
Abstract
Introduction:
Families and friends of homicide victims (FFHV) interact with healthcare systems almost immediately after the traumatic event. Their interactions with healthcare providers can either facilitate healing, have a neutral effect, or compound an already painful experience. When trauma victims are admitted to the hospital, resources are necessarily diverted on their behalf with less consistent attention paid to their families and friends. The interactions surrounding the immediate circumstance as well as experiences in the weeks to months after can have significant long-term impact. This study explores the needs and experiences of FFHV when interacting with the healthcare system to inform physicians’ and providers’ interactions and provision of services.
Methods:
This study of 3 focus groups sought to understand these experiences with the healthcare system to better inform physicians’ and providers’ interactions and provision of services.
Results:
Using the framework approach, the study ultimately built upon the existing trauma-informed care (TIC) framework to include several emergent themes. Participants discussed the need for death notification sensitivity, benefits of coordinated care, barriers to accessing care, the need for physician empathy and attention, the lack of trauma screening, and hastily prescribing medications.
Conclusion:
This TIC approach can inform future healthcare interactions with the FFHV as it grounds the patients’ experience in their historical reality and may improve future provider-patient relationship.
Keywords
Introduction
In the aftermath of a murder, families and friends of homicide victims (FFHV) are secondary victims, exposed to immense trauma which often manifests as physical and psychological health consequences. 1 As the victim’s needs take precedence, families and friends often melt into the background of the event and the medical response to it. However, the immediate impact can have long-standing consequences to the FFHVs’ physical and psychological health and wellbeing.1-6
Emerging research provides a biochemical basis for effects of trauma on patients including alterations in the functioning of the limbic system and of endogenous opioid systems, hypothalamic-pituitary-adrenal axis changes involved in cortisol secretion, and neurotransmitter-regulated dysfunction of the parasympathetic and sympathetic nervous systems.7-11 Trauma significantly contributes to impacts from adverse childhood experiences (ACEs), allostatic load, and chronic health conditions.12-14 “Common physical disorders and symptoms include somatic complaints; sleep disturbances; gastrointestinal, cardiovascular, neurological, musculoskeletal, respiratory, and dermatological disorders; urological problems; . . . substance use disorders;” (p.64) 11 ; and somatization, prominent in this population, where emotional dysregulation is manifest in physical symptoms.11,15-19
Given the potential for exacerbating an already traumatic event, consideration to the unique needs of FFHVs requires a sensitive and nuanced approach. The importance of integrating compassion in all patient interactions is increasingly being recognized. Patients who receive compassionate, patient-centered care have been shown to have superior clinical outcomes, improved compliance with medication regimens, and lower healthcare costs whereas the lack of compassionate care is associated with increased medical errors and poor quality of care.20,21 Compassionate patient care can decrease provider burnout and healthcare costs; for example, improved communication with patients can reduce diagnostic testing expenses.22-24
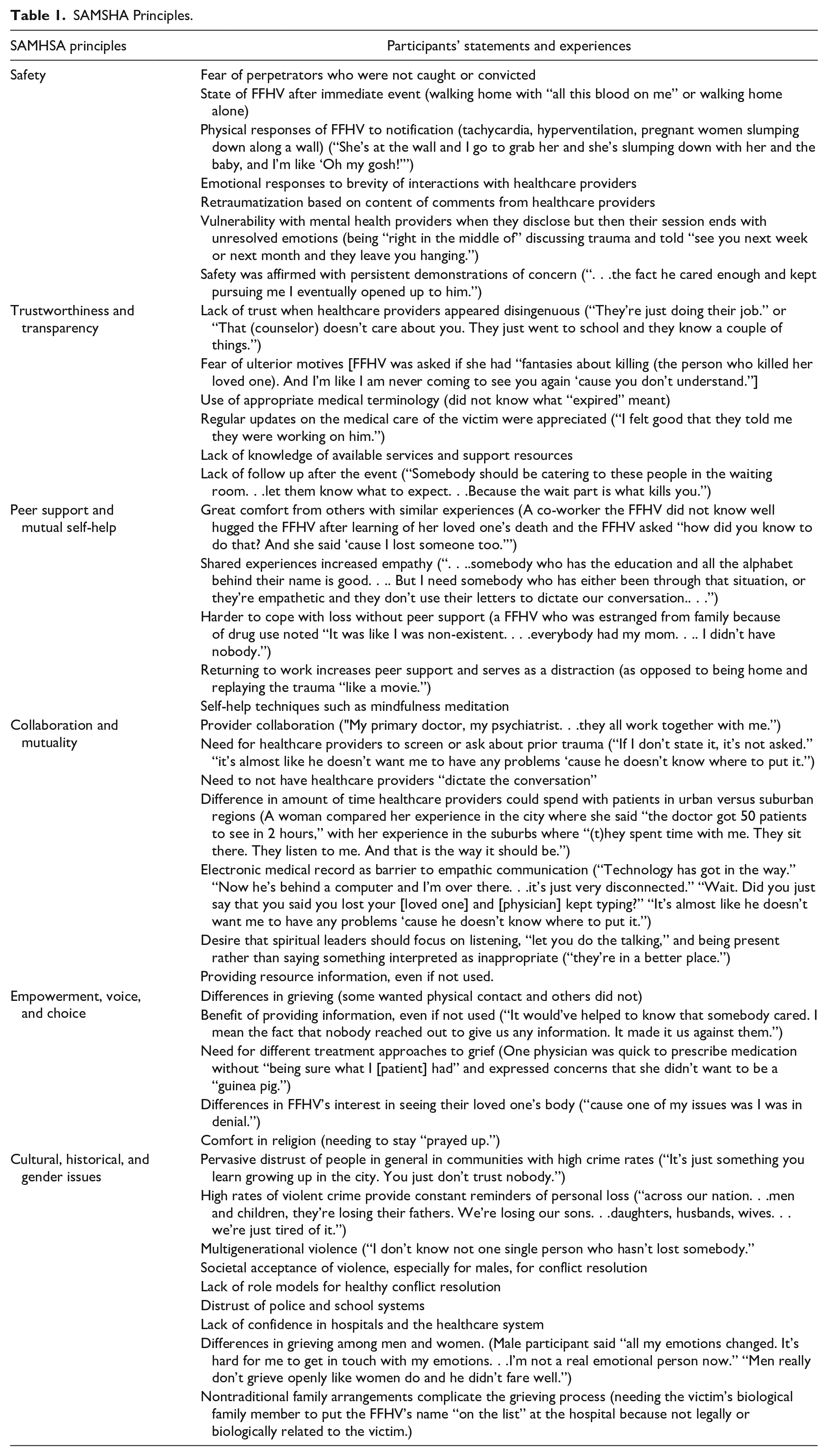
Using principles from trauma-informed care (TIC) models can provide a basis for understanding care delivery and optimal interactions. TIC refers to a systematic response to trauma, based upon the events, experiences, and lasting effects of trauma. While a wide array of trauma and trauma-specific interventions exist, SAMHSA developed 4 assumptions and 6 principles central to implementing care in a trauma-informed manner. The assumptions are that systems supporting those with traumatic events need to realize the impact; recognize the signs and symptoms; respond appropriately; and resist retraumatization. 25 These assumptions led to the 6 principles of Substance Abuse and Mental Health Services Administration’s (SAMHSA) Trauma-Informed Care (TIC) used as the coding framework for this study: safety; culture, historical and gender issues; empowerment, voice, and choice; collaboration and mutuality; peer support and mutual self-help; and trustworthiness and transparency (p. 10) (Table 1). 25 Addressing the underlying needs of this unique population may render future delivery of care more successful.
SAMSHA Principles.
Methods
This qualitative study explores the needs and experiences of FFHV when interacting with the healthcare system to inform physicians’ and providers’ interactions and the availability and provision of services. The study utilized focus groups which allowed for the reflection and discussion of individual and shared beliefs, opinions, and social realities. 26 This study used community-based participatory research, which aims to include community members, researchers, and organizational representatives in the research process. 27
Participants
Participants self-selected in all focus groups, advertised through flyers distributed and publicly posted at health organizations, educational institutions, places of worship, and social service agencies as well as to community leaders.
All study participants met the inclusion criteria of being 18 years of age or older, having a family member or friend killed by homicide, and having an inactive case, defined as being adjudicated by means of a trial or plea or unsolved for at least 6 months with little to no investigative activity. Interested participants were provided a phone number to call and were screened for eligibility by a research team member. Eligible individuals selected 1 of 3 scheduled focus groups to attend.
The sample consisted of 11 participants in 3 focus groups held in NJ and PA in 2018. Most participants self-identified as female (n = 8) and the average age was 46.7 years old. Six participants self-identified as Black, 4 as Hispanic, and 1 as Other. Nearly half the participants were single (n = 5), with 3 each indicating they were divorced/separated or married/partnered. Most participants were employed full time outside the home (n = 8) and 3 were unemployed. One completed some high school, 2 graduated from high school or had a GED, 2 graduated from college, and 2 completed graduate or professional schooling.
Participants provided information about their loved ones who died. There were 12 victims as 1 participant had 2 loved ones killed. The victims were almost all male (n = 11) and mostly Black (n = 8). The race of the rest of the victims was identified as other. The average age of the victims was 26.5, and half the victims were children of the participants (n = 6). The remaining victims were identified as spouse/partner (n = 2), friend (n = 2), sibling (n = 1), and cousin (n = 1).
Rowan University’s Institutional Review Board approved this study under IRB number Pro2018002311. The research team collaboratively created a field guide, to assist with data fidelity and to limit bias, 28 by group consensus and prepared for each focus group via conference calls and emails. The field guide included prompts to guide focus group discussions, which included asking participants to share about their loved one, the impact of the homicide on themselves and those around them, their experiences with various response systems and resources, and services that should be created to benefit FFHV.
The focus group facilitators were experts in the social work and criminal justice fields. Focus groups were held in secure, private locations, and participants were provided a $25.00 gift card. All focus groups were about 3 h and audiotaped. A third-party transcription service was engaged to transcribe all audio recordings.
Data Analysis
The research team read transcriptions of the focus group audiotapes to ensure accuracy and confidentiality of each participant. The research team members who analyzed the transcripts provided a variety of perspectives including academics and practitioners in mental health, medicine, victimology, social work, and law. Absent a team member who screened participants for eligibility, no member of the analysis team had prior interactions with participants.
The framework approach is a systematic qualitative method appropriate for multi-disciplinary qualitative health research. 29 Research team members first engaged in the familiarization step of the framework approach by identifying common themes from the focus groups. 30 After discussing the themes, the team members identified which themes were iconic of SAMHSA TIC framework. 25 (Table 1) SAMHSA provides detailed definitions of these themes that the researchers used when coding. As a summary: safety refers to physical and psychological safety; trustworthiness and transparency refers to working with transparency and the goal of trust building; peer support and mutual self-help seek to establish safety, hope, trust, collaboration, and to use one’s experience to promote healing; collaboration and mutuality stresses that relationships level power dynamics; empowerment, voice, and choice relates to building upon individuals’ strengths and experiences and supporting “shared decision-making, choice, and goal setting”; cultural, historical, and gender issues includes recognizing historical trauma, moving past stereotypes, and incorporating responses that meet individuals’ cultural, racial, and ethnic needs (p. 11). 11
Consistent with the emergent nature of qualitative research 31 and utility in using methodological approaches that answer research questions and address aims in a useful manner, 28 this study built upon the existing TIC framework by adding several additional themes that emerged in the findings: institutional trauma, re-traumatization, symptomatology, effect on family unit, coping, judgment, and learned helplessness.
The research team members then individually coded the transcripts by hand using the modified TIC framework, referred to as the “indexing” data analysis stage in the framework approach, 30 and then conducted several team conference calls in 2019 to analyze the transcripts and for coding consensus based on the framework. While there are various computer programs available for qualitative research, some researchers may prefer not to use such software to develop a more intimate knowledge of their data. 30 The inter-rater reliability ranged from 0.97 to 1.00 on the various themes. After 3 focus groups, the research team came to a consensus that we had met saturation, with no new themes emerging, and therefore collectively decided not to hold additional focus groups.
Results
Within the SAMHSA TIC framework, 25 participants stressed the importance of sensitivity during death notification, the benefits of coordinated care, and barriers to accessing care. There also were issues relating to interactions with healthcare providers, including rushing, sensitivity, and not giving patients their full attention, as well as lack of screening for trauma, hastily prescribing medications, and failure to follow up. Many participants expressed concerns relating to trust (Table 1).
While many of the themes aligned with the SAMHSA framework, 25 others required unique categorization, necessitating the creation of 7 new categories: institutional trauma, retraumatization, symptomatology (mental and physical), effect on the family unit, coping (both effective and ineffective), learned helplessness, and judgment (Table 2).
Additional Themes Identified in This Study.

One of the SAMHSA 25 assumptions is to resist retraumatization. The 2 additional emergent themes of institutional trauma and retraumatization from participants’ stories illustrate the myriad ways and multisystem levels in which participants’ trauma experiences occur and need to be addressed.
Discussion
It is estimated that, for every homicide death that occurs, 3 to 10 loved ones are impacted, roughly translating to 64,000 to 213,000 people annually in the United States.32-34 9% to 18% of the U.S. population are impacted by a loved one’s homicide during their lifetime with marginalized and disadvantaged communities, especially Black and Latinx communities, experiencing more violence and homicides.2,33-35 There are myriad health consequences for FFHV1-6,33 including: increased suicide ideation for immediate family members 2 ; 23.3% of immediate family members developing homicide related PTSD, which is over 3 times higher than the general population2,33; and prolonged or complicated grief, including 23% of adult FFHV experiencing this 2 years after the homicide of their loved one.33,36,37
Given the health consequences of homicide on families and friends, interactions with the medical community may have a long-term impact on FFHV. Limited research exists exploring the experiences of FFHV with healthcare providers and, to our knowledge, no study to date has done research with this population regarding a TIC framework. This study emphasizes the myriad ways in which experiencing the homicide of a loved one can permeate one’s health and/or behavioral health and impact one’s perceptions of interactions with the health system. It also suggests opportunities within these initial interactions to improve communication and potentially ameliorate long-term consequences. It is important to note that patients who are FFHV may have already experienced negative interactions with various response systems, institutional traumas, and socioeconomic barriers in their post-homicide journey. Awareness of this potential history should inform patient interactions. Empathy and psychoeducation about the effects of trauma would greatly benefit the interactions with FFHV. A trauma-informed approach emphasizing practitioner training on how trauma affects human beings, screening for trauma, appropriately responding to trauma, and providing appropriate resource information is key in these physician-patient interactions as is evidence-based training. 38
Common themes raised by participants that are relevant for healthcare providers include the limited amount of time per visit and often feeling rushed within that timeframe. Demonstrations of empathy seen as facilitating a healthy provider-patient relationship included not looking at the computer, acknowledging the homicide, repeatedly showing concern, and sharing resources, even if not used. Health professionals who were caring toward patients, actively listened, and expressed empathy and sensitivity to the patient’s needs were all of paramount importance. This is particularly relevant given individuals’ various responses to tragedy specifically around the amount of desired contact, both physical and emotional. Additionally, given that FFHV often noted feeling alone, isolated, and without resources or support, communication of support resources is a tangible and feasible intervention that hospitals and providers can offer.
Support groups and peers were noted to provide great comfort especially when members included other FFHV and members from the same community as the individual. Linking individuals with peer support can be especially valuable as some felt more distant and less at ease with healthcare professionals. Peer support may also be beneficial in overcoming isolation and generating greater levels of self-efficacy, empowerment, and engagement. Peers may be able to form a stronger therapeutic bond because they have dealt with the same struggles themselves. The mutual exchange of coping strategies is another important aspect of the peer-to-peer community.
Interactions that failed to acknowledge the homicide or threatened one’s psychological safety, to the extent the patient felt retraumatized, undermine trust in service providers and led to deterioration of that relationship. More globally, clinicians need to be sensitive to the pervasive distrust in communities of high violence toward both people in general and social institutions that have not always served their interests. Participants who noted having experienced institutional trauma in interacting with various response systems often discussed an “us versus them” or “streets against the system” mentality. While much of the institutional distrust is focused on the police and schools, some expressed cynicism about hospitals and physicians. Building a therapeutic relationship with FFHV must start with acknowledging the cultural and historical context of interactions and making continued efforts to support patients, even when resources are turned down the first time they are offered.2,33
In working with FFHV, providers must also not assume that a biological connection dictates a relationship nor that nontraditional family arrangements do not represent a significant bond since hearts and minds are not bound by blood relations. This research suggests that providers should continually engage our patients in conversations regarding past trauma, even if they are not immediately forthcoming, and should not minimize the often long-term impact of a traumatic event on an individual. Study participants recognized they had physical symptoms such as problems sleeping and eating, shortness of breath or chest tightness, and mental health conditions, such as depression and PTSD, directly related to the event. 33 However, other chronic conditions such as diabetes or hypertension, which can be related to chronic stress and allostatic load, were not consciously associated with the event. Thus, many more conditions may be exacerbated by the stress of the homicide. While the FFHV who participated in this study were particularly open and motivated to share their experiences and health consequences in the hopes of helping others, many other FFHV may not readily identify the connection between current health problems and prior trauma and open, sensitive dialog to continually engage them may be needed.
Additional individual level concerns were discussed, including variation in response to homicide based on gender, differing effects on the family unit, and coping techniques. Gender was shown to modify the manifestations of grief and was reflected in the effects on the family unit. Mothers commonly repressed sorrow to avoid unduly burdening their children with their grief. Children, even if very young, would suppress their emotional responses at home but then misbehaved in school, which was underappreciated as being associated with the homicide. Men also were noted to repress sorrow, finding stoicism, anger, or violent reactions as more culturally acceptable than grief. Other coping techniques differed among individuals. Support groups were seen more positively than counseling which was sometimes viewed as a sign of weakness. Many participants felt that attending the focus group was therapeutic in hoping to make a difference and in sharing their stories with others who had a similar experience. Many participants also felt it fulfilling to become advocates for change.
While limitations included a small sample size, the participants’ stories and experiences reflected consistent themes across the focus groups and the sample size is consistent with similar studies.39-43 The sample size allowed for a robust in-depth analysis of the shared experience of the homicide of a loved one, with saturation of themes reached with the 11 participants. The information provided is dependent on victim recall, a concern in such focus group studies; however, it is not uncommon for FFHV to clearly remember events with detail. 44 Even if not all details were recalled, the depth and detail of those recounted provided a rich, valuable picture of their experience. Although the generalizability of these findings is limited, the themes observed should be relevant for many FFHV as participants were from urban neighborhoods, which have higher homicide rates and most of the victims were young black males, a group disproportionately likely to be victims of homicide across the country.33,45 In addition, given the limited research in this area, the study provides a foundation for further replication.
Research should continue to explore evidence-based approaches in clinical settings on different communication styles and resource allocation both at the time of the event and in subsequent follow up. Such evidence should be incorporated into medical education and clinical practice. Those resources confirmed to be most efficacious should be codified and supported by policy decisions and budgetary allocations. Specific risks of vulnerable sub-populations should be assessed relative to the broader population and should include economic as well as physical health.
Conclusion
Given the number of people affected by homicide, this study highlights some of the health issues that FFHV are experiencing that physicians and providers may not be aware of. Training in TIC may make healthcare providers more comfortable in asking about the trauma and can provide physicians with tools to effectively unpack and appropriately refer patients in the limited time they have. While there is much to prioritize in the physician-patient interaction, appropriately assessing trauma can potentially result in: a decrease in unnecessary testing, an improved patient relationship, more effective diagnoses and referrals, and better patient compliance with treatment plans.
Footnotes
Acknowledgements
We presented preliminary findings for a Center for Victim Research sponsored webinar in August 2019. We thank all of the participants for being willing to share their stories with us. We thank Carolyn Gribbin for assisting in facilitating the focus groups and Sue Case for assistance with transcription services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Researcher-Practitioner Fellowship from the Center for Victim Research (CVR) under grant number 2016-XV-GX-K006, awarded by the Office for Victims of Crime, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this presentation are those of the contributors and do not necessarily represent the official position or policies of the U.S. Department of Justice.