate treatment to the large “at-risk” patient population
Optimize key areas of the pathway, improving lipid management via the appropriate use of high-intensity statins, ezetimibe, and bempedoic acid
Introduce inclisiran into the lipid management pathway in line with the NICE guidelines
Methodology
The practice took a proactive approach to identify patients at risk that would potentially benefit from inclisiran using a 2-step process:
Case finding
Case review
Before the program commenced, multi-disciplinary training sessions were undertaken to upskill the clinical team around optimal lipid management; ensuring the team had the right knowledge and skills to understand how to incorporate this new treatment option successfully. The content and materials were in keeping with NICE guidance and were provided by the local Academic Health Science Network (AHSN) and from commercial sources.
Case-Finding
Searches were run through the EPR (electronic patient record) using an embedded clinical decision support tool which searched, filtered, and identified “at-risk” patients that would benefit from a review. The criteria used for the case-finding tool comprised:
History of cardiovascular events,
LDL-C ≥2.6 mmol/L
EPR case finding was carried out using existing technologies within the practice and did not necessitate investment in new systems or IT infrastructure.
In addition, practice staff were trained to identify “at-risk” patients during long-term condition consultations (eg, diabetes reviews). Expanding the search for “at-risk” patients in this way was important in the context that this enhanced lipid management approach commenced when the country was starting to emerge from the COVID-19 pandemic. The pandemic had not only created pathology service backlogs but also led to fewer patients presenting for tests to identify “at-risk” factors that would support EPR-related case-finding methods.
Case Review and Management
The notes of the patients identified in the case-finding process were reviewed on an individual basis to determine if they were “at-risk.” If so, they were invited to a secondary prevention cardiovascular disease review. With access to patients ever a challenge, multi-channel modalities were used to ensure appointments were as accessible as possible. To ensure this process did not place an unnecessary burden on a general practitioner (GP), the initial reviews were performed by a physician associate (PA).
A holistic approach to case management was undertaken by the PA with information and/or treatment being delivered on a case-by-case basis which may include one or more of the following:
Confirmation of
Where it was clinically indicated that a patient would benefit from inclisiran, they were offered the medication and on acceptance, assigned an appropriate in-person appointment for their injection. To minimize clinical burden, a range of qualified healthcare providers gave subcutaneous injections of inclisiran under patient-specific directives (PSDs) where required. Automated recall systems were used to ensure follow-up treatments; initially at 3 months, then every 6 months thereafter.
Whilst clinical training sessions help educate practice staff on treatment options, no skills-based training was required to administer inclisiran. Those involved likened it to “the delivery of a Vitamin B12 injection.” For non-prescribers, patient-specific directives were created to allow them to administer the treatment safely and effectively. This simple and quick delivery mechanism also benefits the patient.
Results
In January 2022, 14 “at-risk” patients were identified as a result of searches performed on the practice’s EPR, increasing to 77 patients in March 2022. This was anticipated as more patients received up-to-date lipid profiles as we emerged from the restrictions and backlogs caused by the pandemic. This upward trend of case identification continued throughout 2022.
Patients responded positively to the offer of an effective lipid-lowering therapy that did not add to their current medication burden, with many citing “ease of administration” and “peace of mind” as key drivers for their continued engagement. Practice staff were equally enthusiastic about the process, particularly as it lowered the risk of non-adherence; a problem which affects up to 50% of patients taking statin therapy who stop taking their medication within 12 to 18 months. 23
To date, inclisiran has been well tolerated with no significant side effects and anticipated levels of adherence.
Example cases are detailed in Figures 3–5.

Case study—patient A.

Case study—patient B.

Case study—patient C.
Discussion
Managing high-risk cardiovascular conditions is difficult in time-pressured GP consultations where multimorbidity is the norm. Therefore, taking a multi-disciplinary approach to enhanced lipid optimization has several benefits including:
The potential to mitigate the risk of complications by taking a population health management approach to disease management
Reducing the service burden across primary practice, specifically for GPs, as cases can be assessed by other appropriately trained healthcare professionals
Allowing for rapid review and commencement of treatment
Encouraging a culture of shared learning best practice into everyday clinics
Increasing knowledge and awareness of cardiovascular prevention across clinical teams
At a system level, education and embedding preventative programs of this nature into patient pathways could also provide the opportunity to create a more collaborative approach between primary and secondary care; working together to identify the optimization potential for the benefit of patient care and secondary prevention.
Whilst this paper is focused on the embedding of a process into practice, it is noteworthy that early efficacy data is positive and in line with the LDL-C reductions observed in the ORION-10 11 and ORION-11 23 studies. There has been much discussion around whether the European guidelines outlining an LDL-C reduction target of >50% from baseline and an LDL-C goal of <1.4 mmol/L (<55 mg/dL) for patients at very-high risk 8 is achievable. The case studies in this paper indicate this is not only a realistic target but one that could be surpassed in populations where ASCVD is more prevalent and primary care teams work collaboratively, taking a holistic secondary prevention approach.
In pursuit of national targets, a holistic approach to lipid optimization can deliver more than just an overview of how medication can support the patient. It helps patients understand that lifestyle and dietary changes can significantly impact their quality of life and discussing these factors as part of a therapeutic intervention can facilitate a better relationship between the clinician and patient.
Further work needs to be carried out to determine the number of patients in a typical primary care practice that would fit the criteria for being at risk and therefore eligible for treatment. Early estimates from NHS England indicate that circa. One percent of patients will benefit from inclisiran but it is anticipated that this could be higher in some localities depending on the profile of the patient population. With the prevalence of ASCVD risk factors higher in the authoring practice, a projected 1.6%-2% (105-131) of the 6542 population it serves will benefit from this intervention over time.
As a side note on the technology, the ability to case-find through the EPR will often be subject to the maturity of the software and the completeness of the patient record. Some software providers include pre-programed filters which could facilitate case finding and reduce implementation time but it is always advisable to discuss the potential of these opportunities with your software provider to ensure you are making the most out of your current implementation.
Conclusion
Automation of case-finding searches within the electronic patient record enables prompt identification of eligible patients with resulting treatment then being rapidly and easily administered.
The methodology and education/training processes used in combination with reconstructing the management process can help practice staff realize the program benefits, which in turn can lead to a shift in behavior where all staff embed manual case-finding of high-risk patients into everyday consultations and reviews.
Footnotes
Acknowledgements
The Authors would like to acknowledge the team at Marsh Medical Practice for seamlessly incorporating this new way of working into the practice.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marsh Medical Practice was in receipt of a non-promotional funding grant from East Midlands Academic Health Science Network (EMAHSN) for this work. The Authors had full access to the study data to produce the report. Access for the authors and their associates on behalf of Marsh Medical Practice is ongoing as the review process is embedded into clinical practice through the electronic patient record (EPR).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of financial support for research, authorship, and publication of this article from EMAHSN.