
Abstract
The goal of this study was to explore the weight management experiences of Baby Boomer men (born between 1946 and 1964) and to use the information to develop targeted messages and interventions. Twenty men were interviewed. The Health Belief Model was used as the study’s theoretical framework. Men correctly identified health risks of being obese. However, most believed that body mass index and weight charts were unrealistic, and a few felt that they would be too “skinny” at the recommended weight. Wives were sources of nutrition information and social support. Perceived benefits of losing weight included reduced risk for health problems and looking good. Perceived barriers included apathy and weight loss programs being “too feminine.” Motivators for losing weight included being diagnosed with a health problem, health requirements for work, and financial incentives. The data themes suggest ways to develop male-specific messages and interventions that consider the aging body.
Introduction
Americans 50 years and older will represent 45% of the total population by 2015. This growth is fueled by Baby Boomers who were born between 1946 and 1964 (U.S. Census Bureau, 2009). As Baby Boomers age, they are developing obesity, heart disease, diabetes, and other chronic diseases earlier than previous generations (Crystal & Siegel, 2009; Shoob, Croft, & Labarthe, 2007). By 2030, 25% will have diabetes, 50% will have arthritis, and 33% will be classified as obese (American Hospital Association, 2007). Among Baby Boomer men, there has been a 29% increase in obesity prevalence in every decade since 1950 (Flegal, Carroll, Ogden, & Curtin, 2010; Parikh et al., 2007).
Currently, 36% of men 60 years and older and 37% of men 40 to 59 years old are obese compared with 32% of men 20 to 39 years old (Ogden, Carroll, Kit, & Flegal, 2012). While men report less body dissatisfaction than women (Frederick, Forbes, Grigorian, & Jarcho, 2007; Muenning, Haomiao, Lee, & Lubetkin, 2008; Ogden & Taylor, 2000; Reboussin et al., 2000; Yates, Edman, & Aruguete, 2004), men still report unhappiness with their weight and a desire to lose weight (Kuk et al., 2009; Muenning et al., 2008; O’Brien et al., 2007). Despite wanting to lose weight, men are less likely than women to participate in group and individual weight loss programs (Patrick, Calfas, & Norman, 2011).
As men get older, they start to appreciate their health more and become willing to assume more responsibility for their health (Calasanti, Pietilä, Ojala, & King, 2013). Previous literature conducted outside of the United States has identified motivators and barriers men have toward weight loss (De Souza & Ciclitira, 2005; Sabinsky, Toft, Raben, & Holm, 2007); however, few studies have focused on weight management issues among older men and none have identified key factors for developing programs and interventions for them. Moreover, in the past 10 years participation in weight loss research has predominately focused on females, with only 22% of participants in U.S. studies being men (Pagoto et al., 2012). The goal of this study was to explore the weight management experiences of Baby Boomer men and to use the information to develop targeted programs and messages for them. The Health Belief Model (HBM) was used for this study as it is one of the most popular planning models and helps explain how individuals conceptualize risk and why they change or maintain specific health behaviors (Hochbaum, Kegels, & Rosenstock, 1952). HBM can also provide direction at the micro level for developing materials and intervention strategies for weight management (Daddario, 2007; James, Pobee, Brown, Oxidine, & Joshi, 2012; Lambert et al., 2005).
Method
Participants
This qualitative study used semistructured interviews with 20 Baby Boomer men. The men were recruited from a convenience sample of 211 Baby Boomer men who were surveyed about their weight management strategies and previous participation in weight management programs. Men were recruited from sporting events, civic organizations, and two worksites. Survey participants were asked if they would be willing to participate in a semistructured interview. Those who agreed were debriefed on the audio recording procedures and consent was obtained. Interviews were conducted until the researcher determined a point of data saturation. The men ranged in age from 45 to 63 years, with a mean age of 53 years (SD = 5.50) and a mean body mass index (BMI) of 27.38 (SD = 4.97). None of the men were classified as underweight. Six were at a normal weight with a mean BMI of 23.31 (SD = 0.99) and had a mean age of 53 years (SD = 5.58). Twelve were classified as overweight with a mean BMI of 27.32 (SD = 1.39) and had a mean age of 54 years (SD = 5.60). Finally, two were classified as obese with a mean BMI of 40.02 (SD = 7.09) and had a mean age of 48 years (SD = 0.71). See Table 1 for other demographic information.
Demographic Characteristics of 20 Baby Boomer Men Interviewed About Their Weight Management Experiences.

Procedure
The study was approved by the institutional review board at the researchers’ institution. Interviewees completed a brief survey that included demographic data and self-reported height and weight. Self-reports are commonly used measurements for collecting data on height and weight and are good methods for quickly collecting data for descriptive studies and cross-sectional surveys (Gorber, Tremblay, Moher, & Gorber, 2007). The lead author conducted the interviews and took field notes to later compare with transcripts to ensure proper context was captured. The topics covered were perception of a healthy weight, overweight, and obesity; dieting and weight management experiences; barriers and motivators to weight loss; and information needed to achieve or maintain a healthy weight (Figure 1). The interviews were audiotaped and lasted about 60 minutes. Each participant received a $20 gift card.

Interview questions for Baby Boomer men about their weight management experiences.
Data Analysis
A primary coder and two secondary coders coded each transcript. Coders conducted in-depth reviews and re-reviews of the transcripts based on established themes from the codebook. The statements provided by participants were then grouped according to similarity and frequency. Each coder noted those themes that occurred most often. They also made annotated comments on the transcripts for discussion in team meetings. Several team meetings were used to discuss areas of agreement and disagreement with the themes until consensus was reached (Hill, Thompson, & Williams, 1997). Select verbatim quotes that captured participants’ sentiments, views, and opinions are included in the text.
Results
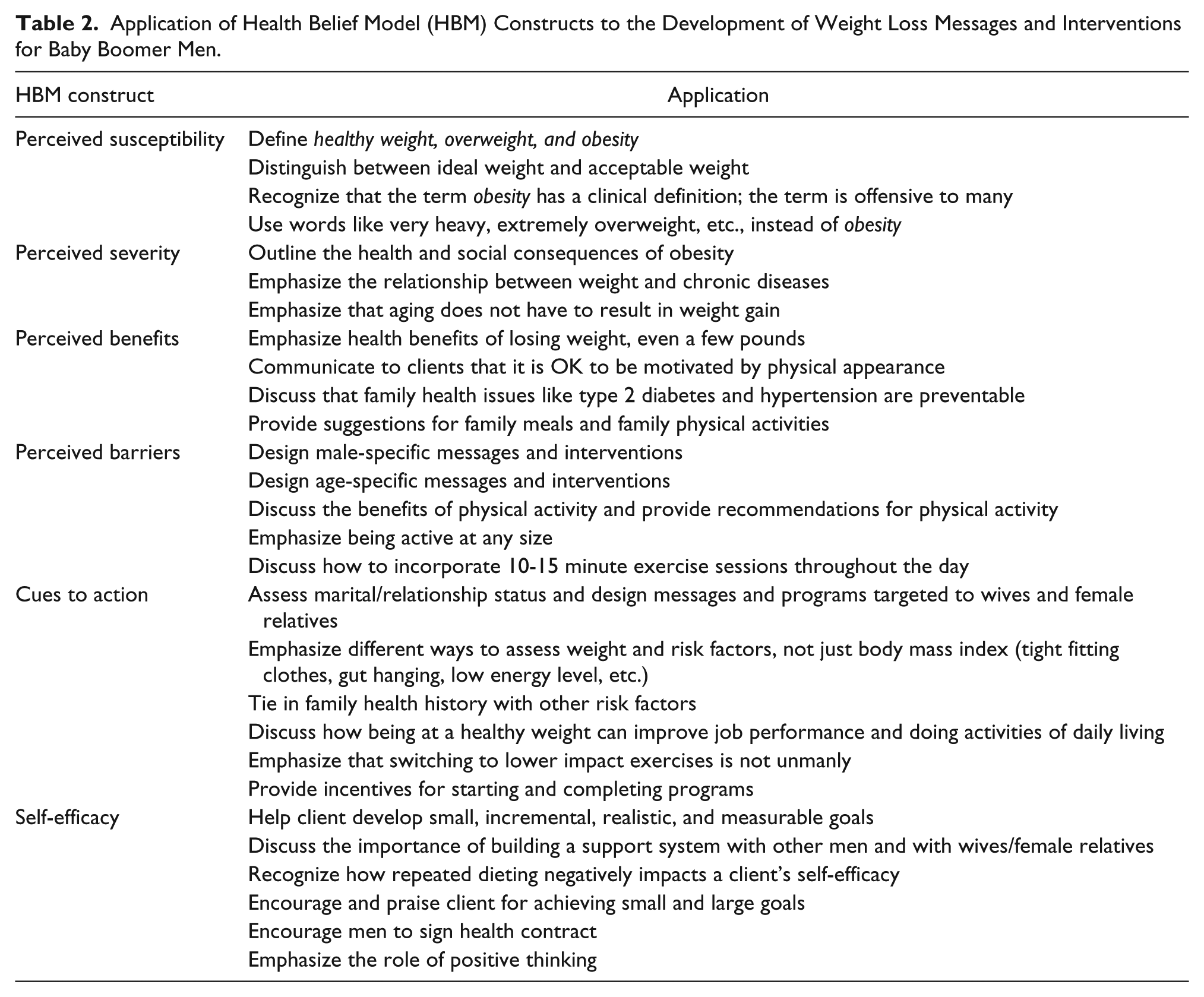
HBM contains six constructs: perceived susceptibility, perceived severity/seriousness, perceived benefits, perceived barriers, cues to action, and self-efficacy (Bandura, 1982; Champion & Celette, 2008; Rosenstock, Strecher, & Becker, 1988). These constructs were applied to the agreed upon themes. Quotes that best reflected the participants’ beliefs, attitudes, and experiences were pulled out and described under each HBM construct. Data themes were organized in a framework matrix around the constructs in Table 2.
Application of Health Belief Model (HBM) Constructs to the Development of Weight Loss Messages and Interventions for Baby Boomer Men.
Perceived Susceptibility to Obesity and Related Illnesses
Baby Boomer men’s perception of their susceptibility to becoming obese or developing related illnesses affects their likelihood of taking action. In addition, it is important to understand how they perceive concepts such as “healthy weight,” “overweight,” and “obesity.”
Weight Categories Are Different
The men made clear delineations between weight categories. Being at a “healthy weight” was defined as “liking what you see in the mirror,” “when your jeans are not tight,” and “being able to do your daily functions.” “Overweight” was considered to be “just a few pounds over your ideal,” “being a little chunky,” and “the point when your gut begins to hang.” “I can feel if I am heavier. I just move differently.” Obesity was seen as being “extreme,” “gross,” and “out of control.”
Weight Charts Are Unrealistic
Several men emphatically stated the weight recommended by their physicians was unrealistic and insisted they knew what weight was right for them. “The weight they say is right for me just doesn’t feel good on me.” “I feel like I’d be too skinny at that weight.” “I was startled when they told me I was obese because I think I look good in the mirror.”
Marriage Results in Weight Gain
Wives were frequently mentioned in the interviews. Marriage, not wives, was seen as the contributor. “When I got married, I was 145 and then I got to 160 and stayed there for years. Now, I am 190. She’s packed it on too” [chuckles].
Perceived Severity of Obesity
It is important to understand how seriously men view the health and social consequences of obesity. Men who perceive the threat to be serious are often aware of the signs, symptoms, and limitations of obesity and may be more inclined to try to get their weight under control.
Risk for Diseases
Obesity was said to increase risk for diabetes, hypertension, and heart disease. “I have diabetes because I’m too heavy. I think I can to get off insulin if I lose some weight.” “My blood pressure comes down when I’m at a good weight, but that’s been a while.”
Older Bodies
Aging and weight gained combined to restrict activity. “It’s just harder to take the pounds off and get enough exercise as you get older.” “As I’ve gotten older, I’ve put on more weight and can’t exercise as much.” Some adapted by switching to different activities. “I used to run regularly when I was in better shape, but now I pretty much do the bike at the gym.” “Swimming is easy on my joints. I can swim intervals to make my workout harder or I can swim the same number of lengths at a leisurely pace and it’s just refreshing.”
Perceived Benefits to Losing Weight
The health and social benefits of losing weight can be strong motivators to change eating habits, physical activity levels, and responses to environmental influences. Many men personalized the benefits of losing weight.
Looking Good
Several wanted to get in shape to “look good.” “I was going to a wedding and I wanted to look really good.” “We took pictures and I was shocked when I saw my stomach in the picture. That picture was my motivator to lose weight. It went up on the refrigerator as a reminder.”
Health Reasons
Having a family member who was either diagnosed with a health problem or died early were indicators to manage their weight. “Coronary artery disease and cancer run in my family. Both of my parents were overweight.” “My dad passed away at 65 and my uncle at 48. I really need to change something here, like stop smoking the cigarettes and losing some of this weight. I mean I can help myself.”
Perceived Barriers to Weight Loss
Negative beliefs, external circumstances, and real and imagined costs often prevent men from trying to lose weight. They may understand the benefits of weight loss, but time constraints, lack of motivation, and lack of male-specific programs often prevent them from taking action.
Time Constraints
Lacking time to exercise was the most cited barrier. “Trying to maintain a weekly exercise schedule is the hardest thing for me.” “I work long hours and I just don’t make time to exercise.”
Apathy and Lack of Motivation
Several overweight men said they had no concerns about their weight. “If you aren’t sick, why worry about it?” “I would say that I’m a little overweight, but getting in shape is just not a big concern.” Not being told to lose weight by a physician also contributes to the lack of concern. “My physician hasn’t said anything so I’m not worried about it.” The men often lacked motivation to take action. “I am just lazy and don’t want to make the effort.” “I’m not doing the things I need to do and I feel bad about it. I mean, it’s not because I have a bum knee, it’s just that I can’t get motivated.”
Diets Are Unrealistic
Men understood the importance of dieting in order to lose weight but felt that eating the foods necessary to lose weight would not be maintainable. “I’ve seen people on diets and I’m not saying that there’s not one that might not work, but it just seems really hard and it seems like you’re kind of always depriving yourself.” “I constantly fail at eating my veggies. What is it now 5-9 servings a day? I don’t even know what it is.”
Programs Too Feminine
Most would not join a weight loss program because they were “too feminine” and “not targeted to men.” “The attraction isn’t there, the atmosphere is too social.” “I’m not going to sit around and talk about my feelings.” They also said the programs do not work. “Those programs take your money and have a high failure rate.” “I’m not going to spend money for them to tell me what I already know.”
Cues to Action
Men are motivated to manage their weight for internal and external reasons. For some, one cue may be enough to motivate them to lose weight, but for others a series of cues may be needed.
Wives
Several husbands stated that their wives had direct and indirect ways to get them to do something about their weight. “If my pants get tight then I have a decision to make because my wife won’t buy me bigger pants. So, that’s my motivation to stay in a certain zone.” “She signed me up for one of those programs, but I didn’t put in much effort.” Wives also provided nutrition information and support. “We decided to lose weight together.”
Weight Goals
Most men had a preferred weight and some monitored it regularly. “I am 198 and I refuse to go over 200.” “My goal is to get my waist equal to or smaller than my inseam.” Several monitored their pant sizes rather than their weight. “I wear a size 34 and I would like to wear a 32. I used to wear a 36 but I don’t want to go back there.” One man stated, “I’ve got boxes of what I call my fat pants and my skinny pants.”
Health Problems
Being diagnosed with a health problem was as a significant motivator. “I changed my diet because I have diabetes and hypertension.” “I knew I had problems, but did nothing until the doctor told me I had to do something about my weight.” The health problem had to be “serious” before action was taken.
Work Requirement and Everyday Tasks
Certain occupations required the men to be fit. “The Navy has weight requirements that force me to stay in shape.” “I was doing a roofing job and I couldn’t get on my knees. That’s when I said ‘OK,’ I need to do something about my weight.” Having difficulties with everyday tasks were another cue. “When you’re having problems climbing stairs and getting out of breath, then you know you need to do something.”
Financial Incentives
Financial incentives can also be motivators. “I joined a program to get my diabetes meter and test strips for free. So, I go to monthly meetings and work on my weight to get the stuff for free.” It was also suggested that a monetary incentive for meeting weight standards would appeal to men, especially at worksites. “Many men would do it if you paid them.” “You could give them a tax credit for meet a certain weight or skinfold pinch test.”
Self-Efficacy
Baby Boomer men with high self-efficacy are likely to take the necessary actions to manage their weight. A frustrated dieting experience, limited knowledge of basic nutrition, and a lack of social support appear to negatively affect the men’s self-efficacy.
Frustration
Several men were frustrated with dieting and may have felt that they were not capable of losing weight. “I’ve tried everything. I’d like to lose 20 pounds, but 10 is probably more realistic. My doctor says I need to lose 30 [laughs].” “I can’t seem to get below 250 no matter how hard I try.”
Ongoing Battle
Weight loss was something that men described that they had tried multiple times or that they were repeatedly involved in some phase of weight loss. “I’m always trying but I never stick to it for [more than] a day or two. I just get busy.” “I go back and forth. Left to my own devices I’m a fat person.”
Need Basic Information
There was a lack of knowledge about what men needed to eat in order to efficiently lose weight. Information on portion sizes, reading food labels, and calorie recommendations were needed. “The other night my wife fried some chicken and made some beans and rice . . . my plate was full and about three inches high. We have no concept of what a healthy portion is.” “I would like food labels that are easier to read. We need to know the big things like fat and sodium content.”
Social Support
Most were not interested in joining a commercial weight loss program, but two said they would join if their wives went with them. “I would do something structured if my wife was doing it with me. We would hold each other accountable.” Others said exercising with male friends helped. “A few of us workout together a few times a week. It’s something to look forward to and we push each other.”
Discussion and Conclusions
Obesity among Baby Boomer men has increased over several decades. While only two (10%) of the Baby Boomer men in the study were obese, 12 (60%) were overweight and at risk for becoming obese. Thus, targeting overweight individuals at risk for obesity appears to be a viable strategy in combating obesity (U.S. Department of Health and Human Services [DHHS], 2010). The men’s narrative revealed a struggle between setting their personal weight goals, accepting the clinical definition of obesity, and being motivated to make significant changes to manage their weight and decrease health risks.
The decision to lose weight is influenced by personal weight perception (James et al., 2012; Miller et al., 2008). Several men believed BMI charts were unrealistic and, thus, self-diagnosed their weight status. Pants size was often used to assess weight status and to set goals. Clothing fit has been found to be an important weight-monitoring tool and can be used as a trigger to reverse small weight gains (Reyes et al., 2012). These issues suggest that Baby Boomer men need help in assessing their weight in the context of their health risks. Men may not clearly perceive what is considered to be an unhealthy weight and thus may not feel that they are susceptible to becoming obese. Providing BMI weight classification measures to this population will assist them with understanding the meaning of their weight status. In addition to using BMI, waist circumference and biochemical indicators can be used to assess their health risks (DHHS, 1998).
There is evidence to suggest that many primary care physicians are ill-prepared to manage obese clients and reluctant to diagnose and document their patients as “obese” (Bardia, Holtan, Slezak, & Thompson, 2007; Terre, Hunter, Poston, Haddock, & Stewart, 2007; Tsai & Wadden, 2009). As a result, obesity is more likely to be underdiagnosed and undertreated by physicians (Surgeon General, 2010). Thus, primary care physicians should be encouraged to refer their obese clients to registered dietitians, counselors, psychologists, and fitness professionals for additional services.
Overweight and obesity often lead to increased insulin resistance, blood lipids, blood pressure, and strain on aging joints (DHHS, 2010; Hu, 2008). The men accurately described the health risks of obesity and a few believed they could reduce or get off diabetes and hypertension medications if they lost weight. Weight also limited some of their activities of daily living as well as tasks on their jobs. Thus, it is important to emphasize the benefits of being at a healthy weight, or even losing just a few pounds (DHHS, 2010; Surgeon General, 2010). Tying these factors in with family histories may provide added motivation (James et al., 2012).
Regular physical activity is necessary for long-term weight management (DHHS, 2008). Studies show that men who combine exercise and dieting experience more cognitive restraint, reductions in hunger, and greater weight loss than those who only diet (Kiernan, King, Stefanick, & Killen, 2001). Fitness plans for Baby Boomer men should have realistic goals for an aging body, emphasize short intervals of activity for heavy men and those starting an exercise program, and include practical ways to fit activity in during the workday (DHHS, 2008; James, 2004; James et al., 2012; Jeffery, Wing, Sherwood, & Tate, 2003; Surgeon General, 2010). Exercising with male peers will also serve to encourage the initiation and sustainment of physical activity (Griffith, King, & Allen, 2013). Practitioners should also recommend switching to low-impact cardiovascular activities, adding weight training to maintain muscle mass and strengthen bones, and doing flexibility exercises to increase range of motion and decrease risk for injuries (DHHS, 2008).
The men reported significant weight gain during their marriage. Regardless of life stage, spouses significantly influence eating and physical activity habits (Dinour, Leung, Tripicchio, Khan, & Yeh, 2012). Furthermore, being married often results in weight gain (Dinour et al., 2012). This may occur because of increased opportunities for eating, larger portion sizes, decreased physical activity, and lack of motivation to maintain a healthy weight to attract a partner (Averett, Sikora, & Argys, 2008; The & Gordon-Larsen, 2009). Men often look to their wives for nutrition and health information and expect their wives to assume some responsibilities in managing their health (August, Rook, Stephens, & Franks, 2011; James, 2004, 2009; Meltzer, McNulty, & Karney, 2012). Because of their attentiveness to their husbands’ health, wives can play important roles in providing encouragements and creating environments that encourage healthy eating and promote physical activity (Allen, Griffith, & Gaines, 2012; James, 2004, 2009). Thus, practitioners should consider marital status when assessing Baby Boomer men’s food and physical activity habits and include wives and significant others when developing treatment plans.
Self-efficacy is essential to behavior change (Bandura, 1982) and is a strong predictor of weight management success (Gallager et al., 2012; Wingo et al., 2012). Practitioners can help foster self-efficacy in clients through praise and reinforcement for behavior changes (Bandura, 1982; Foreyt, 2005). Self-efficacy can also be improved by providing men with information on basic nutrition, portion sizes, food labels, and daily caloric needs. The men perceived most weight loss programs as too feminine, ineffective, and not tailored to their specific needs. Thus, there is a need for male-specific weight management programs that consider the aging male body. These tailored programs should also consider using financial incentives, personal health contracts, and couples-based activities.
Limitations
Few studies have examined the weight management needs of Baby Boomer men. The HBM provided a good fit for the data and it allowed the researchers to use the themes generated from each theoretical construct to develop weight management materials and messages for older adult men. One must remember that qualitative data are not generalizable to other groups. However, the exploratory nature of the interviews was a first step in understanding the beliefs, attitudes, experiences, and needs of the target group (Morse & Field, 1995; Weiss, 1994). The perspectives of the participants in this study are intended to help refine theory and develop weight management materials and interventions for Baby Boomer men. Our findings summarized the most prevalent themes. The men in this preliminary study were mainly White and well educated. Thus, future studies aimed at developing weight management materials and messages for Baby Boomer men need to include more men from different ethnic and socioeconomic backgrounds to give greater breadth and depth to the findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.