
Abstract
Introduction:
Dialogue Café, which is an inclusive process that provides a platform for the exchange of ideas or perspectives on certain issues, is a suitable approach to facilitating mutual understanding between health professionals and citizens/patients. However, little is known about the effects of the Dialogue Café on participants in the context of health communication. Previous studies suggest that transformative learning occurs after dialogue.
Objectives:
This study aimed to clarify the process of the transformative learning process among participants of the Dialog Café and to evaluate whether their transformative learning would lead to an understanding of others’ perspectives.
Methods:
We conducted a psychometric analysis of a web-based questionnaire consisting of 72 items for participants of Dialog Café held from 2011 to 2013 in Tokyo and studied the relationships between various concepts using structural equation modeling (SEM). To evaluate the validity and reliability of concept measurement, we conducted an exploratory factor analysis and a confirmatory factor analysis.
Results:
The questionnaire response rate was 39.5% (141/357), of which 80 (56.7%) respondents were health professionals and 61 (43.3%) respondents were citizens/patients. The SEM analysis revealed that transformative learning occurred in both groups. The process of transformative learning consisted of 2 types; one process leading directly to “perspective transformation” and the other leading to “perspective transformation” via “critical self-reflection” and “disorienting dilemmas.” “Perspective transformation” was related to “understanding others” in both groups. Among health professionals, “perspective transformation” was related to “transformation of awareness toward patients/users.”
Conclusion:
Dialog Café can facilitate the process of transformative learning among participants, and transformative learning may lead to mutual understanding between health professionals and citizens/patients.
Introduction
In recent years, communication methodology has been increasingly emphasized in the provision of optimal medical care and public health promotion. The various modes of communication between health professionals and citizens/patients are called “health communication.” 1 One of the definitions of health communication, the one proposed by the Centers for Disease Control and Prevention, is “the study and use of communication strategies to inform and influence individual decisions that enhance health.” 2 Although the term “health communication” is often used to refer to communication strategies in public health, it is also used to describe general communication activities among health professionals and citizens, including patients. 3
Many studies have explored factors influencing effective health communication, especially in the context of physician-patient communication. In physician-patient relationships, typical barriers include the knowledge gap or low health literacy,4-6 conflicts of different perspectives, 7 uncertainty, 8 and power imbalance.5,6,9-11 It is important to overcome those barriers not only in physician-patient communication but also in public health communication. Among several barriers, power imbalance seems critical in hampering effective health communication. One systematic review demonstrated that patients need both knowledge and power to participate in shared-decision making; thus, knowledge alone is not sufficient and power balance, despite being harder to achieve, is critical. 5
To overcome the power inequity and facilitate the sharing of perspectives between health professionals and citizens/patients in health communication, Dialog Café would be one of the required tools. 3 Dialog Café is an inclusive process that provides a platform for the exchange of ideas or perspectives on certain issues facing the community in question. 12 In Dialog Café, for example, World Café method, people sit at round tables in small groups, talking and listening to each other, sharing their various perspectives in a relaxed atmosphere. 12 During Dialog Café, mutuality and equality are embraced to share the ideas and experiences of various participants. 3 In the field of healthcare, several studies have reported that Dialog Café was useful in involving young people in mental well-being programs, 13 eliciting perspectives of young carers in the aspects of mental issues, 14 empowering nursery teachers to acquire competencies during their training, 15 or facilitating communication on death and dying among staff working for intellectually disabled people. 16
However, there are only a few studies that explored the learning process of participants of Dialogue Café in healthcare. Some studies suggest that awareness change or transformative learning may occur in the process of perspective exchange during dialogue.13,17-19 The theory of transformative learning was established by Mezirow and developed by other researchers in various fields.20-23 He describes the process of transformative learning as “disorienting dilemmas,” “critical self-reflection,” and “transformation of meaning perspective.” 20
According to his theory, transformative learning may occur when we face a life crisis or significant learning, which is referred to as “disorienting dilemmas.” This experience can be emotionally difficult and often leads to feelings of confusion, frustration, or discomfort. Disorienting dilemmas create a sense of cognitive dissonance, which prompts individuals to reassess their beliefs and values. This step is critical in creating the impetus for transformative learning. Disorienting dilemmas are experiences that illuminate and challenge heretofore invisible and unquestioned assumptions that determine how we know ourselves and the world around us. 24
The second step is “critical self-reflection,” which involves examining and analyzing the assumptions and beliefs that were challenged by the disorienting dilemmas. 25 Critical self-reflection allows individuals to question the validity of their previous assumptions and consider alternative perspectives. It is essential to engage in critical reflection in an open and honest way, without judgment or preconceived notions.
The final step is the “transformation of meaning perspective.” 25 This involves a fundamental shift in an individual’s worldview, which results in a new perspective that is more inclusive, integrated, and reflective. The transformation of meaning perspective results from the critical examination and reevaluation of assumptions and beliefs. This shift in perspective allows individuals to view the world and their place in it in a new way and to engage in new behaviors that are more aligned with their new worldview.
Mezirow 26 states that “perspective transformation is the process of becoming critically aware of how and why our presumptions have come to constrain the way we perceive, understand, and feel about our world; of formulating these assumptions to permit a more inclusive, discriminating, permeable, and integrative perspective; and of making decisions or otherwise acting upon these new understandings.” Nevertheless, it is unclear whether or not the process of transformative learning occurs in Dialog Café in health communication.
This study aims to explore the transformative learning process among participants of Dialog Café, and to investigate whether their transformative learning would lead to an understanding of others’ perspectives.
Method
This cross-sectional questionnaire-based study was conducted from October to December of 2013 to explore the learning process of participants of Dialog Café held in Tokyo during the past 3 years.
Dialog Café
The authors regularly held Dialogue Café called “Mincle-Café” (meaning “Café that everyone can join” in Japanese) since 2010. About 10 to 20 participants, including citizens/patients and health professionals, gathered at a Café in Tokyo and freely talked about themes focused on health-related issues. The dialogue sessions were facilitated according to the World Café method. World Café was started by Juanita Brown and David Isaacs in 1995 to activate conversations in business meetings. 12 Participants sit around several tables in small groups (usually 4-7 people per table), exchanging with each other on a topic with the help of a group facilitator, switching tables periodically. Individuals were encouraged to write down keywords on the table sheets. After a few sessions of dialogue, people returned to the original table and reflected on what they learned during the conversation.
Mincle-Café usually starts with a guest speaker’s short speech on a certain topic to share basic information before dialog sessions begin. The guest speaker could be a specialist or someone who has specific experience in the domain of interest. The typical topics of Mincle-Café were: end-of-life care, ending notes (advance directive), home care, life and death, physician-patient communication, and so on.
Participants and Design
A total of 357 participants of Dialog Café held in Tokyo from August 2010 to September 2013 were invited to take part in the study. Each participant received an email of invitation, which included information on the study and the URL link to a web-based questionnaire. Invited participants consisted of health professionals and citizens, including patients. Detailed information about the study was available in the body of the email and on the cover page of the web-based questionnaire. Only those who agreed to participate in the study went on to answer the questionnaire. The web-based questionnaire was designed such that participants could suspend answering at any time until they pressed the “finish” button on the last page. Data collection was completed between October and November of 2013. Because the Dialog Café was held 5 to 6 times during the year, some Dialog Café participants attended more than 1 event, so the number of times an individual participated ranged from 1 to 5 or more. However, all responded to the questionnaire only once.
Materials and Procedure
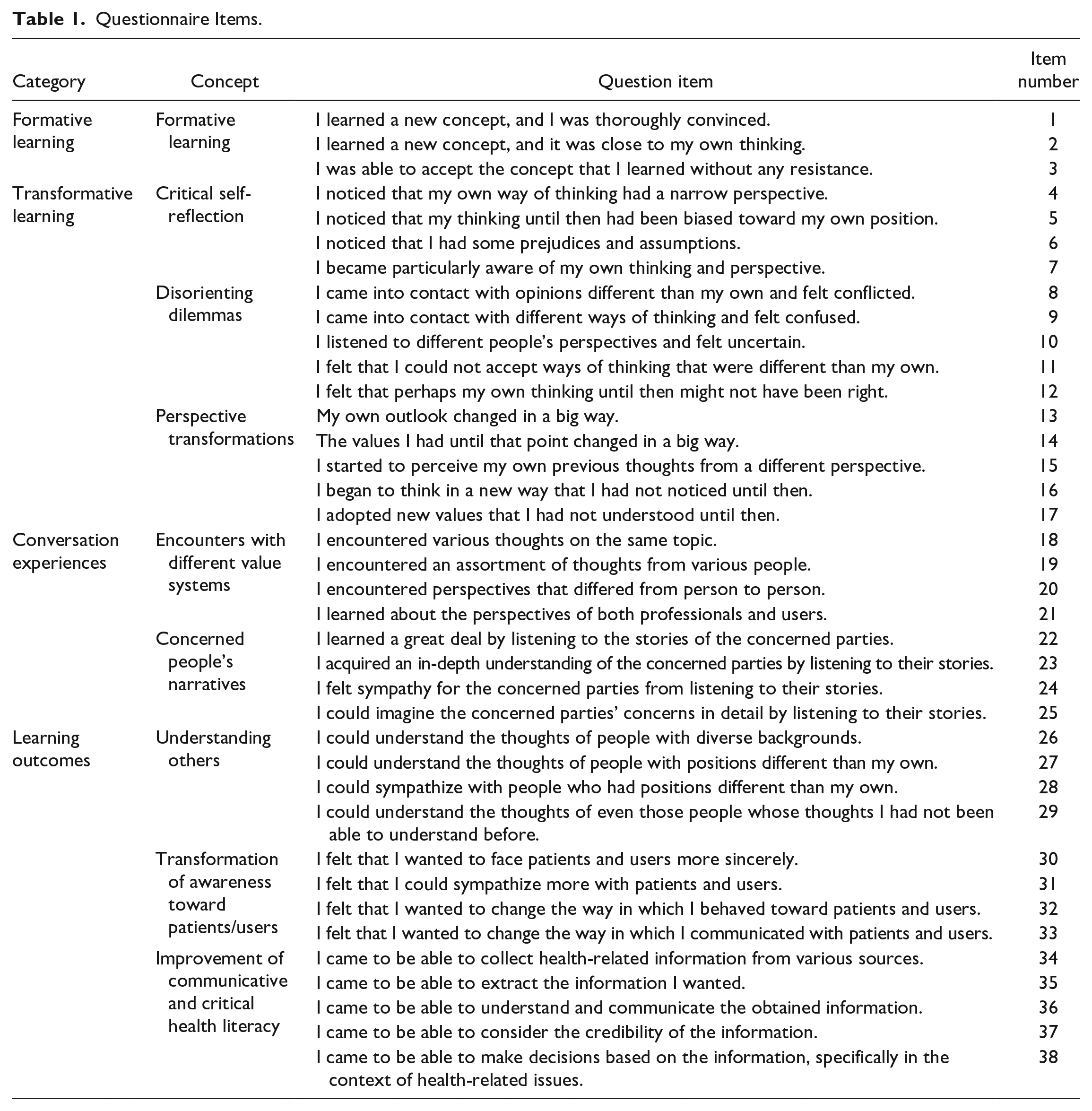
We developed a web-based questionnaire consisting of 38 items (5-point Likert scale) including items that assessed several concepts regarding the transformative learning process and its related outcomes (Table 1). The questionnaire items were mainly developed by the authors based on the findings of previous qualitative research clarifying the transformative learning of Dialog Café participants. 19 The items related to transformative learning were “disorienting dilemmas” (5 items), “critical self-reflection” (4 items), and “perspective transformation” (5 items), according to the transformative learning theory postulated by Mezirow. We also developed items that assess the concept of “formative learning” (3 items). Mezirow defines “formative learning” as pedagogical learning in which people passively learn without criticizing, which contrasts with “transformative learning.” 20 Based on Dialog Café experiences, items were developed on the concepts of “encounter with different value systems” (4 items) and “concerned people’s narratives” (4 items). As learning outcomes, items were developed on the concepts of “understanding others” (4 items) and “transformation of awareness toward patients/users” (4 items). We also developed “improvement in the communicative and critical health literacy scale” to measure the perceived change in communicative and critical health literacy. The original “communicative and critical health literacy scale” consists of 5 items, each to be rated on a 5-point Likert scale. 27 As we were interested in the perceived change in those concepts after participating in Dialog Café, all the items were formulated in sentences written in the past tense.
Questionnaire Items.
A theoretical path diagram of the learning process in a Dialog Café is shown in Figure 1. The first step in the Dialog Café was “encounters with the different value systems” and “concerned peoples’ narratives.” Next, “formative learning” and “transformative learning” (“disorienting dilemmas,” “critical self-reflection,” and “perspective transformation”) were identified as the learning processes. As outcomes of the learning process, we set “understanding others” and “improvement of health literacy” (for citizens/patients) or “transformation of awareness toward patients, users” (for health professionals).

Theoretical path diagram of learning process in Dialog Café.
Data Analysis
Participants’ responses were coded and entered into SPSS 22. Missing demographic data were excluded from the relevant analyses. We replaced the scale items of missing data with their respective mean values. Out of 142 participants, only 1 respondent answered no item; thus, this case was excluded from subsequent analyses.
As we were mainly interested in the process of transformative learning, we conducted exploratory factor analysis and confirmatory factor analysis (CFA) to explore and validate the conceptual structure of the latent variables of transformative learning and formative learning. A Cronbach’s alpha of >.70 is considered an acceptable reliability coefficient for determining the internal consistency of the scale.
To evaluate the relationships between several concepts, structural equation modeling (SEM) was performed using AMOS 22. The SEM analysis was modeled on the path diagram shown in Figure 1.
Ethical Considerations
To protect the privacy and personal information, the web survey was rendered anonymous. The request for research cooperation was indicated on the cover page of the web survey. Even if consent was obtained, we guaranteed in writing that participation in this study was based on free will and that responses were voluntary. This study was conducted after approval by the St. Luke College of Nursing’s Research Ethics Review Committee (Approval No. 13-058).
Results
Demographic Characteristics of the Participants
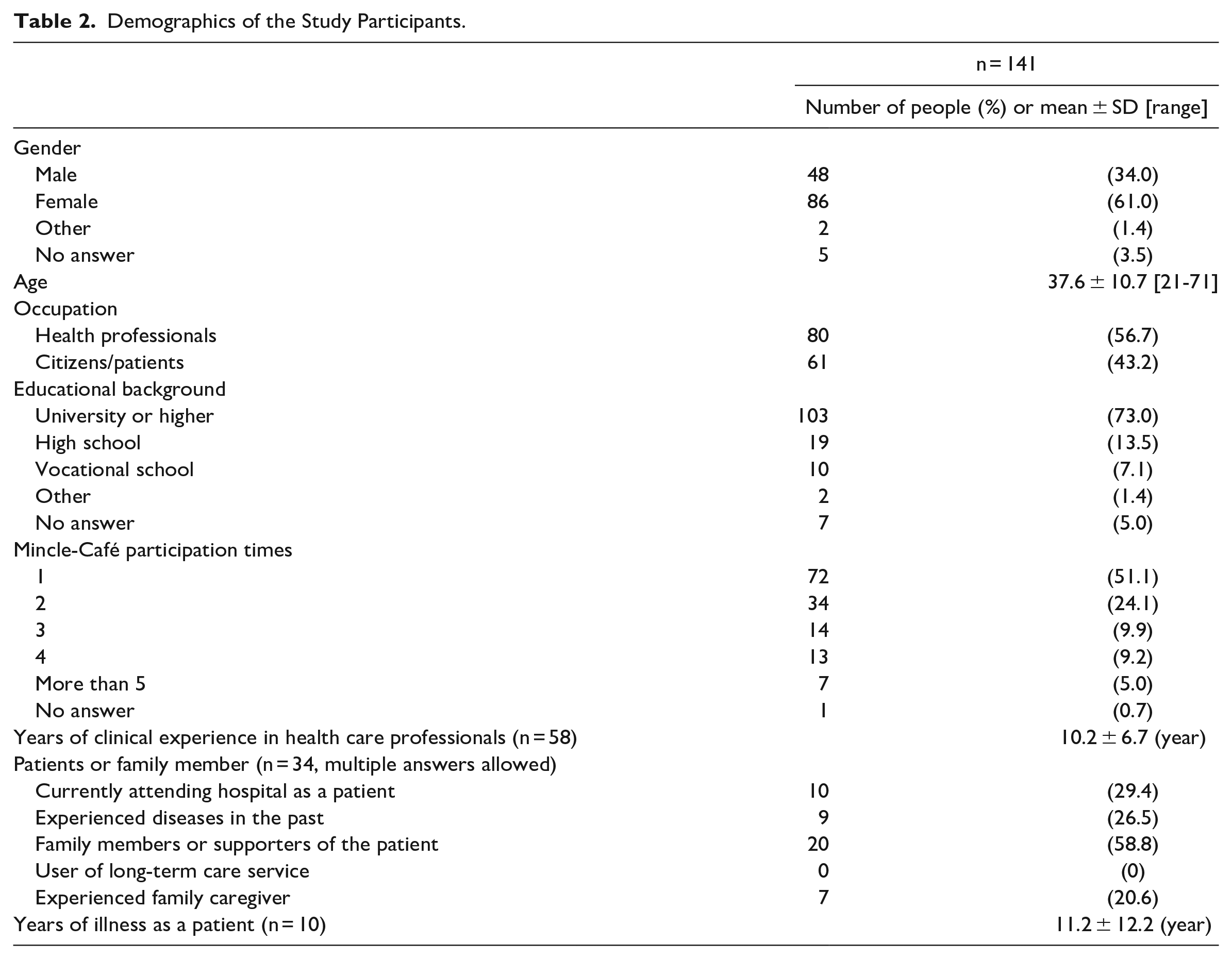
The questionnaire-based survey was conducted using a web questionnaire. Responses were solicited from 357 past participants of the Mincle-Café, and 142 people responded (response rate: 39.8%). The number of valid responses was 141 (valid response rate 39.5%). The demographics of the study participants are shown in Table 2. The male-to-female ratio was 1:1.79. The ages of our study participants ranged from 21 to 71 years, with a mean value of 37.6 years. There were 80 healthcare professionals (56.7%) and 61 citizens/patients (43.3%).
Demographics of the Study Participants.
Validating Concepts Related to Transformative Learning
Exploratory factor analysis (principal factor method, Promax rotation) was conducted on a total of 17 items, including 14 questions on transformative learning and 3 questions on formative learning, to verify the validity of the concepts of “critical self-reflection,” “disorienting dilemmas,” and “perspective transformation,” which are components of transformative learning, and “formative learning,” which is a counter-concept of transformative learning.
First, a principal component analysis was conducted, and the initial eigenvalues were 5.697, 2.931, 1.694, 1.189, and 0.888. Assuming a 4-factor structure according to the hypothesis, a factor analysis was conducted using the principal factor method and Promax rotation, and the results of this analysis are presented in Table 3. We decided to exclude items 7 and 12 because they did significantly influence any of the factors. The phrasing of items 13 and 14 were similar, with a correlation analysis showing a correlation coefficient of .83; thus we decided to exclude one of them. In the 5 question items of factor 1, the reliability coefficient α excluding item 13 was .842, and the α excluding item 14 was .843; so, we decided to exclude the latter.
Exploratory Factor Analysis for Transformative and Formative Learning.

Factor loadings > 0.45 are indicated by bold numbers.
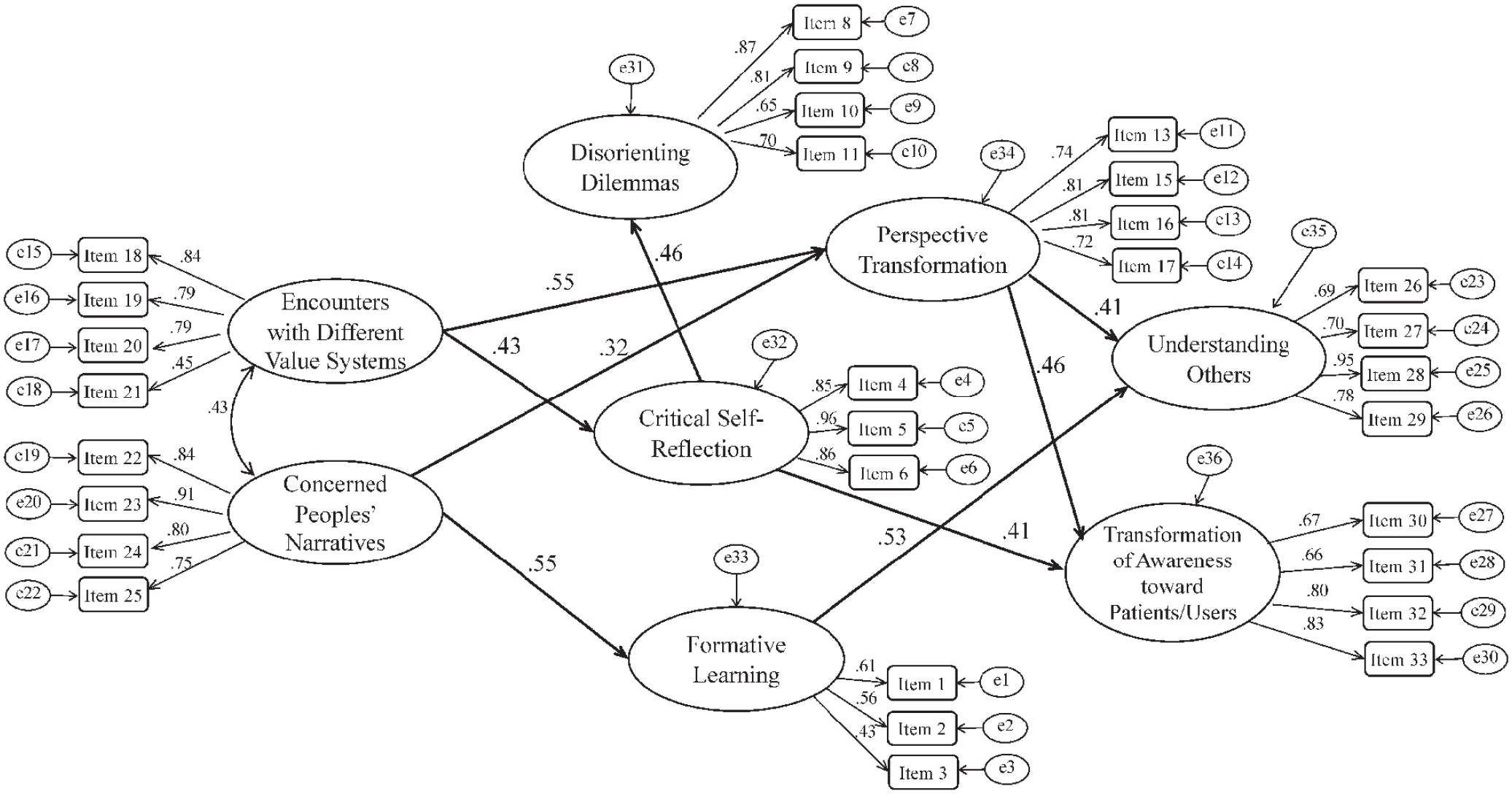
A CFA was conducted on the 14 items excluding the 3 abovementioned items (items 7, 12, 14), assuming a 4-factor structure (Figure 2). The goodness-of-fit indices were generally good, with GFI = 0.885, CFI = 0.926, and RMSEA = 0.084.

Confirmatory factor analysis of transformative and formative learning.
The Process of Transformative Learning in Citizens/Patients
The process of transformative learning in citizens/patients was subjected to SEM analysis (Figure 3). The goodness-of-fit indices were moderate, with GFI = 0.648, CFI = 0.845, and RMSEA = 0.088. For simplicity, paths and path coefficients are shown, leaving out only those that differed significantly at the 5% significance level.

SEM analysis of the process of transformative learning in citizens/patients.
For citizens/patients, the transformative learning process of participating in Dialog Café suggested that “encounters with different value systems” lead to “critical self-reflection,” followed by “disorienting dilemmas,” and then “perspective transformation.” We also found that “perspective transformation” could be achieved by listening to the “concerned people’s narratives.” Listening to the “concerned people’s narratives” also led to “formative learning.” As for the outcomes of the learning process, it was found that “understanding others” was enhanced through “perspective transformation” and “formative learning,” and that “improvement of health literacy” was achieved through “formative learning.”
The Process of Transformative Learning in Health Professionals
The process of transformative learning in health professions was similarly subjected to the SEM analysis (Figure 4). The goodness-of-fit indices were moderate, with GFI = 0.673, CFI = 0.826, and RMSEA = 0.092. Similarly, for simplicity, only paths and path coefficients for which significant differences were found at the 5% significance level were retained.
SEM analysis of the process of transformative learning in health professionals.
Among healthcare professionals, the process of transformative learning via participation in Dialog Café was “critical self-reflection” and “perspective transformation” occurring through “encounters with different value systems.” In addition, “critical self-reflection” caused “disorienting dilemmas.” Listening to the “concerned people’s narratives” led to “perspective transformation” and “formative learning.” As for learning outcomes, “perspective transformation” led to “understanding others” and “transformation of awareness toward patients/users.” “Critical self-reflection” also caused “transformation of awareness toward patients/users.”
Discussion
This study revealed the following of learning and its consequences among health professionals and citizens/patients who participated in the Dialog Café. First, transformative learning occurs through encountering people with different values and listening to participants’ narratives, a process that includes steps such as critical self-reflection and disorienting dilemmas. Second, transformative learning results in changes in understanding of others and in professionals’ attitudes toward patients/users, and in citizens/patients, health literacy is enhanced primarily through formative learning.
The learning process of awareness transformation is described by Cranton 23 as beginning with disorienting dilemmas that question the learner’s basic assumptions and values, followed by critical self-reflection, and then perspective transformation. According to many previous studies,24,28,29 on transformative learning, disorienting dilemmas is the starting point, followed by critical self-reflection that questions one’s assumptions. However, some researchers have shown that the trigger for transformative learning need not necessarily be disorienting dilemmas but can begin unnoticed, incidentally, and sometimes even casually, when a new practice is added to old habits,30,31 In the present study, it is possible that encounters with different values may have prompted critical reflection before triggering the dilemmas.
While critical self-reflection and disorienting dilemma are expected to occur in a relatively short period, perspective transformation is considered to be a process that occurs over a longer period. 23 The timing of the survey in this study ranged from a few months to a few years after participation in Dialog Café, which may have allowed us to assess the transformative process that occurred over a period after participation.
Formative learning is defined as pedagogical learning that people passively engage in without criticizing, which is contrasted with transformative learning. 20 In our analysis, significant paths to formative learning were found only from concerned people’s narratives, and significant paths to critical self-reflection and perspective transformation were found from encounters with different value systems. This means that critical self-reflection and perspective transformation, which are steps in transformative learning, are more likely to be triggered by dialog with people with different values. Also, formative learning is more likely to occur through listening to the narratives of others, which does not necessarily involve the transformative learning step.
This study suggested that health professionals and citizens/patients participating in Dialogue Café may develop an understanding of others’ perspectives through the process of transformative learning, leading to mutual understanding. Similar activities such as health cafés and dementia cafés have been held around the world, and their effects have been shown to be the improvement of health awareness and possible changes in cognition and behavior, in addition to social support.32-37 In Japan, health cafés organized by primary care physicians have been shown to complement primary care outpatient services. 38 The novelty of this study is that the transformative learning process was shown to be involved as a learning mechanism that leads to cognitive and behavioral changes in participants of dialogue activities.
There are several limitations to this study. First, because this study is a cross-sectional survey, the causal orientation in the SEM analysis is mathematically inferred in the model, unlike the changes observed in longitudinal surveys or other types of studies. Second, the population targeted in this study was made of people who voluntarily participated in Dialog Café, and there is a possibility of bias in the readiness of the change in consciousness. Third, some of the participants were surveyed long after their participation in Dialog Café, and there is the possibility of existent recall bias. Fourth, we did not measure the time between participation in the Dialog Café and participation in the survey and thus could not include this time as a covariate in our analysis. Finally, the reason it took so long to publish after the data collection was completed is not only due to the complexity of the model analysis, but also because more evidence on Dialog Cafés has accumulated in recent years and the academic position of this study has finally been established.
The current study is the first to identify the process of transformative learning between citizens/patients and health professionals in Dialogue Café. This study suggests the usefulness of incorporating dialogue and the resulting transformative learning into the design as a form of health communication between health professionals and citizens/patients. Rather than health communication as one-way health education from health professionals to citizens/patients, the dialogue model allows professionals to learn from citizens/patients while improving the health literacy of citizens/patients. We believe that health professionals and citizens/patients can deepen mutual understanding and learn from each other on socially important issues in the form of Dialogue Café.
Footnotes
Acknowledgements
We would like to thank all the study participants for their willingness to cooperate with us in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by JSPS KAKENHI Grant Number JP 25560348.