
Abstract
The objective of this scoping review was to describe the extent and type of evidence related to seeking help for tinnitus and satisfaction with healthcare providers including diagnosis, services and treatments along the clinical pathway. The selection criteria were adults aged 18 and over with tinnitus who sought help and where patient satisfaction with healthcare providers was reported. Online databases MEDLINE (OvidSP), Embase (OvidSP), PsycINFO (OvidSP) and CINAHL plus (EBSCO) were searched for original studies in English. The search had no date limit. Twenty-one records were eligible for data extraction. Studies reported that the most common healthcare providers seen were general practitioners, ear, nose and throat specialists and audiologists. Depression and tinnitus severity were related to an increase in the number of times help was sought and the type of healthcare provider seen may also impact patient satisfaction. The majority of participants were unlikely to receive a referral to a specialist at the initial GP consultation. Although there is limited research in this area, help-seekers for tinnitus were generally dissatisfied and reported negative interactions with healthcare providers. However, once in a specialised tinnitus clinical setting, studies reported that most help-seekers were satisfied and had positive interactions with healthcare providers.
Introduction
Tinnitus is the sensation of noise perceived in one or both ears or inside the head where the sound has no external source, and reported as ringing, buzzing, humming, clicking or other sounds (Baguley et al., 2013; Baguley, 2002). Tinnitus can be temporary, acute or chronic, is often a symptom of an underlying medical condition, and can have a significant influence on the quality of life of those who are affected (Ahmad & Seidman, 2004; Baguley et al., 2013; Crummer & Hassan, 2004; Davis & Morgan, 2008; Han et al., 2009; Newman et al., 2011; Tunkel, et al., 2014). Tinnitus is defined as clinical when the sensation of noise lasts at least 5 minutes and occurs more often than once a week (Dauman & Tyler, 1992) and defined as chronic when experienced for at least three months (De Ridder et al., 2021). The most common form of reported tinnitus is subjective tinnitus (Baguley et al., 2013; Langguth et al., 2013). If the sound of tinnitus can be heard by others, it is known as objective tinnitus. Objective tinnitus is rare and may be vascular in origin (Baguley et al., 2013; Crummer & Hassan, 2004; Langguth et al., 2013). The experience of tinnitus is often described as heterogeneous and this can complicate assessment (Baguley et al., 2013). Clinical assessment requires investigation as to whether a hearing loss or other medical issue is contributing to the tinnitus as well as identification of any accompanying psychological symptoms to ascertain the appropriate treatment (Crummer & Hassan, 2004; Newman et al., 2011). These aspects may not be established at the initial consultation in which case referral to a specialist may be indicated (Crummer & Hassan, 2004). The prevalence of chronic tinnitus has been reported to be approximately 10–15% of the population and even higher for occasional tinnitus (22–32%) (Adrian, D & El Refaie, 2000). A systematic review of the prevalence of tinnitus shows that prevalence varies with age (18–44 years 9.7%, 45–64 years 13.7% and 65 and over 23.6%) and that globally there are approximately 740 million tinnitus-afflicted people, with over 120 million of these having severe tinnitus (Jarach et al., 2022). However, the number of people who seek help for tinnitus is much lower (Adams et al., 1999; Brown et al., 1990; Lee et al., 2018; Newall et al., 2001; Redmond, 2010).
Help-seeking can be defined as a problem-focused, planned behaviour involving an interpersonal interaction with a healthcare provider (Cornally & McCarthy, 2011). A help-seeker is someone who has identified a problem or need, believes that external intervention is required and actively seeks help (Cornally & McCarthy, 2011). Patient satisfaction can be assessed as a measure of the quality of services provided by healthcare providers, and can identify deficiencies and potential improvements (Goldstein et al., 2000; Verbeek, 2004). Although there is not a globally accepted practice for measurement of patient satisfaction, a study reviewing patient satisfaction research found that the strongest positive influences of patient satisfaction were the quality of healthcare provider’s interpersonal skills, their competence, the physical environment of the facility, accessibility, continuity of care, hospital characteristics and care outcomes (Batbaatar et al., 2017).
The low level of help-seeking for tinnitus may be because the tinnitus is not bothersome or problematic enough to require seeking help. In a population study of middle-aged adults (n = 5107) of those who reported tinnitus (n = 1154, 22.6%), about a third (32.4%) reported that tinnitus had an occasional effect on daily life, whilst only a small number (8.9%) reported a frequent or constant effect on daily life (Stegeman et al., 2021). Research into patient care for tinnitus indicates that a low confidence in the ability to resolve or manage tinnitus may also prevent seeking help, (Smith & Fagelson, 2011) and factors such as confidence, knowledge, having a positive approach and support from a significant other may encourage help-seeking behaviour for tinnitus or a hearing issue (Meyer et al., 2014; Smith & Fagelson, 2011).
To understand what factors may motivate someone with tinnitus to seek help, studies comparing help-seekers with non-help-seekers provide some insight. Help-seekers are more likely to have significantly more combined tinnitus sounds, more non-fluctuating tinnitus and significantly higher psychological variables, concentration difficulties, irritability and sleep disturbances (Hallberg & Erlandsson, 1993). Help-seekers report more severe noise-induced hearing loss, more psychological symptoms and reduced coping with tinnitus, as well as significantly lower tolerance to noise, indicating a lack of inhabitation to the tinnitus noise (Attias et al., 1995). Help-seekers report a greater amount of somatic complaints including problems with sleep and concentration, and are also more likely to have higher levels of tinnitus-related distress (Scott & Lindberg, 2000). Help seekers more likely report hearing loss, hyperacusis and comorbidities such as dental problems, depression, balance problems or vertigo (Rademaker et al., 2021; Stegeman et al., 2021).
It has been acknowledged by both researchers and clinicians that health services for tinnitus requires significant improvement (Hoare & Hall, 2011; Langguth et al., 2011; Martinez et al., 2015; Searchfield, 2011). Tinnitus is like other ‘invisible’ chronic health issues such as back pain, insomnia and migraine (Benca, 2005; Bigal et al., 2008; Verbeek et al., 2004) in that they are self-reported. Dissatisfaction with the perceived lack of information has been consistently reported by those who experience these types of chronic conditions (Benca, 2005; Bigal et al., 2008; Verbeek et al., 2004). Tinnitus, in common with these other chronic health issues, is often associated with co-occurring health conditions and psychological symptoms, some of which compound the tinnitus or complicate treatment (Stegeman et al., 2021).
A better understanding of help seeking by those with tinnitus, and the satisfaction with services and treatment is required. A preliminary search of MEDLINE through the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis was conducted and no published or planned systematic reviews or scoping reviews on this topic were identified. The objective of this scoping review was to assess the extent of the literature on the nature of seeking help for the diagnosis and treatment of tinnitus, and the satisfaction with clinical services provided.
Method
This scoping review was based on the PRISMA-ScR extension for scoping reviews (Tricco et al., 2018). This is guided by the scoping review protocols by Arksey and O’Malley (Arksey & O'Malley, 2005) and Levac, Colquhoun, and O’Brien (Levac et al., 2010) which suggests following five stages (i) identifying the review question, (ii) identifying the relevant studies, (iii) study selection, (iv) charting the data, (v) collating, summarizing and reporting the results.
Stage I: Identifying the Question
The scoping review question was “what is known about seeking help for tinnitus and the satisfaction with healthcare providers, including diagnosis, clinical services, and treatment?” this question guided the analysis of the findings.
Stage II: Identifying the Relevant Studies
Eligibility Criteria
The inclusion criteria were original articles published in English that included adults aged 18 years and over (no upper age limit) with frequent or chronic tinnitus seeking help for tinnitus and the satisfaction with the clinical experience including diagnosis, clinical services, and treatment along the tinnitus clinical pathways in different settings and countries. The scoping review considered descriptive observational study designs, quantitative data and studies using qualitative data including grounded theory and interpretative phenomenological analysis. The search was not date limited.
Search Strategy
Online Database Search Strategy Example.
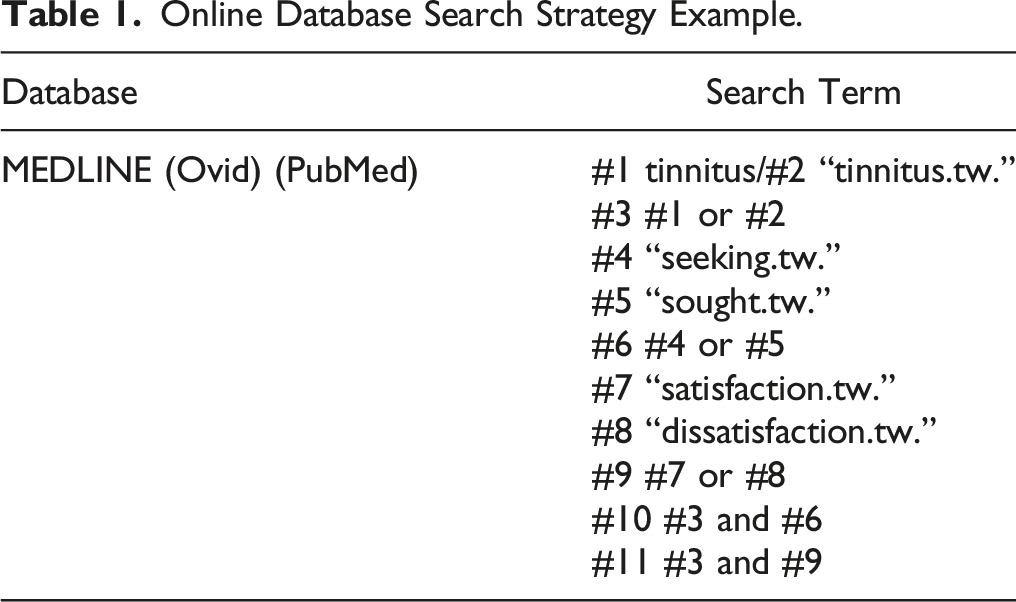
Finally the reference lists of all studies retrieved for critical evaluation for the review were searched for studies not yet identified and websites of relevant organisations were searched, or they were contacted to identify other public documents. The initial searches were conducted in September 2021. These searches were repeated in August 2022 to check for additional papers. A research librarian and the second reviewer (RE) checked over the final search terms used for the electronic searches. The second reviewer also checked over the online searches made whilst a third reviewer (STQ) tested the search strategy in online searches independent from the first reviewer, second reviewer and the research librarian. Any issues were resolved through discussion. (See Supplementary Table of full online database search strategy).
Stage III: Study Selection
Following the search, all identified citations were collated and uploaded by the first reviewer into the online for database Rayyan (Ouzzani et al., 2016) and the duplicates were removed. The titles and abstracts were screened with the blind on so that decisions and labels of any collaborator are not visible to others for assessment against the inclusion criteria. Any uncertain records were discussed with the second reviewer. Potentially relevant sources were retrieved in full and imported into the online database with the blind maintained. The third reviewer assessed the recovered records by the first reviewer uploaded into the online database against the inclusion criteria independently from the first and second reviewers. Any disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion. The results of the search and the study inclusion process are reported in full in this scoping review and presented in (PRISMA-ScR) flow diagram (Figure 1) (Liberati et al., 2009; Tricco et al., 2018). Flow diagram details search process and count of included and excluded records of each stage of the review.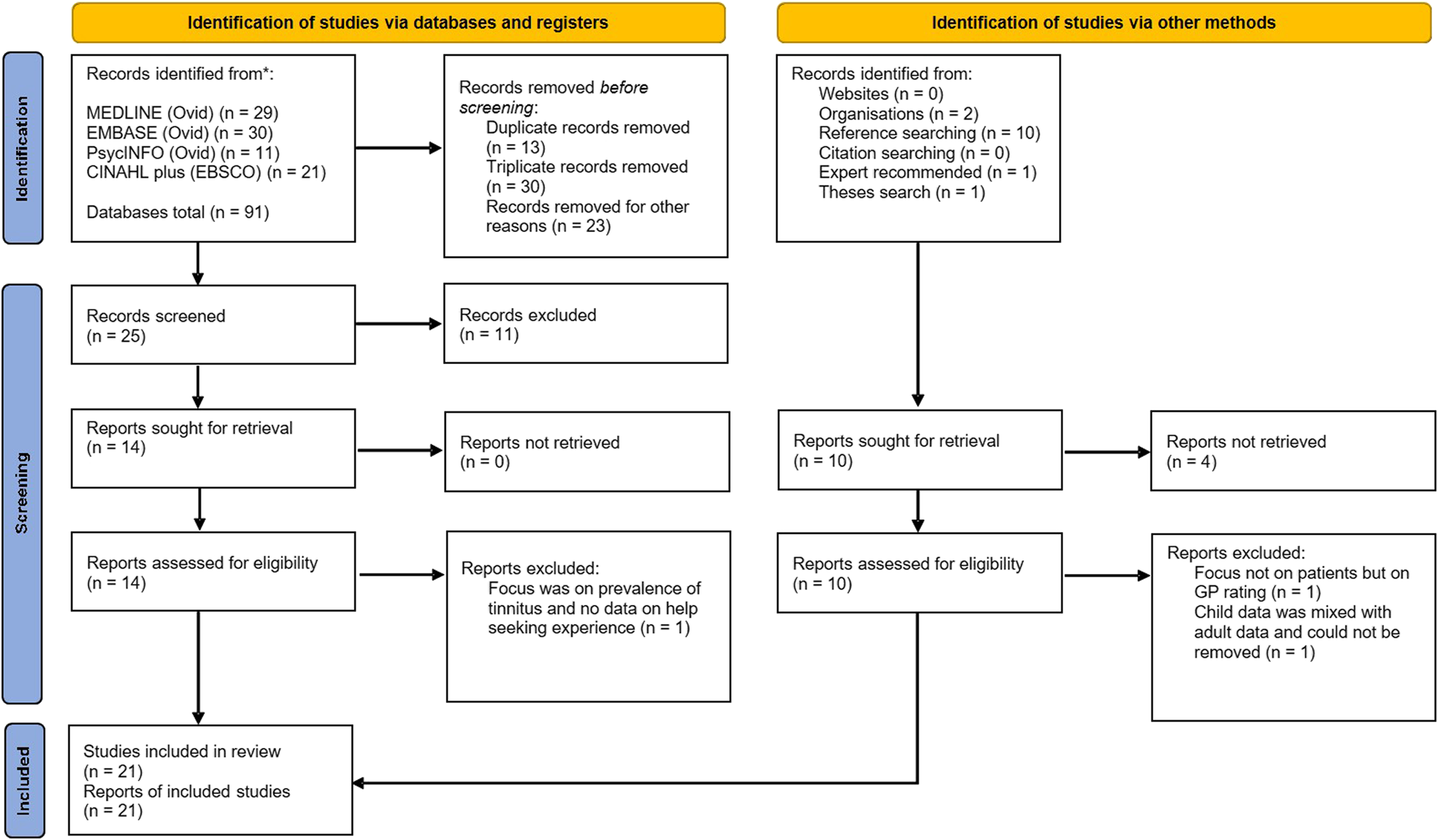
Stage IV: Charting the Data
The first reviewer extracted and tabulated all the data from each individual record and summarised the following characteristics, namely author(s)/year, study aim, title, study design, study setting (including country), study population and sample size. Another tabulation was created with further details such as presence of tinnitus and other characteristics, help-seeking and the health professional(s) seen, treatments, patient satisfaction (if reported). A short summary and key outcomes of each study were also included. The second reviewer checked the data in the tables. In the piloting process of data extracting it was decided that the studies would be sorted into categories of type of study sample reported in the study as the most suitable way to analyse and present the key findings. The third reviewer then performed an audit by selecting three of the included studies in the review to check the data extraction process by the first reviewer. Any issues with data extraction or errors were discussed. Any significant errors or disputes, this process was repeated with a different set of three papers until a decision was reached.
Stage V: Collating, Summarising and Reporting Results
The extracted data of the characteristics and key findings of the included studies were tabulated into four categories under type of study sample: population sample, self-selected sample, clinical/cohort sample, and interviews/qualitative sample. A narrative summary of the results was written to accompany the table which used descriptive statistics on the findings based on the categories above and including the table categories measures for help-seeking or patient satisfaction, help-seeking rate, health professional seen and satisfaction, treatment rate, health professional seen and treatment effectiveness/satisfaction. An overall summary of the results of the reviewed papers was based on the categories covered above.
Results
The number of records identified from the initial search of the databases was 91. After removing duplicates or triplicates and removing unsuitable records, 25 records were screened. From this screening, 14 records were sought for full text retrieval, and 13 records were selected to be included in the scoping review. After searching the references of the 13 retrieved records, 10 more records were identified. From searches of tinnitus and hearing organisations two records were identified and another record was identified by the research librarian. Of these, nine records were retrieved for screening and seven records were included in the scoping review. Further searches of reference lists in records already identified took place and any records deemed suitable were included for screening. A final search on Google Scholar for theses on the topic retrieved a Master’s dissertation, which was included in the scoping review.
Summary of Reviewed Studies.

Healthcare Providers Seen
Most of the studies reported help-seekers seeing either a general practitioner (GP) also known as a doctor or a primary care physician (15), ear, nose and throat specialist (ENT) also known as an otolaryngologist (13), or an audiologist (14). Others seen were health professionals offering psychological care or support (psychologist, counsellor or psychiatrist) (8), hearing therapist (7), nurse (3), audio vestibular physician (2), complementary therapist (2), specialist – not defined (2) and a physical therapist (physiotherapy) (1).
Measuring and Reporting Satisfaction
Most of the studies reported on the patient satisfaction of health professionals (19) and on the treatment effectiveness or satisfaction (13). The studies also reported on either referrals, services, procedures, and treatments offered or discussed with health professionals or the treatments tried by help-seekers (7). In this review one study was reported to use validated surveys to assess patient satisfaction for diagnoses and treatment. The surveys were The Patient Satisfaction with Communication (PSC) survey (Schofield et al., 2003) for diagnosis and the Functional Assessment of Chronic Illness Therapy–Treatment Satisfaction–General (FACIT-TS-G) survey (Webster et al., 2003) for treatment.
Treatments and Services
The most commonly reported tinnitus treatments provided by healthcare providers were educational/informational (explanation of tinnitus), audiological (sound enrichment using hearing aids, tinnitus masking device or sound devices) and psychological/counselling (psychological support or CBT) (Adams et al., 2012; Andersson & Edvinsson, 2008; Beukes et al., 2021; Bhatt et al., 2016; George & Kemp, 1991; Goldstein et al., 2015; Husain et al., 2018; Kim, 2018; Marks et al., 2019; McFerran et al., 2018; Naughton, 2004; The Royal National Institute for Deaf People [RNID], 2019; Sindhusake et al., 2003; West, 1999). Less often reported treatments were medication, surgical and medical procedures, relaxation/biofeedback/mindfulness, supplements or dietary recommendations and alternative therapies like acupuncture (Adams et al., 2012; Andersson & Edvinsson, 2008; Beukes et al., 2021; Bhatt et al., 2016; George & Kemp, 1991; Goldstein et al., 2015; Husain et al., 2018; Marks et al., 2019; McFerran et al., 2018; Naughton, 2004; The Royal National Institute for Deaf People [RNID], 2019; Sindhusake et al., 2003; West, 1999). Services included assessments such as audiometric assessment and or tympanometry, hearing tests and wax removal (McFerran et al., 2018).
In relation to help-seeking and receiving treatment, the studies reported that the level of help-seeking was lower in population samples compared with self-selected populations with the latter also reporting repeated help-seeking. The population sample studies reported that under half of the respondents with tinnitus sought help (30.3% (Sindhusake et al., 2003), 49.5% (Bhatt et al., 2016) and 43.5% (Carmody, 2016)). Four self-selected samples studies reported that the majority of respondents sought help from a health professional, (starting from 60% to 96%), (Carmody, 2016; George & Kemp, 1991; Husain et al., 2018; The Royal National Institute for Deaf People [RNID], 2019). One self-selected study reported that respondents saw a mean of 2.7 different types of health professionals (George & Kemp, 1991). Another study with self-selected participants reported repeated visits at primary and secondary care levels in order to gain referrals or treatments not given at initial stages of seeking help (McFerran et al., 2018). For the majority in population samples that sought help, most did not receive treatment, (over 84.8%), (Bhatt et al., 2016; Carmody, 2016; Sindhusake et al., 2003), even though hearing loss was higher in those with tinnitus and bothersome tinnitus was reported (16% reported tinnitus as extremely annoying (Sindhusake et al., 2003) and 7.2% reported it a big problem (Bhatt et al., 2016)). In the self-selected studies three studies reported that many respondents sought or tried more than one treatment, (from 40% to 70%), (Carmody, 2016; George & Kemp, 1991; Husain et al., 2018).
Accessing Specialist Care
In relation to accessing referrals and appointments, one self-selected sample study reported that the COVID-19 pandemic impacted on access to tinnitus care further reducing the already limited access, (Wray, 2021). A self-selected study reported that fewer people sought help for tinnitus from health professionals during the COVID-19 pandemic than before the pandemic (Beukes et al., 2021). Another self-selected sample study found that tinnitus impacted quality of life for some patients whilst they waited for appointments to specilaised tinnitus care (Wray et al., 2017).
Different Sample Categories and Patient Satisfaction with Services and Treatment
In relation to patient satisfaction and treatment effectiveness, one population study reported that of the 6% that had treatments, the majority of which (66.7%) reported those treatments as ineffective (Sindhusake et al., 2003) whilst 66.7% of those in a self-selected study reported they were dissatisfied with initial treatment (Carmody, 2016). The studies with self-selected participants reported barriers to care, negative counselling, a lack of information, no referrals, intervention or no treatment provided, ineffective treatments or long wait times and mixed reports of dissatisfaction and satisfaction with health professionals (Carmody, 2016; George & Kemp, 1991; Husain et al., 2018; McFerran et al., 2018; The Royal National Institute for Deaf People [RNID], 2019; Wray et al., 2017). Positive satisfaction ratings of services were reported when the health professionals were deemed helpful or patients received a referral or had an effective treatment (Beukes et al., 2021; George & Kemp, 1991; McFerran et al., 2018; The Royal National Institute for Deaf People [RNID], 2019; Wray, 2021). One study identified that patients wanted health professionals to have a positive approach when communicating about tinnitus to patients as it was likely to assist in coping with tinnitus (Beukes et al., 2021)
For patient satisfaction in the clinical/cohort samples the majority of respondents’ provided positive ratings of tinnitus services. One study found that patients were slightly more positive when rating the services from an audiology clinic than from an ENT clinic (97.5% and 74% respectively) (West, 1999). Most of the clinical/cohort sample studies presented mainly positive satisfaction of services from healthcare providers, (Goldstein et al., 2015; Kim, 2018; Sanchez & Stephens, 2000; West, 1999) however, some negative experiences were reported which included not being listened to or understood by the healthcare provider, not understanding what was being said, being spoken down to or a lack of information about tinnitus in consultation (West, 1999) or treatments not helping reduce tinnitus (Kim, 2018). Respondents also reported experiences of unnecessary distress and frustration due to negative views, lack of interest and information about tinnitus from healthcare providers when seeking initial help for tinnitus (Sanchez & Stephens, 2000). In one study, around half of respondents (46.5%) reported that treatment was unsatisfactory or they did not receive any treatment (Zarenoe & Ledin, 2014). Furthermore, another study found that the cost of care, repeated visits, age, sex, marital status, ethnicity, history of behavioural health treatment, sleep disturbances from tinnitus, any medication recommendation or dietary recommendations did not impact on the positive satisfaction with clinical services in a specialist tinnitus clinic (Goldstein et al., 2015).
For patient satisfaction in the interview/qualitative sample studies, respondents from three studies reported both positive and negative experiences along the tinnitus clinical pathway that impacted on their health care journey (Adams et al., 2012; Andersson & Edvinsson, 2008; Marks et al., 2019). Respondents in one of these studies perceived that there was no cure for tinnitus or nothing could be done for them; however, in the same study respondents also reported that they were reassured at being told nothing was wrong with them (Adams et al., 2012). Overall respondents reported concerns over dismissive health professionals, a lack of information and support, no or ineffective treatments and long wait times to specialists (Adams et al., 2012; Andersson & Edvinsson, 2008; Marks et al., 2019; Naughton, 2004; Pryce et al., 2018; Redmond, 2010). One study in particular reported that more respondents were dissatisfied than satisfied with health professionals; >50% reported GPs were unhelpful, >50% were unsatisfied with audiologists with a minority dissatisfied with ENTs (Redmond, 2010). Another study reported more respondents were dissatisfied with ENTs (around half) than GPs (33.3%) and audiologists (15%) (Naughton, 2004). The same study reported more respondents were dissatisfied with treatments than satisfied, of the 23 who reported using hearing aids or a ‘masker for tinnitus,’ 21.7% were satisfied and 30.4% dissatisfied (Naughton, 2004). Both studies reported psychological care to be of benefit to the few respondents that accessed it (Naughton, 2004; Redmond, 2010).
Factors Related to Help-seeking and Patient Satisfaction
Two studies measured the possible factors associated with help-seeking for tinnitus. One study found that those more depressed by their tinnitus saw significantly more health professionals as did those with more problematic tinnitus (George & Kemp, 1991). The other study found that help-seeking was also shown to be significantly related to tinnitus severity and how bothersome the tinnitus was (Beukes et al., 2021). Four studies measured the factors possibly associated with patient satisfaction. In one study the type of health professional seen either an ENT or audiologist was shown to influence the patient satisfaction with services (West, 1999). The other study measured possible associated factors such as age, number of clinic visits, associated costs, sex, marital status, ethnicity, history of behavioural health treatment, reported sleep disturbances due to tinnitus, medication recommendations or dietary recommendations and none of these factors were found to impact on patient satisfaction (Goldstein et al., 2015). In the third study no significant differences were found between patient satisfaction (diagnosis and/or treatment) for type of samples used, sex, hearing loss, medication, health provider seen, anxiety, depression, tinnitus distress or health status, nor was diagnosis satisfaction linked to treatment satisfaction (Carmody, 2016). The final study of benefits and shortcomings of a specialised tinnitus clinic assessed factors such as group status (group 1 being previous patients who first attended the clinic more than 18 months prior or group 2 more recent patients or during the course of the study) and sex (Sanchez & Stephens, 2000). The study found significant differences for group status for benefits volunteered for fitting of the tinnitus masker, reduced stress and worry, coming to terms with tinnitus and moving on (Sanchez & Stephens, 2000). A significant difference was also found for shortcomings for “tinnitus persists” volunteered by 16.3% of group 1 compared with 1.5% of group 2 (Sanchez & Stephens, 2000). The study also found significant differences for sex, for males it was hearing aid provision and for females less stress and worry and having a more positive attitude or feeling less depression (Sanchez & Stephens, 2000).
A study omitted from this scoping review showed that the type of treatments undertaken in a specialist tinnitus clinical setting may impact on patient satisfaction (Aazh et al., 2016). The study did not meet the inclusion criteria as it included data from children that could not be separated from the adult data, however, it does provide insight into the satisfaction ratings of treatments. The clinic received positive ratings from the patients overall (effective 36.4% or very effective 55.7%) (Aazh et al., 2016). Satisfaction with education, counselling and CBT was rated significantly higher than for devices such as hearing aids and noise generators (Aazh et al., 2016).
Discussion
The objective of this scoping review was to understand the extent and type of evidence in relation to seeking help for tinnitus and satisfaction with healthcare providers including diagnosis, clinical services, and treatments. All the studies included reported on one or more aspects of help-seeking for tinnitus and patient satisfaction with either diagnosis, clinical services or treatment effectiveness along the tinnitus clinical pathway provided by healthcare providers.
The studies in this scoping review were categorised according to the nature of study sample, representing the general population (population samples), people more negatively impacted by tinnitus (self-selected samples), those accessing help in specialist tinnitus clinics (clinic/cohort samples), and those assessing the experiences and themes that arise on the tinnitus journey (interview/qualitative studies). Each of the categories of samples used provided a different perspective of the help-seeker experience along the tinnitus clinical pathway. There were more respondents in self-selected samples who reported seeking help for tinnitus than those in the population samples, reflecting the way in which participants are recruited into studies. Population samples are more likely to include those for whom tinnitus burden or distress is low.
Help-seeking Experiences
Some of the common outcomes identified by this scoping review were that help-seekers reported being negatively impacted by their tinnitus, (Beukes et al., 2021; George & Kemp, 1991; Wray et al., 2017) that obtaining referrals for problematic tinnitus could be difficult, (McFerran et al., 2018; The Royal National Institute for Deaf People [RNID], 2019) that help-seeking was repeated until a referral or treatment was received (George & Kemp, 1991; McFerran et al., 2018) and that there were long waits to access specialist tinnitus care (Andersson & Edvinsson, 2008; Naughton, 2004; Redmond, 2010; Wray et al., 2017). The initial interactions with healthcare providers when first seeking help for tinnitus were reported to impact either positively or negatively on the perception of tinnitus and the clinical journey experiences (Marks et al., 2019; Pryce et al., 2018). Help-seekers were seeing GPs, audiologists and ENTs, as recommended by many of the guidelines for the management of tinnitus (Fuller et al., 2017; Langguth et al., 2007). However, help-seekers appeared not to be receiving the help or intervention that they required or had to repeat help-seeking to obtain it (Carmody, 2016; George & Kemp, 1991; McFerran et al., 2018). This repeated help-seeking occurred at primary care and secondary care levels, (McFerran et al., 2018) highlighting that some GPs and specialists could be a barrier to specialist tinnitus services (El-Shunnar et al., 2011; Gander et al., 2011).
Patient Satisfaction
Participants reported dissatisfaction with the lack of information/education, dismissive attitudes or negative counselling, not being offered help for tinnitus, having unsuccessful treatment (George & Kemp, 1991; Sindhusake et al., 2003) or no treatment at all (Carmody, 2016; George & Kemp, 1991; Newall et al., 2001; Sindhusake et al., 2003; Zarenoe & Ledin, 2014). Where patients had access to a specialist tinnitus clinic, the majority of participants reported more positive experiences and satisfaction with the provider of the specialised care, services and treatments, (Goldstein et al., 2015; Kim, 2018; Sanchez & Stephens, 2000; West, 1999) in contrast to more negative experiences reported more frequently from interactions with other providers e.g. GPs, ENTs and audiologists (Carmody, 2016; Husain et al., 2018; Naughton, 2004; Redmond, 2010; Wray et al., 2017).
Help-seeking and Patient Satisfaction for Other Chronic Health Conditions
Studies on help-seeking for chronic conditions such as back pain, insomnia and migraine have reported similar barriers upon seeking help and reasons for patient (dis)satisfaction to those found in this review. Help seekers for these other conditions reported no physical examination, (Verbeek et al., 2004) greater satisfaction from allied health professionals rather than GPs, (Butler & Johnson, 2008; Verbeek et al., 2004) lack of knowledge of effective treatments, (Benca, 2005; Bigal et al., 2008) uninformed in regards to referrals, (Cheung et al., 2014) reluctance to provide recommended care or treatment (Bigal et al., 2008; Dodick et al., 2016) and incorrect diagnosis (Dodick et al., 2016). These studies all highlight the difficult process faced by people with chronic conditions to obtain a diagnosis and an informed approach to management of the condition. Satisfaction is more likely to be achieved from specialised clinics providing tailored services.
Healthcare Provider Perspective
Studies surveying health professionals who provide services for tinnitus mainly GPs, ENTs and audiologists show that there is a need for appropriate adherence of healthcare providers to tinnitus guidelines, improved access to specialised tinnitus assessment, tinnitus management or treatments and access to tailored psychological tinnitus care (El-Shunnar et al., 2011; Gander et al., 2011; Hall et al., 2011; Hoare et al., 2012, 2015; Kochkin & Tyler, 2008; McFerran et al., 2019; Redmond, 2010; Sheppard et al., 2022). A survey of members of the British Tinnitus Association (BTA), which included individuals with tinnitus as well as health professionals working with tinnitus patients, identified a number of uncertainties in tinnitus assessment, diagnosis and treatment along the clinical pathway (Hall et al., 2013). The study recommended that an increase in clinical trials and research was needed to address both the needs of the patients and the concerns of health professionals in the National Health System (NHS) in England (Hall et al., 2013).
Additional research on tinnitus healthcare systems from clinician/expert opinion has found that when comparing different healthcare settings i.e. countries and regions across Europe these healthcare structures varied significantly (Cima et al., 2020). Other major significant differences where the use of definitions of tinnitus, beliefs regarding tinnitus patient characteristics, assessment procedures used by clinicians and accessibility of treatments for patients (Cima et al., 2020). There were also differences in regions on who to seek help from i.e. GP first or to a specialised tinnitus clinic (if known) or available, also whether going to a GP was necessary in the first instance and having a lack of knowledge of referral patterns or awareness of who to refer to if specialised tinnitus clinics existed there (Cima et al., 2020). These findings indicate the importance of knowing the referral pathway for tinnitus (Cima et al., 2020). Knowing the referral pathway is necessary for clinicians and the research suggests to incorporate this in the European tinnitus guidelines to address the clinician lack of knowledge (Cima et al., 2020) therefore further assisting those seeking help for tinnitus.
Clinical Guidelines for Tinnitus
This scoping review shows that most dissatisfaction with and barriers to receiving help for tinnitus occur at the initial stages of the clinical journey, and that satisfaction increases once patients access specialised care or a tinnitus clinic. This suggests that healthcare providers should be encouraged to provide information about and/or referral to specialised services in the initial appointment. Help-seeking experiences at the initial stages of seeking care informs and influences how those with tinnitus manage and whether they seek and or receive further help. The application of clinical guidelines and recommendations addressing diagnostics, assessment, referral, management and treatment of tinnitus along clinical pathways by practitioners is required to intervene at the initial and or vulnerable stages of seeking help for tinnitus (Fuller et al., 2017; Langguth et al., 2007).
A number of the reviewed studies used clinical practice guidelines to inform on their research (Bhatt et al., 2016; Husain et al., 2018; McFerran et al., 2018; Wray, 2021). A preliminary study by the British Tinnitus Association (BTA) reported on the satisfaction with GPs before and after the publication of latest NICE guidelines (2020) were introduced in the NHS for tinnitus patients, the report showed that after the guidelines were introduced there was a reduction in the reporting of GPs negatively counselling tinnitus patients. (Wray, 2021). Bhatt et al., 2016 examined the data before and after the implementation the American Academy of Otolaryngology–Head and Neck Surgery Foundation (AAO-HNSF) multidisciplinary clinical practice guidelines (Tunkel et al., 2014). They showed that the management options outlined by the AAO-HNSF guidelines were not followed consistently, with most interventions infrequently discussed: hearing aids (9.2%), wearable (2.6%) and non-wearable (2.3%) masking devices, and cognitive behavioural therapy (0.2%). On the other hand, medications were discussed in 45.4% of instances, as recommended by the AAO-HNSF guidelines even though few drugs have been shown to alleviate tinnitus (Ahmad & Seidman, 2004; Cederroth et al., 2018; Langguth et al., 2009). McFerran et al. acknowledges the development of a number of guidelines in recent years, which include the Department of Health (UK) guidelines best practice guide in 2009, the AAO-HNSF (US) clinical practice guidelines and more recently the National Institute for Health and Care Excellence (NICE) (UK) clinical knowledge summary (accessed in 2017) (McFerran et al., 2018) (this has been updated to the Tinnitus: assessment and management guide and published in 2020) (Wray, 2021). However, despite these guidelines, many help-seekers still report dissatisfaction with tinnitus services with negative counselling occurring at primary and secondary levels of care (McFerran et al., 2018). Husain et al. examined satisfaction with tinnitus services in the US and 70% of healthcare providers were audiologists (Husain et al., 2018). The American Academy of Audiology (AAA) provides audiology guidelines on the diagnosis and management of tinnitus patients (Husain et al., 2018). Patients reported they were advised that nothing could be done, they were not given information about tinnitus and majority of patients rated healthcare provider treatment or management of tinnitus as ineffective (Husain et al., 2018). For these reviewed studies it suggests that at primary and at specialised levels of care guidelines are not always followed. There could be many reasons for this, for example a lack of available services (Gander et al., 2011) or a lack of awareness of what is available for patients (Cima et al., 2020).
The TINNET initiative on establishing multidisciplinary European guidelines for tinnitus including diagnostics, assessment, treatment options, referral pathways, patient information and support based their criteria on a systematic review by Fuller et al., 2017 (Cima et al., 2019; Fuller et al., 2017). The five documents included were the national clinical practice guidelines from Denmark (Jørgensen et al., 2007), Germany (The Association of the Scientific Medical Societies, 2015), Sweden (Idrizbegovic et al., 2011), The Netherlands (Nederlandse Vereniging voor Keel – Neus – Oor heel kunde en Heelkunde van het Hoofd – Halsgebied, 2020) and the USA (Tunkel et al., 2014). All but one of the guidelines (Sweden) provided information and referred to the research literature associated with the particular recommendation (Cima et al., 2019; Fuller et al., 2017). Based on the recommendations of these guides on the clinical care of tinnitus they all agree that an audiological assessment be performed and that a validated survey be used to determine the degree of tinnitus distress (Fuller et al., 2017). All but one guide (Germany) recommended referring on to psychological or psychiatric care should the tinnitus distress be more severe and impacting on quality of life (Fuller et al., 2017). For treatment and management of tinnitus the recommendations of all guides provided information about tinnitus and treatment options for patients and using hearing aids only when patients also experienced hearing loss (Fuller et al., 2017). All of the guides except for the one from Denmark recommended CBT, three of which (Germany, The Netherlands and the USA) recommended specialised CBT for tinnitus and one (Sweden) recommended CBT for co-morbid anxiety or depression (Fuller et al., 2017). By following these recommendations, health professionals should be able to at minimum help the patient identify if hearing loss is present or possibly other ear based issues or refer on to get this assessed, ascertain the level of tinnitus distress using a validated survey, provide a referral to psychological care or CBT based tinnitus therapy and or management of tinnitus.
Recommendations and Future Directions
The use of appropriate guidelines at primary care level for GPs and healthcare providers is recommended to inform on referrals on to specialised care. These guidelines also provide evidence-based advice on the diagnosis of tinnitus, and potential interventions such as hearing aids, and psychological therapies. Additionally, those with tinnitus should be encouraged to persist with help-seeking, particularly in the face of being negatively counselled, or not being referred for specialist help from audiologists or ENTs.
Patient satisfaction is a growing area of research, but currently there is no standard way of measuring help-seeking or patient satisfaction in tinnitus research and in health science (Batbaatar et al., 2017; Verbeek, 2004). However, there are validated surveys that can be used to measure different aspects of patient satisfaction or clinical settings. For example, for patient satisfaction of a therapy for a chronic illness, the Functional Assessment of Chronic Illness Therapy scales would be a suitable choice for chronic conditions like tinnitus (Webster et al., 2003) and for measuring clinic or hospital settings the Australian Hospital Patient Experience Question Set (AHPEQS) would be suitable (Jones et al., 2021). In this scoping review the majority of studies reported their findings using unvalidated questions, and they did not assess the possible associated factors with help-seeking or with patient satisfaction. Further investigation on what factors motivate help-seeking, the type of health professional seen for the tinnitus whether it be a GP or specialist (ENT or audiologist) and type of treatments undertaken, either education, psychological or audiological that may impact on patient satisfaction, is recommended.
Limitations
As this was not a systematic review of the literature on seeking help for tinnitus and the satisfaction with the clinical experience including diagnosis, clinical services and treatment provided by healthcare providers we did not make any conclusions about the quality of the studies applying measures on either help-seeking or patient satisfaction. The inclusion criteria of the scoping review were limited to published and unpublished original studies in English. Although this did include studies conducted in non-English speaking countries published in English, care should be taken in generalising the findings to other countries and settings. This scoping review included only adults with tinnitus and excluded studies with data on childhood tinnitus. Finally, the number of studies on this research topic was limited.
Conclusions
The research suggests that although those seeking help for tinnitus found their way to a healthcare provider, it was unlikely for most help-seekers to be satisfied with the initial experience. It was also unlikely that help-seekers received a referral to a specialist at the initial consultation with a GP. Of the small group that received treatment, most reported that it was either unsatisfactory or ineffective. However, once help-seekers were in a specialised tinnitus clinical setting they were more positive with their satisfaction ratings of healthcare providers, services, procedures, and treatments. Positive and negative experiences impacted on the healthcare journey of those seeking help for their tinnitus and it shaped their perceptions of tinnitus and future interactions with healthcare providers. More positive approaches to communicating the tinnitus diagnosis and referrals to specialised tinnitus care would help patients in their journey of adjusting to tinnitus.
Supplemental Material
Supplemental Material - Seeking Help for Tinnitus and Satisfaction With Healthcare Providers Including Diagnosis, Clinical Services, and Treatment: A Scoping Review
Supplemental Material for Seeking Help for Tinnitus and Satisfaction With Healthcare Providers Including Diagnosis, Clinical Services, and Treatment: A Scoping Review by Natalie Carmody, Robert H. Eikelboom, and Susan Tegg-Quinn in Evaluation & the Health Professions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.